
Abstract
Background and Objective:
Bikram yoga is the most popular form of hot yoga, despite the limited information available on its cardiovascular benefits. This study sought to determine the effect of Bikram yoga on arterial stiffness and insulin resistance in young and older adults.
Methods:
Twenty-four young (mean age±standard deviation, 30±1 years) and 18 middle-aged and older (mean age, 53±2 years) adults completed an 8-week Bikram yoga intervention. Bikram yoga classes were performed for 90 minutes per session, three times per week, in a room heated to 40.5°C with 40%–-60% relative humidity.
Results:
Body mass, body fat percentage, blood pressure, and fasting blood glucose and triglyceride concentrations did not significantly change as a result of the intervention in either the young or the older group. Trunk flexibility, as measured by the sit-and-reach test, increased in both groups (p<0.01). Total (p<0.05) and low-density lipoprotein cholesterol (p<0.05) levels, plasma insulin concentrations (p<0.01), and scores on the homeostatic model of the assessment of insulin resistance (p<0.01) decreased in older adults, whereas total and high-density lipoprotein cholesterol concentrations were reduced in young adults (all p<0.05). Carotid artery compliance (p<0.05) was increased and β-stiffness index decreased in young (p<0.05) but not in older adults. Carotid pulse pressure did not significantly change in either group.
Conclusion:
A relatively short-term Bikram yoga intervention improved arterial stiffness in young but not older adults and significantly reduced insulin resistance index in older but not young adults.
Introduction
A
Bikram yoga is a form of hot yoga that has been widely practiced over the past few decades in the United States, with exponential growth worldwide. Although this widely practiced alternative medicine has gained popularity and acclaim, there is a paucity of scientific data supporting its associated health benefits. No published studies have assessed the effects of Bikram yoga on arterial stiffness or insulin resistance. However, some indirect observations have suggested that Bikram yoga might help improve vascular function. For instance, stretching and relaxation exercises reduce arterial stiffness, 6 and inverse associations between trunk flexibility and arterial stiffness have been demonstrated in middle-aged and older adults. 7 Practiced at a temperature of 40.5°C with 40%–60% relative humidity, Bikram yoga can also be considered a form of thermal therapy. An animal study observed an increase in expression of endothelial nitric oxide synthase 3 messenger RNA with thermal therapy, 8 which could account for a reduction in arterial stiffness with Bikram yoga through endothelium-dependent vasodilation. Additionally, previous studies using an animal model have reported reductions in hyperinsulinemia and attenuations in high-fat diet– induced glucose intolerance with hot tub therapy. 9 These improvements were attributed to increases in heat shock protein levels. 9
Accordingly, the primary aims of the present investigation were to determine the effects of Bikram yoga, the most popular form of hot yoga, on arterial stiffness in young and older adults and to determine whether the presumed enhancements in arterial stiffness would be accompanied by reductions in insulin resistance. The hypothesis was that the magnitude of change in arterial stiffness would be greater in older than in young adults on the basis of two previous observations. First, arterial stiffness is elevated in middle-aged and older adults and is more likely to be reduced in this population due to the law of initial baseline. 1,10 Second, regular aerobic exercise produces favorable adaptations in the vasculature, which is more likely in older than in young adults. 11
Materials and Methods
Ethical approval
The Institutional Review Board at the University of Texas at Austin reviewed and approved the experimental procedures, and participants provided written informed consent in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki.
Participants
Twenty-four apparently healthy young adults (13% male) aged 18–39 years and 18 middle-aged and older adults (28% male) aged 40–70 years completed an 8-week Bikram yoga intervention.
All participants were free of overt cardiovascular disease as assessed by a comprehensive health history questionnaire and were nonsmokers at the time of the study. Exclusion criteria included habitual physical activity during the last 6 months, pregnancy, uncontrolled hypertension, infection within the previous 4 weeks, renal disease, adrenal or endocrine tumors, prior myocardial infarction, known coronary artery disease, chronic heart failure, personal history of stroke or cardiac arrhythmias, diabetes, heat intolerance, and cardiovascular or hormone replacement therapy medications.
Procedures
All testing was performed after participants had fasted for 12 hours in the absence of caffeine. All vascular measurements were performed in the morning to avoid diurnal changes and after the participant had rested in the supine position for at least 15 minutes in a quiet, temperature-controlled room. Premenopausal female participants were tested during the early follicular phase of the menstrual cycle to avert the influence of estrogen and progesterone on outcome measures.
Body composition was determined via dual-energy x-ray absorptiometry (GE Medical Systems, Fairfield, CT). Trunk flexibility was determined by using a sit-and-reach box after the participants walked on a treadmill for 5 minutes as a warm-up. Fasting blood samples were obtained from the antecubital vein and were analyzed for lipid and lipoprotein concentrations with standard enzymatic methods. Hemoglobin A1c was analyzed by using the affinity chromatography technique (BioRad, Hercules, CA). Plasma insulin concentrations were determined via insulin antibody-coated tube 125I radioimmunoassays (MP Biomedicals, LLC, Solon, OH). The homeostatic model of the assessment of insulin resistance (HOMA-IR), an index of insulin resistance, was calculated by using the following equation: 12 (fasting plasma insulin×fasting blood glucose)/22.5.
Carotid artery compliance was measured noninvasively via simultaneous acquisition of tonometrically obtained pressure waveforms and ultrasonographically obtained images of the carotid artery. 1 Brachial systolic and diastolic blood pressures were measured in the supine position. Carotid artery compliance was calculated by using the following equation, where D1 and D0 are maximal and minimum arterial diameters and P1 and P0 are maximal and minimum blood pressures, respectively: [(D1−D0)/D0]/[2(P1−P0)]×π×D0 2 . In addition, β-stiffness index, an index of arterial stiffness that adjusts for the effect of alterations in distending pressure on arterial diameter, was calculated using the following equation: (lnP1/P0)/[(D 1−D 0)/D 0].
In our laboratory, the day-to-day coefficients of variation (mean±standard error) were 2%±1%, 7%±3%, and 5%±2% for carotid artery diameter, pulse pressure, and arterial compliance, respectively.
Bikram yoga intervention
Participants completed three Bikram yoga classes per week for 8 weeks. The intervention duration of 8 weeks was chosen according to previous exercise intervention findings that changes in arterial stiffness occur fairly rapidly in the first 4–8 weeks after the initiation of exercise programs. 1,6 They were instructed not to engage in any other forms of exercise or alter their normal dietary patterns. Classes were performed at local Bikram yoga studios, where rooms were heated to 40.5°C with 40%–-60% relative humidity. All classes lasted 90 minutes, began and ended with breathing exercises, and consisted of a standardized series of 26 different postures (several standing postures followed by floor postures) designed to improve balance, strength, and flexibility. All Bikram yoga instruction was scripted and standardized. Upon arrival at each session, participants signed in at the respective yoga studio and computer-generated attendance reports were obtained.
Statistical analyses
Data were analyzed using SPSS and are presented as means±standard error of the mean. Analysis of variance was used to compare young and older groups as baseline, and paired-sample t-tests were used to analyze changes in dependent variables with the Bikram yoga intervention. The significance was set a priori at p<0.05.
Results
At baseline, the young and older groups were not different in body mass, body fat percentage, blood cholesterol and triglyceride concentrations, hemoglobin A1c, or brachial blood pressure (Table 1). Older participants had higher (p<0.05) fasting blood glucose and HOMA-IR scores than young participants. Sit-and-reach scores were higher in young versus older participants (p<0.05).
Values are means±standard error of the mean.
p<0.05 versus young.
p<0.05 versus before.
p<0.01 versus before.
BP, blood pressure; HDL, high-density lipoprotein; HOMA-IR, homeostasis model of assessment of insulin resistance; LDL, low-density lipoprotein.
Body mass and composition did not significantly change as a result of the intervention in either group. After the Bikram yoga intervention, total and high-density lipoprotein cholesterol levels decreased (p<0.05) in young participants, whereas total and low-density lipoprotein cholesterol levels decreased (p<0.05) in older participants. Plasma insulin concentrations and HOMA-IR scores were reduced in older (p<0.01) but not in young participants, whereas fasting blood glucose and hemoglobin A1c did not change in either group. Blood pressures did not significantly change in young or older participants. Trunk flexibility increased in both groups (p<0.05) after the yoga intervention.
At baseline, carotid artery compliance and carotid pulse pressure were not different between the groups (Fig. 1). Carotid artery compliance increased significantly in young (p<0.05) but not in middle-aged and older participants. The trend was the same (although inverse in direction) when β-stiffness index was calculated.
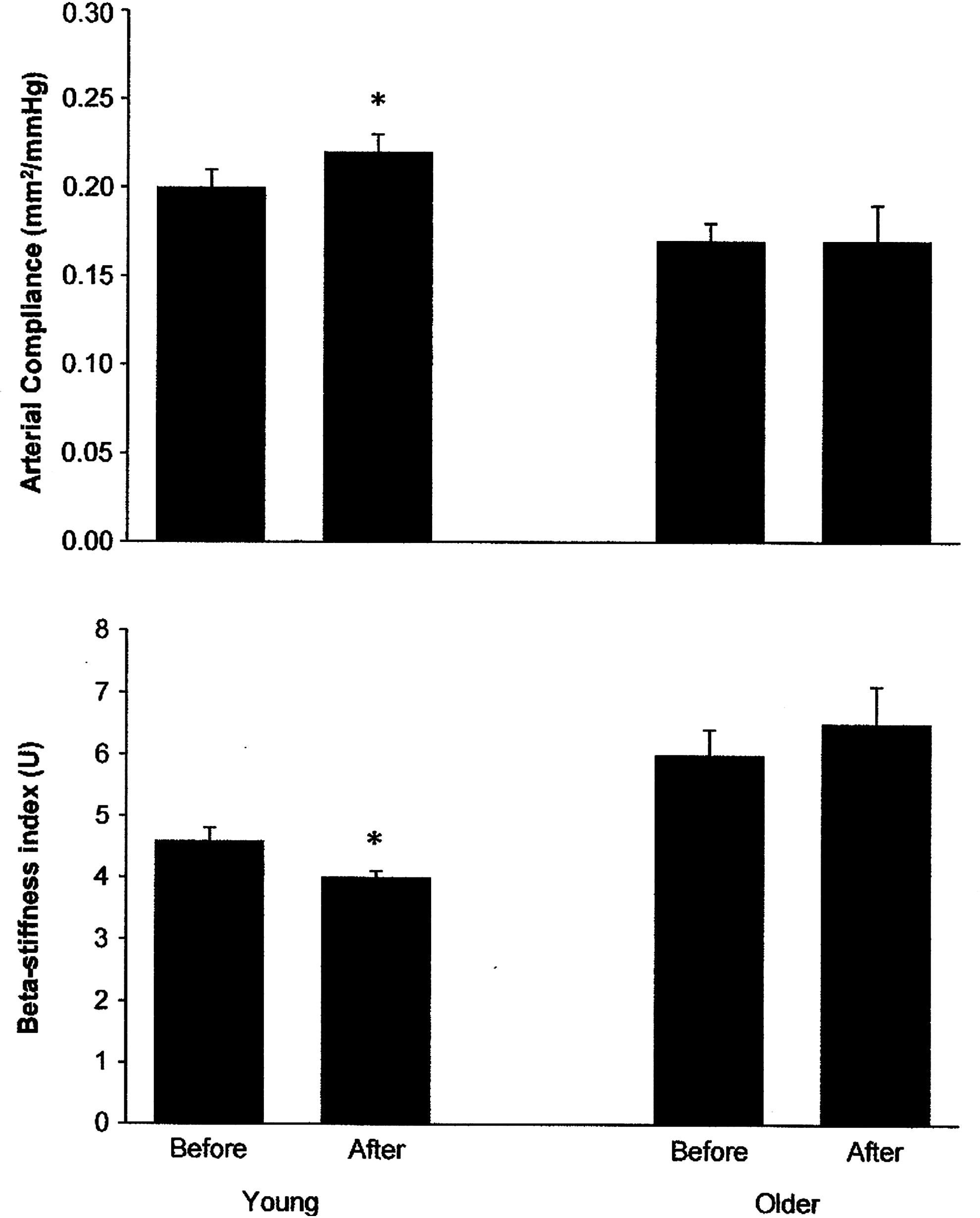
Changes in carotid artery compliance and β-stiffness index with the hot yoga intervention in young and older participants. Carotid artery compliance increased and β-stiffness index was reduced in young but not in older participants. *p<0.05 versus before.
Discussion
The results from the present study indicate that a relatively short-term Bikram yoga intervention reduced arterial stiffness in young but not in older adults and significantly reduced HOMA-IR index in older but not young adults. This appears to be the first study to investigate the effect of hot yoga on arterial stiffness and metabolic risk factors.
The most salient finding of the present study is that regular Bikram yoga practice demonstrated an arterial destiffening effect in young participants. At least three elements in Bikram yoga could act to reduce arterial stiffness. First, stretching is a large component of Bikram yoga postures. The authors' laboratory has previously reported an increase in carotid artery compliance with regular stretching exercises, 6 and negative correlations between trunk flexibility and arterial stiffening have been reported by others. 7 The aforementioned study 6 suggested that the increase in carotid artery compliance with stretching was due to a significant reduction in pulse pressure. In the current study, however, pulse pressure was unaltered by the hot yoga intervention. It is plausible that the stretching exercises could have imposed a traction stimulus to the arteries, resulting in matrix and smooth muscle cell adaptations that favorably affected cross-sectional arterial compliance. Sustained axial stretching of the cardiothoracic artery has been shown to modify arterial wall content and induce matrix reorganization, 13 which could act to reduce arterial stiffness.
Second, relaxation and meditation are important and essential constituents in Hatha yoga practices. Indeed, regular yoga practice is known to reduce stress and anxiety, 14,15 both of which could reduce sympathetic vasoconstrictor tone and chronic restraint placed on the arterial wall.
Third, the thermal therapeutic component of Bikram yoga could have elicited reductions in arterial stiffness, as studies have shown transient reductions in an index of central arterial stiffness with thermal therapy. 16 The mechanism by which thermal therapy affects arterial stiffness is not known. However, increases in expression of endothelial nitric oxide synthase-3 messenger RNA have been reported with thermal therapy in animal models. 8
In addition to reductions in interleukin-6 and C-reactive protein levels that have been reported with yoga practice, 17,18 other physiologic factors, including increases in nitric oxide availability and reductions in endothelin-1, 19 –22 that have been observed after regular exercise training could contribute to reductions in arterial stiffness. It is more than likely that the physiologic mechanisms underlying reductions in arterial stiffness with Bikram yoga in young adults are multifactorial in nature.
The present finding that the reduction in arterial stiffness was limited to young adults participants was rather perplexing and is contrary to the original hypothesis. Given that arterial stiffness increases with age and that a reduction is more consistently shown in older than in young adults with exercise training interventions, 1,11 the study hypothesis was that the older adults would demonstrate a larger reduction in this variable. Perhaps because of the potential loss of plasticity with aging, 23 the intervention duration and/or frequency might have been insufficient to significantly alter this variable in older participants. However, longer yoga interventions of 3 and 8 months also failed to decrease arterial stiffness in middle-aged adults. 24,25 Taken together, the available evidence indicates that yoga (either regular Hatha or Bikram) does not significantly affect arterial stiffness in middle-aged and older adults.
Unlike the older adults, younger participants were able to reduce arterial stiffness with the Bikram yoga intervention. These results are consistent with the previous cross-sectional data, which demonstrated lower levels of arterial stiffness in Hatha yoga practitioners versus sedentary adults 26 and also agree with a recent intervention study that demonstrated significant increases in arterial compliance in young adults with 6 weeks of Dhyana yoga practice. 27
Insulin resistance improved significantly in older participants as a result of the hot yoga intervention, as indicated by the reduction in HOMA-IR scores, whereas no changes were observed in young participants. The improvement in insulin resistance in older participants may be attributed to the effects of the yoga postures and/or heat in which the exercise was performed. The present finding agrees with a previous study showing reductions in HOMA-IR with 16 weeks of Hatha yoga in postmenopausal women with elevated metabolic risk. 28 It is also consistent with a previous study demonstrating attenuations in high-fat diet–induced glucose intolerance and hyperinsulinemia with thermal therapy in an animal model. 9 In addition to insulin resistance, both total and low-density lipoprotein cholesterol were significantly reduced in the older participants, whereas total and high-density lipoprotein cholesterol were reduced in young participants. Previous studies have shown reductions in total and low-density lipoprotein cholesterol with Hatha yoga 28,29 and thermal therapy. 30
Several limitations should be noted. First, the number of participants studied was relatively small. Second, a nonyoga sedentary control group was not included. Third, Bikram yoga is a hybrid form of lifestyle modification that includes a variety of elements, such as relaxation, meditation, stretching, isometric exercises, and thermal therapy, and this study could not tease out the effect of each component of Bikram yoga on arterial stiffness and metabolic risk. The primary intention was to produce more generalizable findings that directly assessed the effects of popular Bikram yoga practices. In this context, it should be emphasized that Bikram yoga classes are tightly standardized and are composed of performing a set series of 26 postures in exactly 90 minutes.
In conclusion, a relatively short-term Bikram yoga intervention reduced arterial stiffness in young but not in older adults. Bikram yoga also reduced lipoprotein levels and improved trunk flexibility in young and older adults. Clearly, additional studies are needed to better understand the effects of Bikram yoga on overall health and vascular function in particular. Although no incidents occurred during this study, the occurrence of heat injury and/or illness has been suspected during Bikram yoga, especially in older adult populations. As such, it may be necessary to advise older adults to use caution when practicing Bikram yoga.
Footnotes
Acknowledgments
We would like to extend our gratitude to Pure Bikram Yoga and Yogagroove yoga studios for their support of this project through participant recruitment and class rate concessions.
Disclosure Statement
No competing financial interests exist.