
Abstract
Objective:
Pregnancy-related lumbopelvic pain is a major problem for the majority of pregnant women. Complementary medicine has been used to alleviate pain, and yoga is one of the most commonly chosen alternative methods. The objective of this study was to assess the effectiveness of Hatha yoga in the reduction of lumbopelvic pain in pregnancy.
Methods:
A randomized controlled trial with 60 pregnant women (age range, 14–40 years) who reported lumbopelvic pain at 12 to 32 weeks of gestation was conducted from June 2009 to June 2011. Pregnant women who had twin pregnancies, had medical restrictions for exercise, used analgesics, and participated in physical therapy were excluded from the study. Pregnant women were divided into two groups: the yoga group, practicing exercises guided by this method, and the postural orientation group, performing standardized posture orientation according to instructions provided in a pamphlet. Treatment in each group lasted 10 weeks. A visual analog scale (VAS) was used to measure pain intensity. Lumbar pain and posterior pelvic pain provocation tests were used to confirm the presence of pain. Statistical analysis included the Mann–Whitney test, the McNemar test, a paired Wilcoxon test, and analysis of covariance.
Results:
The median pain score was lower in the yoga group (p<.0058) than the postural orientation group. Lumbar pain provocation tests showed a decreased response in relation to posterior pelvic pain provocation tests and a gradual reduction in pain intensity during 10 yoga sessions (p<.024).
Conclusions:
The yoga method was more effective at reducing lumbopelvic pain intensity compared with postural orientation.
Introduction
T
Complementary and alternative medicine (CAM) has received increasing attention in scientific communities around the world. Many ongoing studies are assessing the usefulness and safety of CAM, particularly for the relief of low-back pain. 9,10 In Brazil, one of the main reasons for use of alternative medicine is to relieve physical pain. 11 Yoga, accessible and well known in various countries worldwide, is one of the most widely used methods of CAM. In the 1990s, around 15 million women in the United States had practiced Yoga at some time in their lives. 12 Among other forms of therapy, professional healthcare workers from CAM organizations in the United Kingdom have indicated yoga as a treatment method for several disorders. 10
To the best of our knowledge, no published study has examined the use of yoga for treatment of pregnancy-related low-back pain (PLBP) and pregnancy-related pelvic girdle pain (PGP) during the gestational period. Therefore, the study design was based on the hypothesis that pregnant women reporting this type of pain could benefit from properly applied yoga and monitoring by physical therapists. The aim of this study was to evaluate the effectiveness of Hatha yoga exercises in alleviating PLBP and PGP.
Methods
A randomized controlled trial (RCT) was conducted to assess the efficacy of Hatha yoga exercises in pregnant women with lumbopelvic pain (PLBP and PGP).
The sample size was calculated by the evolution of mean pain intensity scores reported for a Global Active Stretching group at the end of the first and eighth weeks of treatment. The mean and standard deviation of pain intensity at the end of the first week was 4.9±3.1. At the end of the eighth week, pain intensity was 0.85±1.9. It was assumed that the effect of yoga treatment would be similar to that found with Global Active Stretching in the study by Martins and Pinto e Silva 13 in a population with the same characteristics. Significance level was set at 5%, considering a power test of 80%, based on the difference in the means reported. A paired t-test was adopted for comparison. The smallest sample size needed for each group was seven. Nevertheless, the current study included 30 women per group because eventual losses after randomization were predicted.
The study was conducted from June 2009 to June 2011 in Basic Healthcare Units, Paulínia, São Paulo, Brazil. Paulínia is an industrial center with approximately 80,000 inhabitants. Postural pain during pregnancy was prevalent in 79.8% of women living in the city. 8
Pregnant women receiving prenatal follow-up were included between the 12th and 32nd weeks of pregnancy. During consultation, these women were interviewed and met eligibility criteria if they reported and confirmed PLBP or PGP by marking pain sites on a drawing of a human figure. Exclusion criteria were twin pregnancies, medical restriction for exercise, use of analgesics, and participation in physical therapy for these symptoms.
For patient allocation, a list of random numbers was generated by computer for 60 participants using SAS software (SAS Institute, Inc., Cary, North Carolina). The researcher was blinded to allocation sequence by use of sealed, sequentially numerated, opaque envelopes. The envelopes were opened after the initial interview had ended, the informed consent term had been signed, and pain provocation tests had been applied.
Patient identification data were recorded in a notebook containing name and number of patient chart. To differentiate pain location, lumbar pain provocation tests for PLBP 14 and posterior pelvic pain provocation tests for PGP 15 were used.
For the lumbar pain provocation test, the physical therapist asked the pregnant woman to stand with her knees joined together and perform flexion of the trunk, bending forward until the lower limbs went into flexion. The test result was considered positive if the patient reported pain in the lumbar region, on trunk circumduction, and on palpation of the paraspinal lumbar musculature and upon confirmation of the pain site marked on a drawing of a human figure. 14
For the posterior pelvic pain provocation test, the pregnant woman was instructed to lie in a supine position with one leg flexed and the other extended. The knee of the flexed leg that was in the vertical position was pressed in the direction of the homolateral sacroiliac joint, stabilizing the other side simultaneously. The test result was considered positive when the pregnant woman reported pain in the sacroiliac region in the compressed leg or when turning in bed at night, when she felt weight in the deep gluteus muscle region, and when she indicated the pain location on a drawing of the human figure. 15
A visual analog scale (VAS) 16 was used to estimate pain intensity according to each pregnant woman, investigated by initial and final interview and at the beginning and end of yoga sessions. The scale was presented to the pregnant woman in a graphic form. Pain was ranked in an increasing order from 0 to 10. At the beginning, middle, and end of the scale three facial expressions represented pain, classified as weak, median, and severe.
After testing, the women were randomly allocated to participate in weekly yoga sessions or receive a pamphlet that described postural orientation for daily activities.
Pregnant women from the yoga group (a maximum of 10 per group) participated in 10 Yoga sessions once a week for 1 hour each. Sessions were administered by one researcher, who is a physical therapist and licensed Hatha yoga instructor. For treatment, 34 poses (asanas) were chosen to stimulate the psychophysical effects, such as joint range of motion, flexibility, strengthening, muscular resistance, balance, stimulation of introspection, self-confidence, self-control, concentration, and mental relaxation (Fig. 1). The breathing exercises performed were complete breathing, square breathing, and polarized breathing. 17
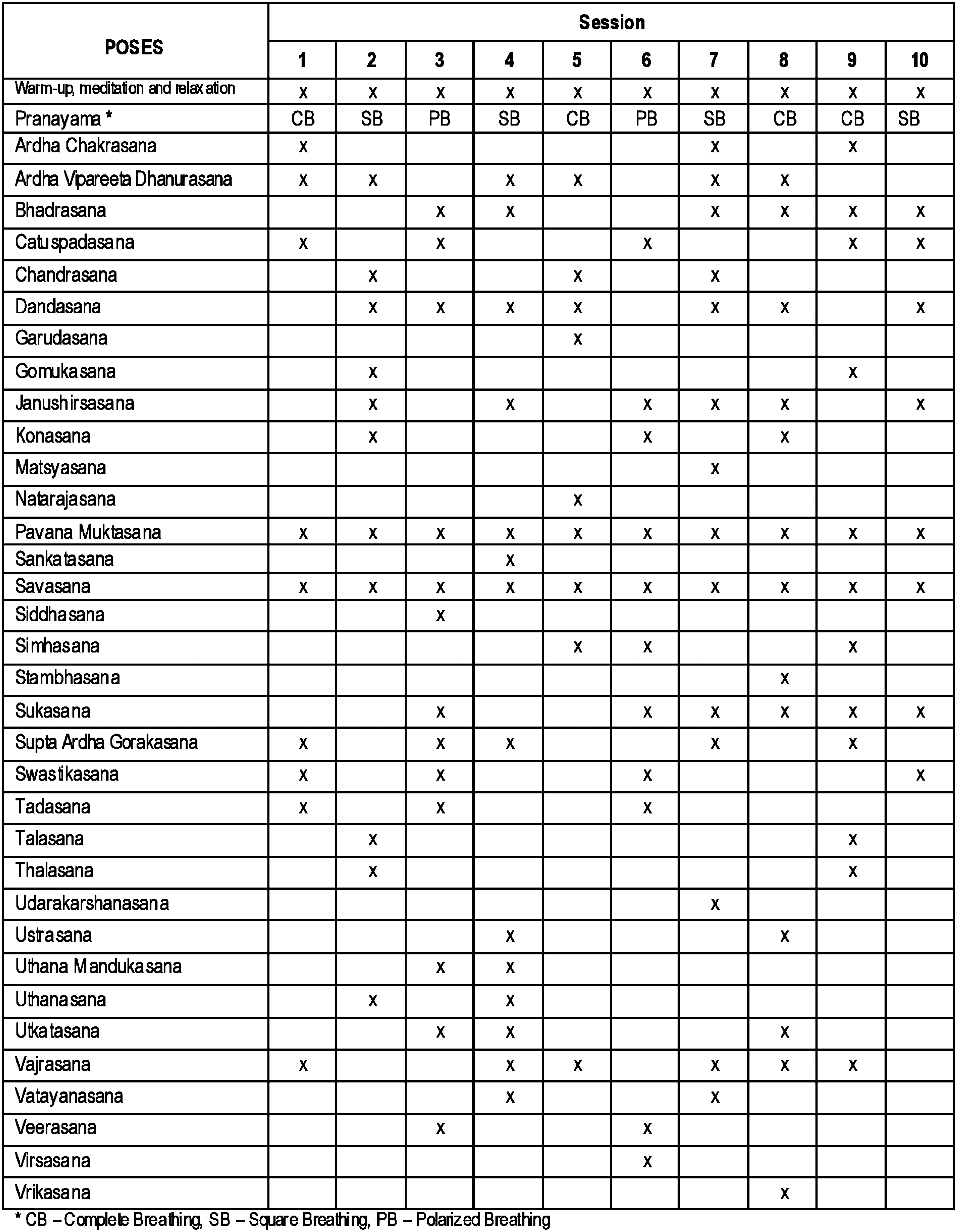
Poses used in Yoga sessions.
Sessions were divided into three time points: Initially, attention was focused on the breathing rhythm and warm-up of the major joints (10 minutes) in a moment of introspection, followed by poses and breathing exercises (40 minutes). In the end, women listened to messages of meditation and relaxation (10 minutes). At the beginning and end of each session, pain intensity was assessed.
Pregnant women in the control postural orientation group received a pamphlet on postural orientation that contained figures and text explaining some possible changes in the curvature of the vertebral spine during pregnancy (hyperlordosis and hyperkyphosis). Suggestions concerning spinal positioning were made for daily activities, while lying down (to lie on one's side with a proper support for the head and abdomen and between the knees), while sitting (to have adequate lumbar and foot support), and while standing (to have feet supported and to lengthen the handle of the broomstick).
After 10 weeks, both groups were scheduled for final data collection, including information on weight, height, location and intensity of pain, and the results of lumbar pain and posterior pelvic pain provocation tests.
Homogeneity between groups was tested using the Mann–Whitney test. A McNemar test was applied to compare the presence of lumbar pain and posterior pelvic pain in each group at the beginning and end of follow-up. To compare group behavior regarding pain (VAS), rank analysis of covariance was performed. Pain intensity distribution measured by VAS was compared between time periods before and after intervention by using the Wilcoxon nonparametric test for paired samples. The analyses were performed by using SAS software, version 9.1. A statistical significance level of 5% was adopted.
The study protocol was approved by the Municipal Health Office of Paulínia, by the Research Ethics Committee of the Department of Obstetrics and Gynecology–Women's Integrated Healthcare Center, and by the Research Ethics Committee of the Universidade Estadual de Campinas–UNICAMP School of Medicine. All participants signed a free informed consent term before the initial interview and randomization.
Until November 2012, no RCTs were identified in the following electronic databases: MEDLINE, Popline, the Scientific Electronic Library On-line (SciELO), Latin American and Caribbean Health Science Information (LILACS), Science Direct, and Cochrane Library. The databases were searched by using the following keywords: (“pregnancy”) AND (“yoga” OR “back pain” OR “low back pain” OR “lumbar back pain” OR “pelvic pain” OR “lumbopelvic pain”).
Results
Of the 245 pregnant women interviewed, 185 were excluded before intervention. Of those excluded, 181 (73.7 %) did not meet the inclusion criteria and four (1.63%) declined to participate. Sixty (24.48%) satisfied the inclusion criteria and were allocated to follow-up groups. Of the 60 women enrolled, 45 (75%) completed the study. Nine pregnant women from the yoga group were lost to follow-up: Two declined to participate, six withdrew from treatment, and one had an obstetric complication (cerclage). Six pregnant women discontinued intervention with the postural orientation group: two because of treatment withdrawal and four because of obstetric complications (two premature deliveries and two placental abruptions) (Fig. 2).

Procedures for selection and follow-up of pregnant women (per Consolidated Standards of Reporting Trials, 2008). 48
Both groups were similar in age, gestational age, and body mass index (Table 1). Concerning pain location before treatment in both groups, 10 (17%) pregnant women had PLBP, 12 (20%) had PGP, and 38 (63.3%) had PLBP associated with PGP or lumbopelvic pain. Regarding pain intensity at the beginning and end of the intervention, a final VAS score of 0 (no pain) was reported by 71.4% (p<.0211) in the yoga group and 20.8% (p<.4702) in the postural orientation group. Pain intensity decreased in the yoga group (Table 2).
Units of measure for variables are as follows: age (years), gestational age (weeks), weight (kg), height (m), body mass index (kg/m2).
Mann-Whitney test.
Comparison was done by using the McNemar test.
p<.05.
p<.01.
p<.001.
Not significant.
After the intervention, results on lumbar pain provocations tests were negative and significant in both groups. In the yoga group, trunk flexion test results were 52.4% in the beginning and 9.5% at the end (p<.01), palpation of the spinal musculature was 52.4% in the beginning and 4.8% at the end (p<.01), pain on circular motion of the trunk was 60% in the beginning and 5% at the end (p<.001), and confirmation of pain location was 76.2% in the beginning and 9.5% at the end (p<.001). In the postural orientation group, flexion test results for the trunk were 69.6% in the beginning and 8.7% after the intervention (p<.001), palpation of the spinal musculature was 60.9% in the beginning and 17.4% at the end (p<.01), pain on circular motion of the trunk was 72.7% in the beginning and 36.4% at the end (p<.05), and confirmation of pain location was 77.3% in the beginning and 45.5% at the end (p<.05). The trunk range of motion continued to decrease in both groups, and there was no significant difference between the initial and final intervention. On posterior pelvic pain provocation tests, results after the intervention were not significantly different (Table 2).
After adjustment for the initial VAS scores, median pain intensity scores in the yoga group were 6 in the beginning and 0 at the end. In the postural orientation group, the scores were 7 and 4.5, respectively. Pain decreased in the yoga group (p<.0058) (Table 3).
Rank analysis of covariance.
During the yoga intervention, the VAS score was recorded in the beginning and at the end of each session. Mean pain intensity scores progressively decreased during the 10 sessions (p<.024) (Fig. 3).

Evolution of mean pain intensity scores in 10 Yoga sessions. VAS, visual analog scale.
Using open-ended questions and colloquial speech at the end of the yoga sessions, all pregnant women in that group described the method as excellent. Ninety percent of the pregnant women thought of recommending the method, and 100% reported a decrease or cessation of pain after exercise. Exercises were considered relaxing and favorable for decreasing physical discomfort, alleviating tiredness, improving body posture, and helping perform daily routine activities with safety. Women learned to control pain without the use of analgesics. The emotional effects reported were tranquility, decreased stress, an easy mind, mental balance, and feeling closer to the baby.
In the control group (the postural orientation group), half of the pregnant women found that orientation was good and 11 (45.8 %) would recommend the method, believing it was useful for partial pain relief. However, they emphasized that pain diminished partially, and some women thought postures were difficult to perform because of pain intensity. The most frequently modified posture was the lying position (with placement of head support and support below the abdomen and between the knees), followed by standing (with foot support and broomstick stretching) and sitting (with lumbar and foot support, as well as adjustment of chair height).
Discussion
To the best of our knowledge, this is the first RCT to show the effectiveness of the Hatha yoga method in relieving PLBP and PGP. Comparison with a control group was possible because all pregnant women in the study were randomly selected, permitting the formation of two groups that proved to be homogeneous.
This study found that the Hatha yoga method effectively decreased PLBP and PGP intensity after 10 weeks of intervention. A similar result was observed by Sherman et al.; 18,19 they found yoga to be more effective than the orientation manual at reducing these types of pain, with benefits lasting for some months. In a meta-analysis, Büssing et al. 20 suggested that yoga is an efficient complementary approach for pain and incapacity. Posadzki and Ernst 21 performed a systematic review to analyze interventions performed in RCTs among the general population for treatment of lumbar pain using the yoga method. 18,22 –26 They found that most studies observed a significant reduction in pain intensity, 18,23,25 –27 improvement in functional abilities, 18,23,25,28 and reduction in the use of analgesics. 23,25,27
The fundamental principle of the yoga method is that disorders have a psychosomatic origin. In the physical aspect, these disorders are triggered by an imbalance of the autonomic nervous system. Yoga intervention is aimed at regulating the psycho-neural-endocrine structures through the hypothalamus-pituitary-adrenal axis to rebalance the autonomic nervous system. 29,30 One biochemical effect is a decrease in plasma concentration of stressor hormones in particular: cortisol and catecholamine (epinephrine and norepinephrine). 30
Many positive results of yoga practice are described in the literature. Some of the benefits of yoga related to the skeletal muscle system can be cited as increases in respiratory function, 31 flexibility of the body 32,33 and vertebral spine, 24,34,35 strength, 35,36 muscular resistance, 35 balance, 36 joint range of motion, 37 and muscle relaxation. 38
The practice of Hatha yoga is based on breathing exercises (pranayamas) and poses (asanas), in addition to meditation. Both favor mental concentration and body relaxation. The poses act on all biomechanical axes and are actively performed by the patient, favoring the rebalance of muscles, joints, and ligaments.
Clinical pain provocation tests were used as tools to aid in the differential diagnosis of pain and to check whether postures and positions of daily living activities caused pain in pregnant women. Pregnant women in the yoga group with lumbar pain had a significantly negative response on provocation tests and had decreased pain as assessed by the VAS.
A controversial result occurred in the postural orientation group; no effective reduction in pain was seen in these women. However, the lumbar pain provocation test showed a decreased response. One reason for this result could be the reliability of the low-back pain provocation test; its sensitivity and specificity have still not been fully investigated, despite its wide use for diagnostic purposes in different circumstances. 14,39 Another reason could be that pain decreased in the postural orientation group, albeit insignificantly, which could alter provocation test results for this type of pain.
Response to the PGP provocation test did not decrease in either group, although pain intensity decreased in the yoga group. Nevertheless, when pain was provoked in the yoga group, it reappeared momentarily. This finding could be related to the pathophysiology of PGP, which involves many factors. A review by Vermani et al. 40 highlighted that trauma and mechanical, hormonal, metabolic, and degenerative factors are related to this type of pain. Those authors suggested that there may be a mechanical imbalance between pelvic structures (muscles, ligaments, fascia, and bones), especially the sacroiliac joint, which could be produced by high plasma concentrations of the hormone relaxin, causing gradual laxity of regional structures and resulting in increased pelvic mobility. Damen et al. 41 also observed a significant relationship between asymmetric laxity of the sacroiliac joint and the presence or appearance of PGP.
After treatment, almost all pregnant women approved of the Hatha yoga method and would recommend it to other pregnant women. In the literature, it is considered a very acceptable and safe practice during pregnancy. Furthermore, it is one of the first options chosen by women and suggested by obstetricians. 42,43 A qualitative study on patient perception of the Hatha yoga practice suggests that participants benefit from this method because it allows changes in cognitive and sensorial behavior in the face of pain. 44
The therapeutic use of yoga is still controversial. Vleeming et al. 45 and van Tulder et al. 46 state that no evidence is available to recommend this method of PLBP and PGP treatment. However, Dupeyron et al. 47 recommend the method for coadjuvant therapy because it might reduce the use of inadequate postural behavior and improve patient adherence to treatment.
This study had some limitations. In the literature, several RCTs confirm the effectiveness of yoga intervention in alleviating spinal pain in the general population. However, as of November 2012 no study had shown results on the efficacy of the Hatha yoga method in pregnancy-related lumbar and posterior pelvic pain.
During the intervention, some pregnant women in the yoga group abandoned the treatment because their pain had been relieved; this was inferred through the intensity of pain recorded at the last meeting attended.
Conclusions
Exercises based on the yoga method contribute to a decrease in pain intensity in the lumbar and posterior pelvic regions compared with a control intervention of postural orientation. Lumbar and posterior pelvic pain intensity decreased gradually during 10 weekly sessions of yoga. Clinical lumbar pain provocation tests showed decreased response at the end of the intervention in both groups. Clinical posterior pelvic pain provocation tests did not show any significant modification in either group at the end of the intervention.
We hope that this study may stimulate and encourage researchers to investigate methods for reducing the postural pain that affects many pregnant women and impairs their quality of life.
Footnotes
Acknowledgments
We thank the entire team of the Health Units and pregnant women who participated in and supported this study. We also thank all the professional healthcare workers involved in this study at the Department of Obstetrics and Gynecology. We especially thank to the team in the Department of Rehabilitation–Rehabilitation Sector of the Community at the Municipality of Paulínia.
This article is part of a doctoral dissertation, “Back Pain in Pregnancy: Prevalence, Risk Factors and Treatment of Lumbar and Pelvic Pain by the Hatha Yoga Method,” to be presented by Roseny Flávia Martins in the Department of Obstetrics and Gynecology of the Universidade Estadual de Campinas–UNICAMP School of Medicine. This trial is registered in the International Standard Controlled Trial Register (number NCT01576978).
Disclosure Statement
No competing financial interests exist.