
Abstract
Objectives:
Falls are an important cause of morbidity in older adults. Equine-assisted activities including therapeutic riding (TR) benefit balance and neuromuscular control in patients with neurological disabilities but have not been systematically studied in older adults at greater risk for falls due to balance deficits. The effect of an 8-week TR program on measures of balance and quality of life in community-dwelling older adults with established balance deficits was evaluated.
Design:
This was a pretest–post-test single-group trial of a TR program on measures of balance and quality of life.
Setting:
The study was conducted at a Professional Association of Therapeutic Horsemanship (PATH) International Premier riding center.
Subjects:
The subjects comprised 9 adults (5 female, 4 males) with a mean age 76.4 years (range 71–83 years).
Interventions:
This included an 8-week observation period followed by an 8-week TR program consisting of 1 hour per week of supervised horseback riding and an 8-week follow-up period. Subjects received balance testing at weeks 0, 8, 16, and 24 using the Fullerton Advanced Balance Scale (FABS), and quality of life was measured at weeks 8 and 16 using the Rand SF (short form) 36 quality-of-life measure.
Outcome measures:
Outcome measures were change in the FABS and Rand SF 36.
Results:
There was no significant difference in balance scores between the start and end of the observation period. There was a significant improvement in the balance score and perception of general health from the start to the end of the intervention period, and no significant difference between the end of the intervention and the end of study, suggesting that improvements may have been sustained.
Conclusions:
TR is a safe activity for older adults with mild to moderate balance deficits and leads to both improvements in balance and quality of life. Longer and larger studies to assess the benefit of equine-assisted activities on improvements in balance and reduction in fall risk are needed.
Introduction
Balance represents a complex interaction of sensory and musculoskeletal systems, and deficits in either can lead to falls. At any age, exercise leads to faster postural reflexes, improved balance and mobility, and fewer falls. This includes individuals with significant disabilities such as chronic stroke. 4 A Cochrane Database Review 5 of exercise and balance in older people identified 34 studies in which those who exercised showed statistically significant improvements in balance over individuals with usual activities. All types of exercise were represented in these studies including those involving gait, balance, coordination, and muscle strengthening, with combinations of multiple types showing the greatest improvement.
Hippotherapy (HPOT) and therapeutic (horseback) riding (TR) have become important methods of providing both a pleasurable activity and physical exercise for individuals with developmental and acquired disabilities. HPOT is defined as a physical, occupational, or speech therapy treatment strategy that utilizes equine movement, usually as part of an integrated treatment program to achieve functional outcomes. TR utilizes mounted activities including traditional riding disciplines or adaptive riding activities conducted by a PATH International (Professional Association of Therapeutic Horsemanship International, Denver, CO) certified instructor. Both are termed equine assisted activities proven to improve dynamic postural stabilization, muscle co-contraction, joint stability, weight shift, postural and equilibrium responses, and gross motor function in children with cerebral palsy (CP). 6,7 TR has also been shown to improve balance in individuals with mental retardation. 8 However, few systematic studies of the potential benefit of equine assisted therapies have been undertaken in older individuals. This article presents the results of a 10-week, single-blind, controlled study of a 10 TR program on two measures of balance in community-dwelling, older adults without selecting subjects specifically for balance deficits. In that study, we recorded improvements in balance in both the intervention (TR) group and active, healthy controls, both with relatively small balance deficits, emphasizing the need to study patients with greater established balance deficits. 9 In addition, safety of the intervention in an older age group was established.
Methods
The study was approved by the Bronson Methodist Hospital Institutional Review Board (Kalamazoo, MI). A convenience sample of individuals 65 years of age or older was recruited from the local community. All subjects gave informed consent, and underwent a health screening and a balance screening. The balance screening consisted of four questions (Short-Form Version) from the Fullerton Advanced Balance scale (FABS), a validated measure of balance deficit and fall risk (personal communication Debra J. Rose, PhD and reference 2). The full FABS (Table 1) is a test of static and dynamic balance and is especially suited to higher-functioning individuals with slightly more challenging tasks. It consists of 10 maneuvers scored from 0 to 4 (high to low fall risk) with a total possible score of 40 and takes approximately 20 minutes to complete. The FABS has also been found to have high test–retest (intra-rater) and inter-rater reliability. The short form version of the FABS consists of questions 4, 5, 6, and 7 of the full FABS with a total possible score of 16. A score of 9 or lower indicates a reasonable high probability of fall risk. Subjects otherwise meeting the entry criteria and scoring between 6 and 12 on the short form FABS were enrolled in the study. In addition, physician clearance was required of all subjects entering the study.
Each item is scored 0–4 with a possible total score of 40 (see reference).
Subjects were excluded with any chronic condition known to affect balance including history of stroke, Parkinson's disease, multiple sclerosis, vestibular dysfunction, or any other condition leading to severe musculoskeletal or neurologic dysfunction or impairment in balance. Additional exclusion criteria included history of intake of more than the equivalent of 1.5 ounces of alcohol per day, fear of horses, and recreational or therapeutic riding within 1 year of enrollment. Entry into the study was at the discretion of the physician investigator (DNH).
The FABS was administered to selected individuals at the time of entry into the study (week 0), just prior to starting the TR intervention (week 8), immediately upon completion of the TR intervention (week 16), and 8 weeks after completing the TR intervention (week 24) by a licensed and experienced physical therapist (CVS). In addition, each subject was asked to complete the Rand SF (Short Form) 36 quality-of-life survey at the start and end of the TR intervention (weeks 8 and 16). The Rand SF 36 is a validated tool using 36 questions that have been used to assess physical and emotional functioning in older adults. 10,11 Questions from the tool are combined to form nine domains corresponding to various quality-of-life indicators. These include physical functioning, role limitations due to physical health, role limitations due to emotional problems, energy/fatigue, emotional well-being, social functioning, pain, general health, and health change. Each domain has a possible score of 100.
Participants underwent balance testing and the TR intervention at the Cheff Therapeutic Riding Center (Augusta, MI). The Cheff Center is a PATH International premier accredited therapeutic riding center, established in 1970, that serves multiple types of clients including children and adults with physical, developmental, and psychologic disabilities including veterans with post-traumatic stress disorder, children and adults with autism, CP, and so on. The TR course consisted of a once per week, 1-hour session with a PATH-trained and certified TR instructor investigator (TDH or KMH). The TR session included grooming and tacking, mounting, a warmup exercise on the horse, riding skills, and dismounting. The riding portion of the session lasted approximately 45 minutes and consisted of walking and/or trotting, depending on the skill of the rider. One (1) to 3 volunteers assisted the rider to maintain safety. Close observation of the rider was maintained at all times for early detection of fatigue, discomfort, etc. The Rand SF 36 was administered at the start and the end of the TR intervention (weeks 8 and 16). Seven (7) subjects completed both measures.
Results
Eleven (11) subjects met the entry criteria and were enrolled in the study and 9 subjects (mean age 76.4 years, range 71–83 years, 4 male, 5 female) completed the TR intervention and all four balance measurements. Seven (7) subjects who finished the trial (mean age 76.1 years, range 71–83 years, 2 male, 5 female) also completed both measures of the quality-of-life questionnaire.
Mean balance scores at each study time point are shown in Table 2 and Figure 1. Comparison of balance scores between each time point in the study is shown in Table 3. As noted, there was no significant change in balance scores during the observation period (weeks 0–8, p=0.35). There was a significant improvement in balance scores from the start to end of the TR intervention (weeks 8–16, p=0.001), and no significant difference between the end of the TR intervention and the end of the follow-up period (weeks 16–24, p=0.908). The observation period was established to investigate and minimize the effects of learning on the balance tests as well as to gather information on daily physical activities of the participants. Most measures of quality of life improved from the start to end of the TR intervention; however, only the measure of overall perception of general health improved significantly (p=0.003) (Table 4, Fig. 2). No safety issues were encountered during the trial.
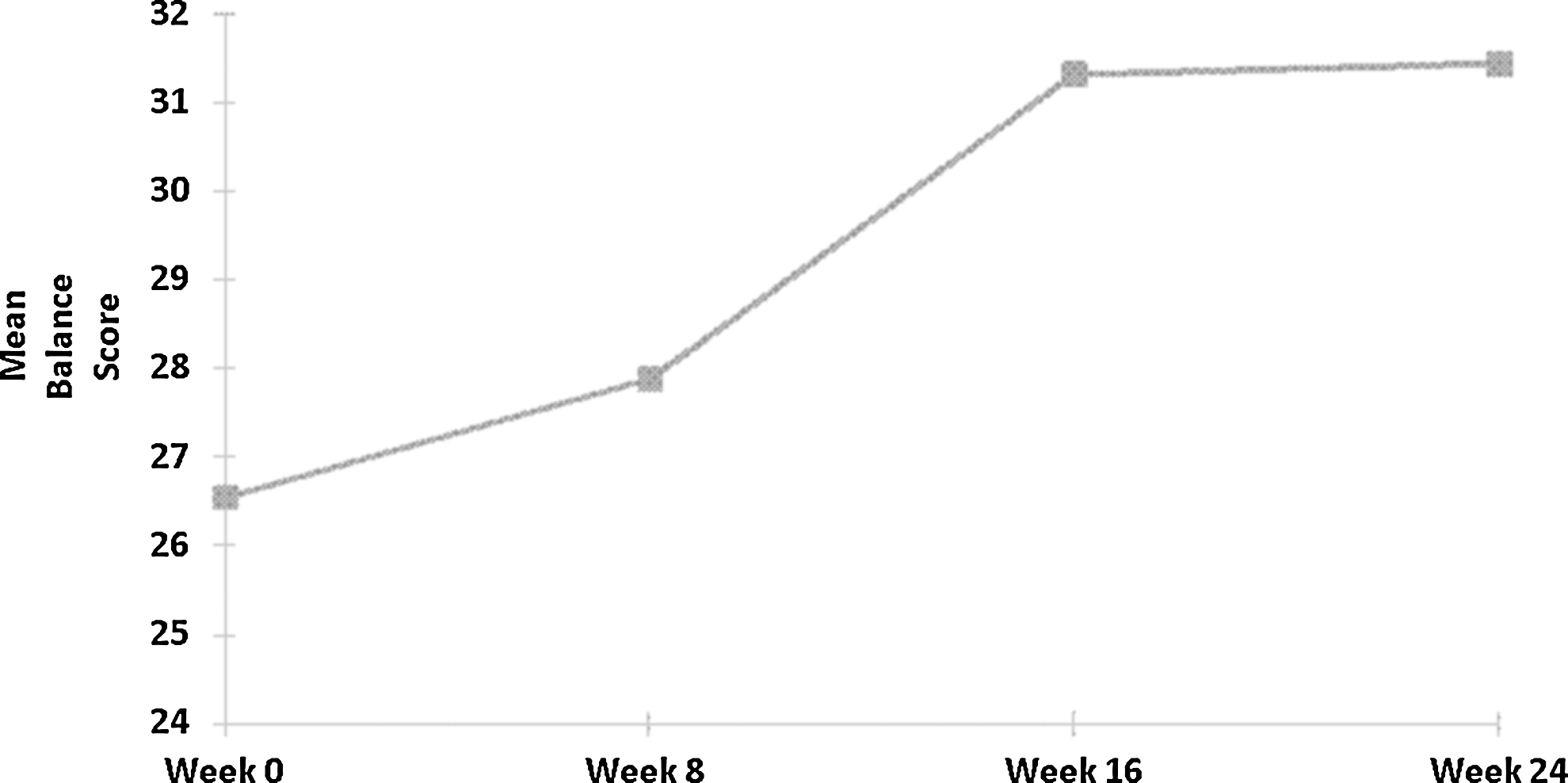
Mean balance scores at each time point.
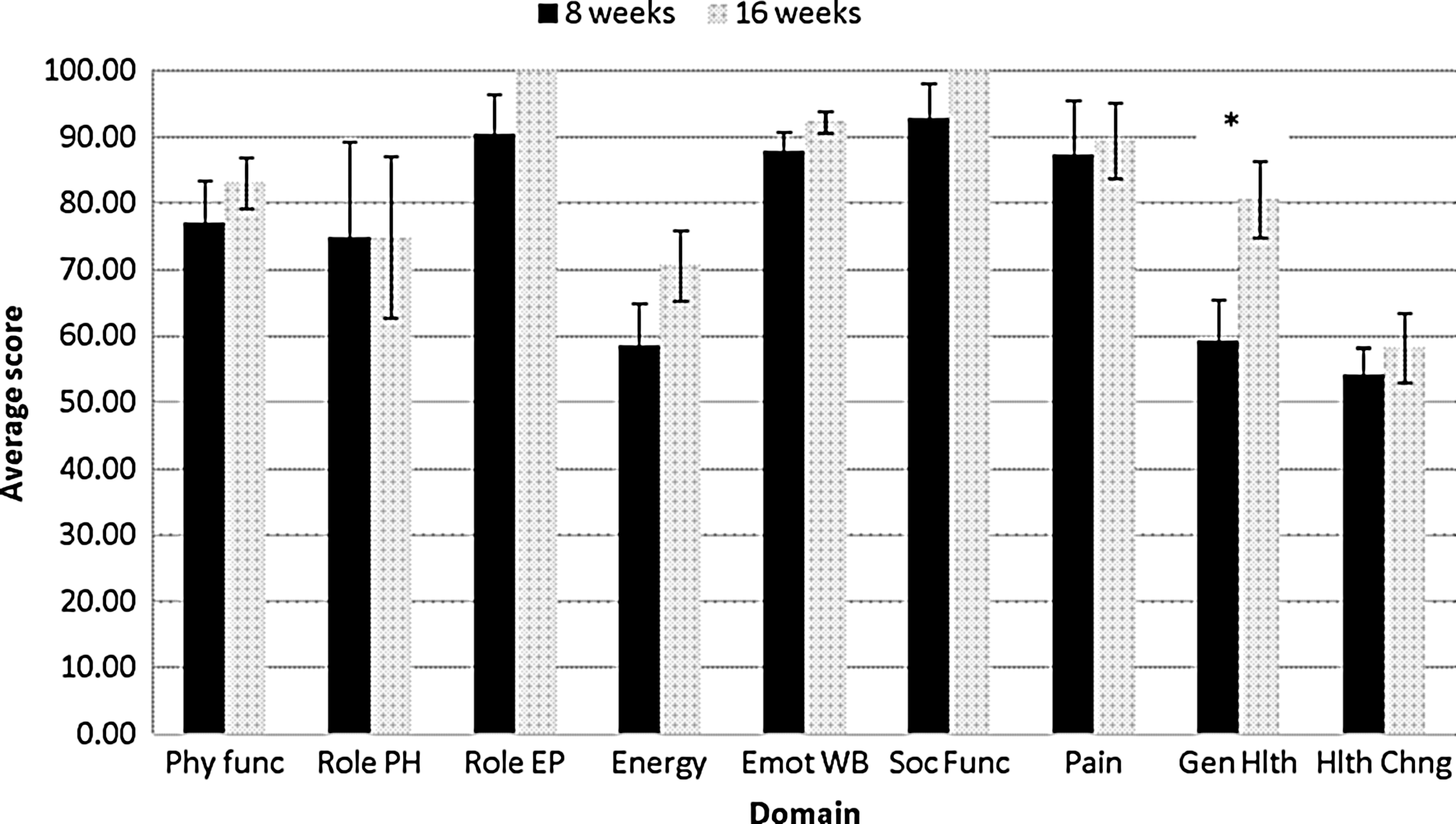
Quality-of-life measurements at 8 and 16 weeks. Phy Func, physical functioning; Role PH, role limitations due to physical health; Role EP, role limitations due to emotional problems; Energy, energy/fatigue; Emot WB, emotional well-being; Soc Func, social functioning; Pain, pain; Gen Hlth, general health; Hlth Chng, health change. *p = 0.022.
Sig., significance; df, degrees of freedom.
QOL, quality of life; Std., standard; df, degrees of freedom; Sig., significance; Phys func, physical functioning; Role PH, role limitations due to physical health; Role EP, role limitations due to emotional problems; Energy, energy/fatigue; Emot WB, emotional well-being; Soc Func, social functioning; Pain, pain; Gen Hlth, general health; Hlth Chng, health change.
Statistical analysis
Descriptive statistics for balance scores are shown in Table 2 and comparisons of the means at paired time points are shown in Table 3. The descriptive statistics for the quality-of-life measures are shown in Table 4 and comparisons of the means at paired time points in Figure 2. The paired t-test was used throughout as the measurements were taken on the same subjects throughout the study. The tests were conducted at a 0.05 significance level. Minitab 16 (Minitab, Inc., State College, PA) statistical software was used for the analyses.
Discussion
Falls are common in older individuals and have an important impact on quality of life. They are also expensive, with the cost of fall injuries reaching $20.2 billion in 1994 and estimated to increase to $32.4 billion in 2002, likely due to an increasing senior population as baby boomers age. 12 Factors that increase risk of falls include disability, poor performance on physical tests, depressive symptoms, poor executive function, concern about falling (balance confidence), and previous falls. 13 Identification of those individuals at risk and early intervention with medical assessment and management, exercise programs, and environmental modification is known to reduce fall risk and improve quality of life.
Exercise reduces fall risk in older adults. Nowalk et al. 14 demonstrated the benefits of two exercise programs, resistance/endurance training and t'ai chi, in reducing fall risk in residents of two long-term care facilities. Cyarto et al. 15 showed improvements in balance confidence and balance ability in independent-living retirement village residents undergoing either home-based resistance and balance training or group-based walking. In another study of relatively healthy community-dwelling adults age 65 and older, Feldenkreis exercises significantly improved mobility and balance confidence. 16 Disabled older adults also benefit from exercise programs. Miller et al. 17 achieved improvements in balance performance, balance confidence, and gait in debilitated, ambulatory community-dwelling adults undergoing 4 weeks of exercise and balance training. In addition, a recent Cochrane Database Systematic Review 18 of 111 clinical trials of fall intervention in older community-dwelling adults concluded that multiple-component group exercise, t'ai chi, and individually prescribed multicomponent home-based exercise all reduced fall risk and rates of fall.
HPOT and TR are not only forms of exercise with proven rehabilitative potential but also are pleasurable activities for those with disabilities. The exact therapeutic benefit of horseback riding is unknown is but thought to be due displacement of the horse's center of gravity three-dimensionally, leading to rhythmic movements similar to a human gait. 19 Neurosensory and neuromuscular responses are elicited from underutilized muscle groups in response to this mechanical stimulation. Although not yet defined, movement of the horse may also improve vestibular responses to alterations in posture, leading to improved fall protection in older individuals.
TR and HPOT improve muscle tone, balance, posture, trunk/head stability, upper extremity reach/targeting, gross motor function, and gait speed in children with CP. 19 –21 Balance and quality of life are also improved in multiple sclerosis with both TR and HPOT. 22,23 However, there are no systematic studies of the effects of TR or HPOT in older adults with any medical condition, including the effects on balance.
A total score on the FABS of 25 or lower has been determined to be a predictor of increased fall risk in older subjects. 2 Mean FABS score for the group in the current study at baseline was 26.5 and increased to 31.33 at the end of the TR intervention. This would indicate that these subjects had reasonable balance deficits at the start of the trial with clear improvement after completing the TR course. Of interest is the maintenance of the mean balance score at the follow-up measure and above the baseline balance score, suggesting persistence of effect, although no subjects continued to ride after completing the TR intervention. The subjects, however, were not queried as to whether they may have increased other physical activities during the follow-up period, possibly accounting for the apparent persistence of effect. The small sample size precludes any definite conclusions regarding this.
A control group was not used for this study, but rather a single-group pretest–post-test design was chosen to minimize the effects of other confounding variables such as other exercise in a comparison group. Sterba et al., 6 in discussing a study design for assessment of the effects of TR on children with CP, pointed out that using intervention subjects as their own controls was a sensitive way to determine small therapeutic changes. They felt that an interventional before–after trial with subjects serving as their own controls was useful for evaluation of effects on gross motor function in the evaluation of sports therapy. This may also prove true for balance studies involving exercise. Additional issues include determining optimal frequency and duration of TR or HPOT therapy for balance and what is the duration of a possible sustained effect once therapy is discontinued. Since falls and fall risk rather than balance per se are the ultimate clinically significant outcomes, a future study with a longer (perhaps 1 year) TR course while measuring not only balance but actual falls and fear of falling, perhaps compared to a nonintervention matched control group would clarify the true benefit of equine-assisted activities on reducing fall risk.
However, this study demonstrates the practicability, safety, and benefit on improvement in balance of a short-term TR course in older individuals with established mild-to-moderate balance deficits. As the general population ages, is generally healthier and more active than their parents, and desire to continue to undertake physical activities, equine activities and equine-assisted therapies may prove beneficial for maintenance of balance with resultant decrease in the fall risk and improved quality of life. Additional studies in this area would help clarify the benefits of this type of activity in older individuals.
Footnotes
Acknowledgments
All listed authors contributed significantly to the design, implementation, and reporting of results of this study. The statistical services of Robert Flikkema, MS, Department of Statistics, Western Michigan University, Kalamazoo, Michigan are greatly appreciated. Funding Source: The Cheff Therapeutic Riding Center.
Disclosure Statement
The authors do not indicate any conflicts of interest in regard to this study. Tamara D. Homnick, Kim Henning, and Charlene Swain are employed by the Cheff Therapeutic Riding Center. Douglas Homnick reports no financial interest in regard to this study. The Cheff Therapeutic Riding Center provided in-kind support of this project.