
Abstract
Study of complementary and alternative medicine's mind and body interventions (CAM-MABI) is hindered not only by the inability to mask participants and their teachers to the study intervention but also by the major practical hurdles of long-term study of practices that can be lifelong. Two other important methodological problems are that study of newly trained practitioners cannot directly address long-term practice, and that long-term practitioners likely self-select in ways that make finding appropriate controls (or a comparison group) challenging. The temporary practice pause then resumption study design (TPPR) introduced here is a new tool that extends the withdrawal study design, established in the field of drug evaluation, to the field of CAM-MABI. With the exception of the inability to mask, TPPR can address the other methodological problems noted above. Of great interest to investigators will likely be measures in practitioners of CAM-MABI that change with temporary pausing of CAM-MABI practice, followed by return of the measures to pre-pause levels with resumption of practice; this would suggest a link of the practice to measured changes. Such findings using this tool may enhance our insight into fundamental biological processes, leading to beneficial practical applications.
Introduction
Description of Withdrawal Study Design
In a randomized withdrawal trial, subjects receiving a test treatment for a specified time are randomly assigned to continued treatment with the test treatment or to withdrawal. “Any difference that emerges between the group receiving continued treatment and the group randomized to placebo would demonstrate the effect of the active treatment. The pre-randomization observation period on treatment can be of any length; this approach can therefore be used to study long-term persistence of effectiveness when long-term placebo treatment would not be acceptable.” 3 As noted above, in studies of CAM-MABI, placebos are usually not feasible, and thus randomization to withdrawal (called temporary practice pause then resumption [TPPR] in this article) or to continuation of the contemplative practice would be employed, with close monitoring. The randomized withdrawal study design is described and included as a valid methodology in the regulatory document “Choice of Control Group and Related Issues in Clinical Trials” of the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use. 4 This document represents official guidance from the U.S. Food and Drug Administration (FDA), as well as from the regulatory bodies analogous to FDA in Europe and Japan, to pharmaceutical manufacturers and developers. Therefore, the randomized withdrawal design or TPPR can adhere to rigorous methodological requirements for clinical research. An important advantage of this study design is that it allows in a relatively brief study the evaluation of characteristics that may have been affected by extended practice (perhaps years), such that a prospective study from onset of the practice would for practical reasons be difficult or infeasible. 3,4 For example, one might study whether a temporary practice pause impacts neural correlates of attention expertise in long-term meditation practitioners, thus addressing a typical caveat of cross-sectional studies. 5
Evidence of the practical clinical importance of this study design is apparent in that results from a controlled randomized withdrawal trial served as a basis for the FDA's approval in 2012 of the use of Vyvanse® (lisdexamfetamine dimesylate) for the maintenance treatment of attention deficit hyperactivity disorder in adults. 6 Another current example of this study design in a psychiatric condition is Astra Zenica's Multicenter, Double-blind, Randomized-Withdrawal, Parallel-group, Placebo-controlled Phase III Study of the Efficacy and Safety of Quetiapine as Monotherapy in the Maintenance Treatment of Patients with Generalized Anxiety Disorder Following an Open-Label Stabilization Period. 7 In addition, the randomized withdrawal study design has been employed in many other therapeutics areas including, but not limited to, cardiology, 8 rheumatology, 9 nephrology, 10 and pain control. 11
Resuming CAM-MABI Practice After Pausing
In the setting of the use of the TPPR study design in persons with established CAM-MABI practices, for ethical and scientific reasons resumption of the usual practice is a critically important element of the study design. Following the pause of practice (or “dechallenge”), resumption of practice would essentially constitute a “rechallenge”; dechallenge–rechallenge can be a useful approach to infer causality in pharmacoepidemiology and other disciplines. 12,13
Advantages of the Temporary Practice Pause Then Resumption Study Design
The TPPR study design is explained further below by contrasting with other CAM-MABI study designs to highlight some of its advantages. One commonly utilized CAM-MABI study design involves evaluation of novices undergoing an introductory CAM-MABI, with comparison to a group on a waiting list or to a group undergoing another type of training or education. To utilize this approach to study advanced practitioners from the time of their initiating practice would require years of training and monitoring, with great expense and likely many dropouts, rendering such a study rife with practical challenges and nearly impossible. In contrast, a TPPR study design could recruit more or less advanced practitioners, randomize them, and then monitor the evolution of the measures of interest as a function of pausing and then resuming practice, without the necessity of years of monitoring. In addition, another desirable feature is that the measurable attributes and skills acquired in introductory training are unlikely to be identical to those acquired after a longer duration of practice, and thus the withdrawal study design provides the possibility of observing correlates or effects of long-term practice that would not be observable in a study based on short-term training.
Another study design that has been used involves the comparison of advanced practitioners to nonpractitioners, with possibly a third group of less-advanced practitioners. An investigator who has employed this study design notes an important limitation: “Long-term training is something that might only be undertaken by an individual who is different to begin with. Unless we had measures at different points along the continuum of training, we could not disentangle training effects from the study of those individuals who are likely to persist in such training.” 14 The withdrawal study design can address this issue by undertaking to temporarily reverse the “continuum of training” in those who undergo pausing of their contemplative practice. In addition, because in this study design the individual is compared to his or her pre-pause self, the design controls for the likelihood that long-term training “might only be undertaken by an individual who is different to begin with.”
Measurable attributes in a group that are unaffected by pausing practice of CAM-MABI may reflect that the pause was not long enough to affect the measure, that the contemplative practice has no effect on the measure, that the measure had become fixed, that there were measurement problems, and so on. Of greater interest and more informative than measurable attributes that are unaffected by pausing practice will be measures that change in experienced practitioners who pause their CAM-MABI practice, while those who continue do not show changes. Measurable attributes may be investigated using neuroimaging, electroencephalography, physiologic testing, laboratory testing of specimens obtained from subjects, behavioral response tests, affective measures, and so on. When such changes are observed, they can be linked to the CAM-MABI. Moreover, confirmatory evidence for a link can be obtained by demonstration of reversion of the metrics to pre-pause levels with resumption of CAM-MABI practice.
Time Course of Findings: An Idealized and a Real Example
Figure 1 presents idealized data to illustrate simply how a TPPR study's findings could appear. Panel A in the figure shows a control subject who is randomized to continue his or her usual CAM-MABI practice. The metric of interest, shown on the y-axis, does not change. Panel B shows a subject who was randomized to pause practice for 10 days and then resume, and the metric of interest does not change, suggesting no link between the metric and the 10-day pause or resumption. Panel C shows a subject who was randomized to pause for 10 days and then resume, and the metric of interest shows a constant monotonic increase with onset of the pause and then reversal with resumption of practice. This indicates a clear correlation between the study interventions and the metric of interest. Panel D indicates a pattern similar to Panel C; the main difference is that in Panel D there is a several-day lag between the onset of the pause, or of the resumption, and the associated change in the metric of interest.
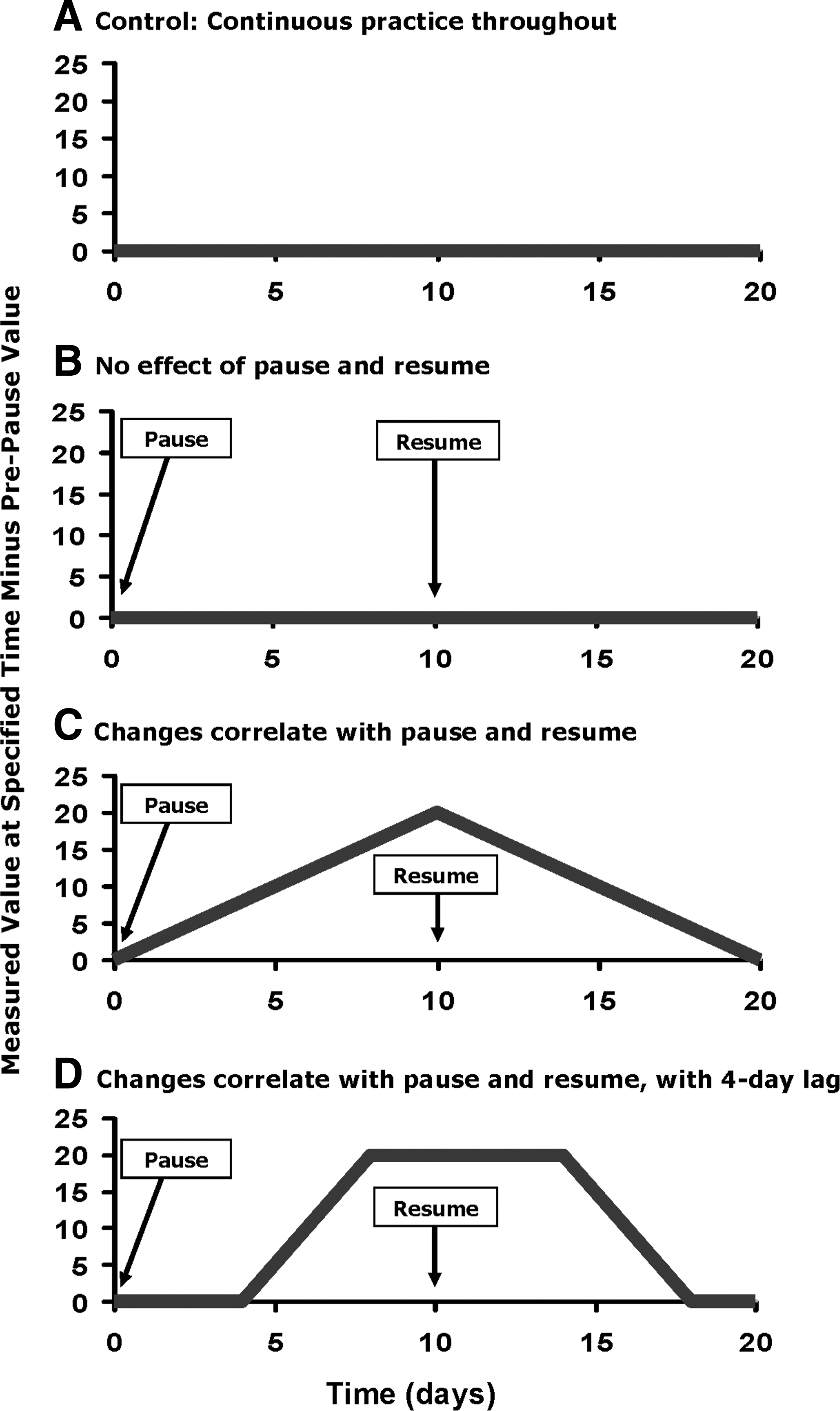
Idealized data to illustrate possible temporary practice pause then resumption study findings and inferences that may be made from them.
The pattern in Panel D during the pause period is roughly similar to that observed in the Vyvanse withdrawal study's placebo group, and the pattern in Panel A is similar to that observed in the Vyvanse continuation group. 15 In the Vyvanse study, subjects randomly assigned to placebo withdrawal had a substantially higher proportion with relapse or treatment failure than subjects who continued the drug. This contributed significantly to the FDA's approval of Vyvanse for maintenance therapy. Of note, the increase or decrease in a measured value of interest (relapse or treatment failure, in the Vyvanse example) might not be evident until a minimum amount of time elapses between the start of the pause and the observation of a change in the variable of interest. In the Vyvanse study, the drug main effect of interest was not apparent before day 5 of withdrawal, then began to be seen at about 1 week, and the effect was clear and pronounced after about 1 month of withdrawal.
The Vyvanse example is given to demonstrate general patterns, and its duration of withdrawal should not be automatically extrapolated to CAM-MABI studies. The duration of the pause (the “washout period”) is a key decision in study design. Factors to consider in deciding on pause duration include but are not limited to safety concerns and subjects' health status, the specific measurable attributes of interest, the CAM-MABI, the subjects' practice durations, and practical issues such as resource availability and subject recruitment feasibility. Study piloting should be helpful in determining duration of withdrawal, taking into account intersubject variability of practice pause–related changes in variables of interest. Some measurable attributes will be more plastic than others, and it is possible that some variables of interest may show significant changes with pauses as brief as 2 days. On the other hand, in the event of a failure to observe in a study group a change in a metric of interest after the entire withdrawal period, it would be prudent to qualify the lack of observed change with mention of the duration of the pause. Indeed, a pause of a few days might not be sufficient to change certain measurable attributes acquired through years or even decades of training and practice. In some instances, CAM-MABI practice could conceivably lead to permanent changes, with the likelihood of permanent changes correlated with practice duration.
Important Considerations of the Withdrawal Study Design
Ethical considerations are important with respect to discontinuing temporarily a practice that may be positively impacting a practitioner's life. Institutional Review Board approval of withdrawal studies, like all studies with human subjects, is essential. As noted above, the withdrawal study design has been employed to study treatments of multiple important diseases. Consideration of enrolling a practitioner in a withdrawal study should be done with careful evaluation of the nature and duration of the study intervention and evaluation of the practitioner's potential for adverse effects of pausing, including but not limited to the practitioner's current health status, medical history, and the reason(s) the practitioner initiated and maintains his or her practice. Close monitoring of practitioners during their pausing of CAM-MABI can facilitate “early escape” from the pausing, return to their usual practice and other intervention if indicated. 3,4 In addition, although it might be postulated that requesting a practitioner to pause practice may increase the likelihood for that person's practice to weaken or end, it is also possible that the pause may create a strengthened desire, link, and appreciation relative to the practice. Moreover, there is at least the possibility that some desirable effects may accrue as a result of pausing even though these are not expected to predominate and are not the intent of pausing; thus, the occurrence of both adverse and desirable events should be captured.
When a study design that requests that practitioners pause their practices is not acceptable, variants of the withdrawal study design may be considered. One variant study design would be to study practitioners who decide independently and of their own volition to stop practice. Another variant would be to study practitioners whose practices usually vary substantially in intensity over time (for example, a week or month of daily practice alternating with a week or month of not practicing), comparing within subjects periods of more intense to periods of less intense practice; comparison could also be made to subjects whose practices' temporal variation is substantially less. From a methodological perspective, both of these variant approaches have a major hurdle to overcome in that the reasons for the practitioner's changes in practice may confound any study measure's association with practice. For example, a rise in plasma levels of an immunomodulatory cytokine observed with pausing of practice might be due to a correlate of, or the precipitant of, the pausing of practice rather than the pausing of practice itself. Analytic attention to such potential confounding would be necessary and could potentially obviate the confounding, depending on the specific study design, research question of interest, and analytic solution.
Limitations
The FDA and the International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use have included in their guidance for the setting of drug withdrawal studies: “In using randomized withdrawal designs, it is important to appreciate the possibility of withdrawal phenomena, suggesting the wisdom of relatively slow tapering.” 3,4 For CAM-MABI studies, pilot evaluation of the speed of tapering and the duration of withdrawal could be indicated and be a function of the metric of interest and other factors noted above (see Important Considerations of the Withdrawal Study Design).
Another caveat of the FDA and International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use is: “A patient may develop tolerance to a drug such that no benefit is being accrued, but the drug's withdrawal may lead to disease exacerbation, resulting in an erroneous conclusion of persisting efficacy.” 3,4 Disentangling and distinguishing these two sharply contrasting possibilities could be aided by assessing the specific exacerbation and assessing whether its converse is observed in association with the onset or ramping up of a meditative practice. Fortunately, in this regard the desired measurable variables of interest for study of CAM-MABI pausing would not primarily involve pathology or disease but rather functional measures of mind and body, including neurologic function. Of interest, a PubMed literature search for meditation cessation or meditation withdrawal did not find any concerning reports, and a similar search could be done for any CAM-MABI of interest.
Expectancy and belief may be associated with measurable changes in new CAM-MABI practitioners. 16 Expectancy and belief may also be associated with measurable changes in CAM-MABI practitioners who pause their practices, and these changes may be in the opposite direction seen in new practitioners. Thus, expectancy- and belief-related characteristics relative to practice pausing should be assessed prior to randomization and in all study arms.
Assessing the adherence of practitioners to randomization to CAM-MABI pausing will likely rely to a large extent on self-report. However, depending on the practice involved and feasibility, independent assessment that a pause actually occurred should be useful for confirmation of self-report. For example, when the practice to be paused is usually performed in a group setting, assessment of the pause can be facilitated. In addition, adherence by advanced practitioners to pausing their practices could be enhanced by their appreciating that their participation may lead to clearer and deeper scientific understanding of their practice that may help not only themselves but also others.
Conclusions
This article is intended to stimulate methods development and exploration in a methodologically challenging domain of investigation. Experience from the drug evaluation field holds valuable methodological insights for CAM-MABI investigations. The TPPR approaches described above should be considered open to modification and adaptation to specific study questions, populations, and areas of interest. TPPR can be suitable to investigate many of the CAM-MABI modalities that are listed by National Institutes of Health/National Center for Complementary and Alternative Medicine. 17 The study findings most interesting to investigators will likely be key measurable data that change with temporary pausing of CAM-MABI practice, followed by return to pre-pause levels with resumption of practice; this would suggest a link of the practice to the measured changes. Such findings using the TPPR tool may enhance our insight into fundamental biologic processes, leading to beneficial practical applications.
Footnotes
Acknowledgment
The author gratefully acknowledges review of this article and suggestions by Peter Wayne, PhD, and Martin Kulldorff, PhD, and digitalization of the figures by Jon Fryzek, PhD, and Kui Xu, MD, PhD.
Disclosure Statement
No competing financial interests exist.