
Abstract
Background:
Antidepressants including selective serotonin reuptake inhibitors (SSRIs) and serotonin noradrenaline reuptake inhibitors (SNRIs) are known to cause secondary sexual dysfunction with prevalence rates as high as 50%–90%. Emerging research is establishing that acupuncture may be an effective treatment modality for sexual dysfunction including impotence, loss of libido, and an inability to orgasm.
Objectives:
The purpose of this study was to examine the potential benefits of acupuncture in the management of sexual dysfunction secondary to SSRIs and SNRIs.
Subjects:
Practitioners at the START Clinic referred participants experiencing adverse sexual events from their antidepressant medication for acupuncture treatment at the Mood and Anxiety Disorders, a tertiary care mood and anxiety disorder clinic in Toronto.
Design:
Participants received a Traditional Chinese Medicine assessment and followed an acupuncture protocol for 12 consecutive weeks. The acupuncture points used were Kidney 3, Governing Vessel 4, Urinary Bladder 23, with Heart 7 and Pericardium 6. Participants also completed a questionnaire package on a weekly basis.
Outcomes measured:
The questionnaire package consisted of self-report measures assessing symptoms of depression, anxiety, and various aspects of sexual function.
Results:
Significant improvement among male participants was noted in all areas of sexual functioning, as well as in both anxiety and depressive symptoms. Female participants reported a significant improvement in libido and lubrication and a nonsignificant trend toward improvement in several other areas of function.
Conclusions:
This study suggests a potential role for acupuncture in the treatment of the sexual side-effects of SSRIs and SNRIs as well for a potential benefit of integrating medical and complementary and alternative practitioners.
Introduction
Studies have shown the most common cause of discontinuation of medication is related to intolerability or adverse events including nausea, somnolence, sweating, tremor, asthenia, dizziness, dry mouth, insomnia, constipation, diarrhea, decreased appetite, and sexual dysfunction. 6,7
Sexual Dysfunction
SSRIs and SNRIs have been reported to cause sexual dysfunction, with prevalence rates as high as 50%–90%. 8,9,10,11 Specific symptoms reported by patients include delayed orgasm, decrease sex drive, erectile dysfunction, and pain on intercourse, with the first three being the most commonly associated. 7 Consequently, sexual dysfunction secondary to the SSRIs and SNRIs remains a significant challenge to treatment adherence and to outcomes for patients suffering with anxiety disorders and depression. Some strategies used to manage antidepressant-induced sexual dysfunction include waiting for a certain period of time to confirm that the dysfunction is due to antidepressants, as up to 42% of patients report spontaneous remission, as well as employing short drug holidays (drug is withdrawn for a period of time) or altering antidepressants from one that is more prone to causing sexual dysfunction to one that is hypothesized to be less likely to cause symptoms. 10 Although these strategies aim to temporarily relieve the dysfunction, they are not a long-term response for best treatment outcomes.
An alternative option to the strategies mentioned above is to provide separate pharmaceutical treatment for the sexual adverse events themselves. However, there is concern with adding additional medication to treatment regimens, as secondary effects may result in patients already burdened by sexual dysfunction. To date, several drugs have been investigated as potential adjunctive treatments for antidepressant-induced sexual dysfunction. Bupropion, sildenafil, tadalafil, mirtazapine, phentolamine, mianserin, yohimbine, and bremelanotide have demonstrated some benefit; however, all carry a risk of adverse effects ranging from those typically associated with antidepressant medication to dangerous increases in blood pressure. 12 –19
Sexual dysfunction itself is not clearly understood. Sexual function is a complex biopsychosocial behavior dependent on the adequate functioning of psychologic, endocrine, vascular, and neurological processes. Sexual dysfunction is commonly associated with depression and anxiety disorders, even when medication is not utilized as a treatment modality. 20 Current treatments for primary sexual dysfunction include phosphodiesterase-5 inhibitors (e.g., sildenafil citrate), vacuum devices, and injectable dilating drugs. 20
Acupuncture
Acupuncture is one of the treatment modalities used in Traditional Chinese Medicine (TCM). TCM is a comprehensive therapeutic system that manages disease by assessing and correcting imbalances of Yin and Yang and energy movement within different organ systems in the body. Acupuncture is the practice of gentle insertion of needles at specific points throughout the body that correspond to different organs. The needles are thought to correct the energy imbalance or obstruction and restore normal function to the body. 21 The current literature supports a role for acupuncture in the treatment of a number of conditions including back pain, chemotherapy-induced nausea and vomiting, osteoarthritis, insomnia, dysmenorrhea, chronic fatigue syndrome and menopausal symptoms. 22 –28 Recently, Aung et al. reported findings suggestive of a role for acupuncture in the treatment of sexual dysfunction. 29
Although acupuncture is a novel approach for secondary treatment in a psychiatric clinical setting, the purpose of this study is to assess the efficacy of acupuncture as a treatment for sexual dysfunction secondary to antidepressant treatment in previously unaffected, sexually active men and women.
Methods
Study procedure
This study was an investigational, open-label case study. Patients were recruited by their psychiatric clinicians (MK and CC) at The START Clinic for the Mood and Anxiety Disorders, a tertiary care clinic in downtown Toronto. Referral to the study was based on adverse sexual effects as a result of SSRI or SNRI antidepressant treatment in the absence of a history of sexual difficulties. Prior to commencement of the study, all potential participants were given an evaluation visit to determine eligibility for enrollment. Potential participants were assessed using a standard psychologic evaluation, the MINI Neuropsychiatric Interview (M.I.N.I) (by MV), a TCM assessment involving pulse and tongue diagnosis, and a package of self-report questionnaires measuring anxiety, depression, and various aspects of sexual function. Individuals eligible for the study were those with current sexual dysfunction of any subtype that began after the initiation of antidepressant treatment, without a prior history of sexual dysfunction otherwise. Patients who met eligibility criteria, but were unable to make weekly appointments were excluded from the study. All other eligible individuals were offered enrollment in the study, and those interested in participating signed informed consent. Once enrolled, participants received a fixed acupuncture point protocol, which was administered during visits 1 through 12. At each visit, participants were required to complete a set of self-report questionnaires that assessed changes in the participant's symptoms of anxiety and depression, as well as sexual functioning. The MINI was also re-administered for each study participant (by MV) at visit 12, and at a follow-up 1 month post study completion.
The treatment protocol was developed to treat the two TCM diagnoses most commonly associated with sexual dysfunction based on TCM theory: Heart Yin Deficiency and Kidney Qi Deficiency. 21 Other aspects of the protocol, including the frequency and duration of treatment and the acupuncture point selection, were based on two previous studies, which showed improvement in sexual dysfunction. 1,2
All acupuncture treatments were performed by one of the primary research investigators (ML), a licensed Naturopathic Doctor in the province of Ontario, Canada with at least 500 hours of TCM acupuncture training as part of the Doctor of Naturopathic Medicine program at the Canadian College of Naturopathic Medicine.
Instruments
1. Mini International Neuropsychiatric Interview (MINI): The MINI (Clinician Rated) (MINI CR) is a short, semistructured diagnostic inventory for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and International Classification of Diseases, 10th Revision used to explore 17 Axis I psychiatric disorders. The MINI has good reliability and validity as compared to the Composite International Diagnostic Interview and the Structured Clinical Interview for DSM-IV, but has a much shorter format than the abovementioned and therefore, can be administered in an easy and quick manner 30 and exhibits a high inter-rater reliability κof 0.98. 31
2. Beck Anxiety Inventory (BAI): The BAI is a 21-question self-report tool designed to assess subjective or somatic symptoms of anxiety. 32 The respondent is asked to rate how much he or she has been bothered by each symptom over the past week on a 4-point scale ranging from 0 (“not at all”) to 3 (“severely, I could barely stand it”). Scores are totaled and a total scale score is obtained that corresponds to either minimal (total scores of 0–7), mild (total scores of 8–15), moderate (total scores of 16–25) or severe (total scores of 26–63) anxiety. The BAI has demonstrated high internal consistency (α=0.92) and good test–retest reliability (r=0.75). 32
3. Beck Depression Inventory, Second Edition (BDI-II): The BDI-II is a 21-item self-report instrument intended to assess the presence and severity of depressive symptoms as listed in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. 33 Each item is scored based on increasing severity of depressive symptoms, with scores ranging from 0 to 4. Total scores correspond to either minimal (total score of 0–13), mild (total score of 14–19), moderate (total score of 20–28), or severe (total score of 29–63) depressive symptoms. The BDI-II has high internal consistency (α=0.91) and good test–retest reliability (r=0.93). 34
4. The Sexual Function Visual Analogue Scale (SFVAS): SFVAS (male or female) is a five-item self-reporting tool that assesses sexual function. Each item addresses a component of sexual function. In the male version, these components include desire/libido, erection, orgasm delay, orgasm quality, and frequency of sex. 35 The female version is similar; however, erection is replaced by lubrication. Each item is rated on a 10-cm visual analog scale, where one end corresponds to normal functioning for the respondent, and the other represents the complete absence of function. Respondents are asked to place a line along the 10-cm scale, indicating their rating for each item. Analogue responses are measured and converted into a numerical score. Higher total scores correspond to more normal sexual function. 35
5. The Arizona Sexual Experience Questionnaire (ASEX): The ASEX (male or female) is a self-administered five-question tool that assesses five major aspects of sexual dysfunction. 36 Each of the items asks about the strength or ease of the following components of sexual function: drive, arousal, penile erection/vaginal lubrication (in the male/female versions, respectively), ability to reach orgasm, and satisfaction from orgasm. The respondent is asked to rate each item on a 6-point Likert scale ranging from hyperfunction (1) to hypofunction (6). Total scores range from 5 to 30, with higher scores suggesting greater levels of sexual dysfunction. Cronbach's α analysis indicated that the ASEX demonstrated good internal consistency and scale reliability (α=0.90). The measure also demonstrated strong test–retest reliability when comparing patients and controls (patients, r=0.80, p<0.01; controls, r=0.89, p<0.01). 36
Acupuncture treatment
One-inch 34-gauge disposable stainless-steel needles bearing brand name Huan Qiu were inserted and left for a total of 15 minutes at nine common acupuncture points for 12 sessions. According to the TCM technique, five of the points were “tonified,” using a thrusting and rotation action in the clockwise direction at the 5- and 10-minute mark: Kidney 3 (bilateral), Governing Vessel 4, Urinary Bladder 23 (bilateral). The “neutral method,” during which the needles are left untouched for the duration of treatment, was applied with Heart 7 (bilateral) and Pericardium 6 (bilateral). The correct placement of the needle was confirmed by the sensation known in TCM as de qi. It can be described as a sudden feeling of soreness, numbness, distension, or heaviness in the deep tissue, experienced initially once the inserted needle has reached a certain depth. 1 Subsequent treatments were as identical in method as possible.
Statistical analysis
Changes from pre- to post-treatment in scores from the BAI, BDI-II, SFVAS, and ASEX were analyzed using a paired t-test, with αset at the 0.05 level. All statistical analyses were completed using intention to treat; the last observation was carried forward through the 12 weeks of treatment. When changes in scores were analyzed between the final treatment session and the 1-month follow-up session, only participants who completed both sessions were included in the analysis. All analyses were completed using a computer software program, the Statistical Package for the Social Sciences.
Results
The 35 subjects enrolled in the study included 18 men and 17 women. The mean age at the time of referral was 41.6 (standard deviation=12.8) years. The average number of diagnoses met by patients enrolled in the study was 3.7, with Generalized Anxiety Disorder and Social Anxiety Disorder being the most common diagnoses (present in 85.7% and 45.7% of participants, respectively). Figure 1 illustrates the frequency with which each diagnosis occurred among the sample. All patients were taking either an SSRI or an SNRI at the time of enrollment and reporting sexual dysfunction due to its use. The most common medications were citalopram, paroxetine, and venlafaxine, as illustrated in Figure 2. The mean number of psychiatric medications taken by each participant was 1.51.
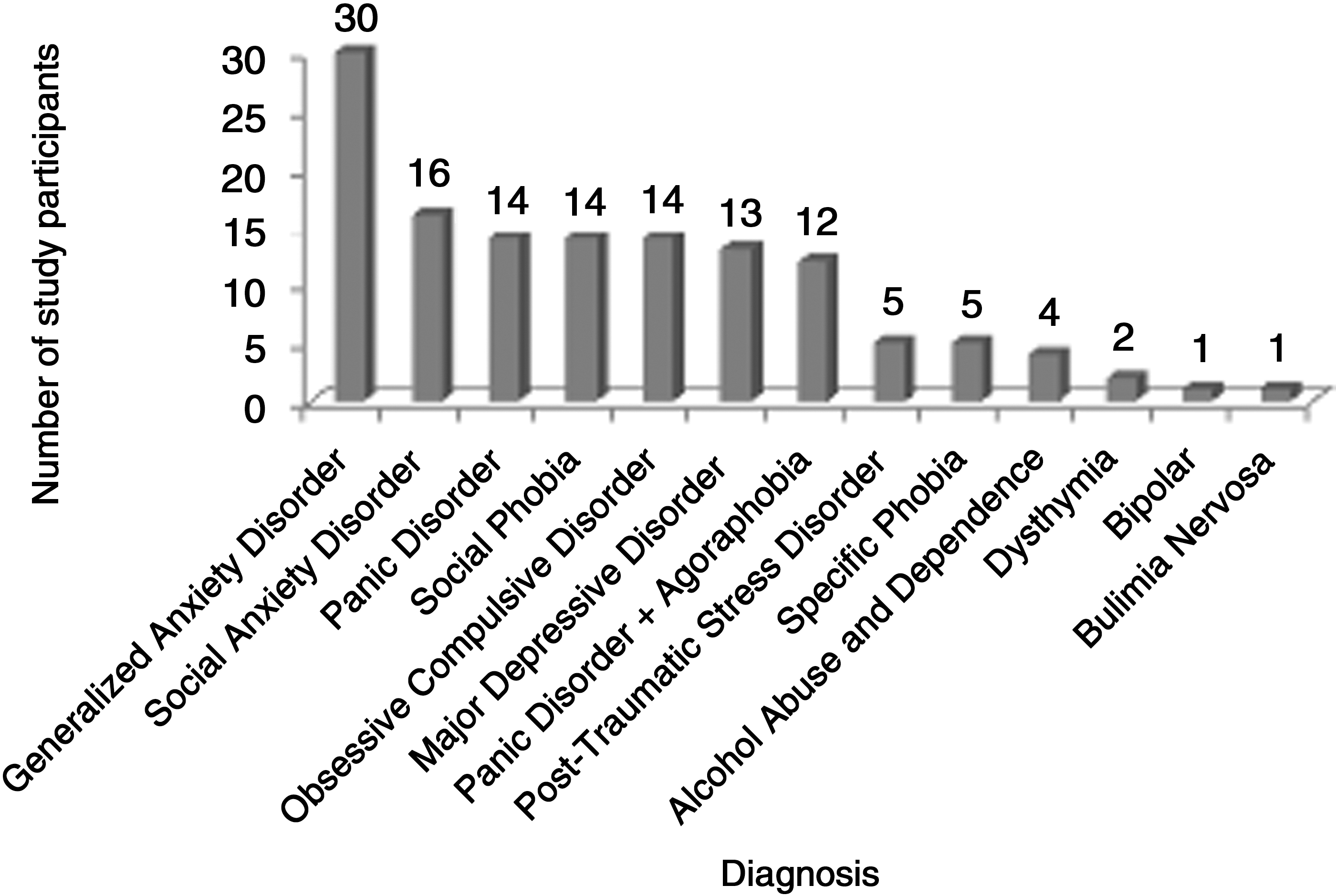
Frequency of psychiatric diagnoses among study participants at the time of enrollment.
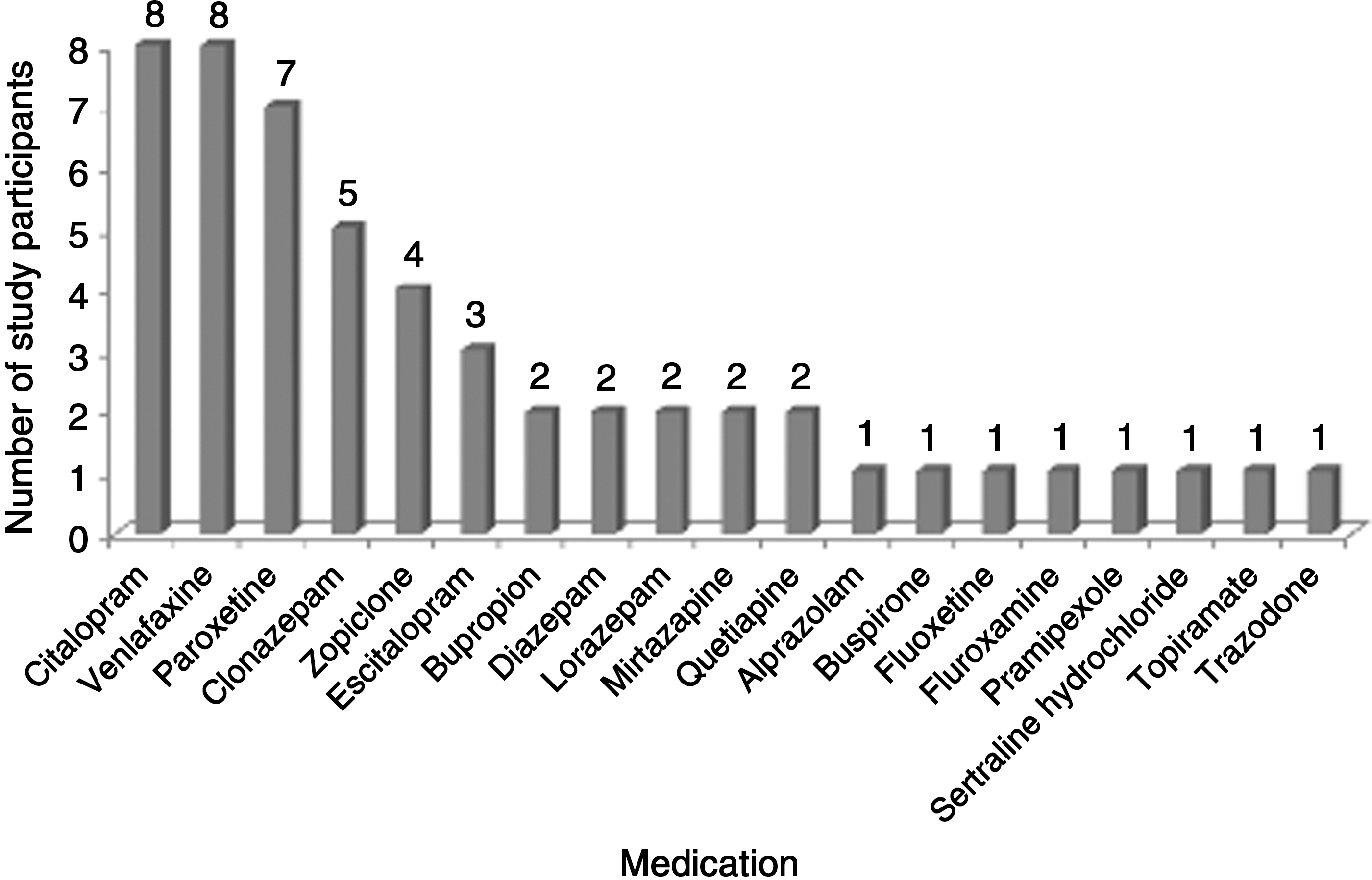
Number of participants using each psychiatric medication at the time of enrollment.
Twenty-nine of the 35 enrolled participants completed the study; however, nine patients missed one treatment session. The reasons for premature termination by the participant included inability to attend weekly appointments (either due to their work schedule or high levels of social phobia) and an inability to tolerate further acupuncture. Thirteen participants completed the post-treatment session 1 month following the final treatment.
Several significant improvements were observed among participants, particularly among males (Table 1). On the SFVAS, the mean score among all participants increased from 162.00 (±77.57) at baseline to 224.28 (±115.45) after 12 weeks of treatment (p<0.001), corresponding to a significant improvement in function. On the ASEX, the overall mean score decreased from 19.49 (±4.61) to 17.91 (±4.70) (p=0.027), corresponding to more normal function. For males, scores on the SFVAS significantly increased from pre- to post-treatment (p=0.001), while ASEX scores significantly decreased from pre- to post-treatment (p=0.017). In females, scores on the SFVAS demonstrated a nonsignificant trend toward increasing from pre- to post-treatment (p=0.067); however, ASEX scores did not display significant changes from pre- to post-treatment (p=0.384).
Statistically significant improvement from initial score (p<0.05).
BAI, Beck Anxiety Inventory; BDI-II, Beck Depression Inventory, Second Edition; SFVAS, Sexual Function Visual Analogue Scale; ASEX, Arizona Sexual Experience Questionnaire; SD, standard deviation.
Certain aspects of sexual functioning benefited more from the acupuncture treatment among male and female participants (Tables 2 and 3, respectively). Scores from male participants increased significantly in all five categories of the SFVAS, and decreased significantly in three of five categories (Drive, Erection, and Ability to Orgasm) on the ASEX. Among female participants, significant improvements were only observed in the SFVAS item related to Desire/Libido and Lubrication, and on the ASEX item related to Lubrication.
Statistically significant improvement from initial score (p<0.05).
Statistically significant improvement from initial score (p<0.05).
Significant improvements were discovered from pre- to post-treatment among male participants on assessments of anxiety and depressive symptoms (Table 1). Mean BAI scores decreased from 7.88 (±5.80) to 5.00 (±5.02) (p=0.010), while mean BDI-II scores decreased from 9.94 (±7.86) to 7.61 (±8.73)(p=0.040). The female participants reported a reduction in depression and anxiety symptomatology; however, neither change reached statistical significance (Table 1).
For participants who completed the follow-up session (N=13), scores at the end of treatment were compared to those at the 1-month follow-up. Statistical analyses revealed no statistically significant differences in scale measures (Table 4). When looking at the trend after the discontinuation of treatment, it is noted that there is a slight increase in mean depression and anxiety scale ratings—corresponding to worsening symptoms—and in mean sexual function scale ratings; however, the results were not significant. Among men, improvement in the ASEX score demonstrated a trend toward statistical significance, despite the small sample size (p=0.058).
Only those participants who completed the follow-up were included.
Discussion
Sexual dysfunction is a significant challenge for many patients using SSRIs or SNRIs to treat symptoms of depression or anxiety. The purpose of this study was to assess the potential therapeutic benefit of acupuncture treatment to alleviate symptoms of sexual dysfunction as a side-effect of pharmacological treatment. It was discovered that male patients benefited from the acupuncture treatment, as they reported significant improvements in several aspects of sexual function as well as a decrease in anxiety and depressive symptoms. Female patients benefited with respect to some of the components of sexual function measured, including desire and lubrication.
The concomitant improvement in sexual function and mental health can potentially be explained in several ways, as it is well established that these two aspects of health are intimately connected. It may be that the acupuncture treatment directly improved sexual function, which resulted in a decrease in depressive and anxiety symptoms. An alternative explanation would suggest that the acupuncture treatment may have caused a decrease in depression and anxiety, which resulted in an improvement in sexual function. Potentially, a third explanation suggests the treatment may have directly improved both mental health and sexual function. Further investigation should be conducted to elucidate the precise mechanism of improvement in these two areas of health.
Comparison of the severity of symptoms at the end of the trial with those at a 1-month follow-up did not reveal a statistically significant change. This may be due to the small sample size at follow-up and the large variance among the population. It is interesting to note that despite a small increase in mean anxiety and depressive symptoms reported by both genders, there was also a small improvement in the mean sexual function scores. Although these improvements were not significant, this finding warrants further study; if acupuncture treatment is able to produce changes in sexual function that are maintained or further improved after the end of treatment, it would make this treatment a highly useful clinical tool. In clinical practice, the individual patient's need for continued acupuncture treatments is periodically reassessed. In some cases, the patient may be able to stop treatment after a course of acupuncture sessions or they may require ongoing treatment at the same or a reduced frequency. There are many possible explanations for the poor rate of participation in the follow-up for this study. Explanations may include a worsening in the patients' condition, or the inconvenience of scheduling and making time to attend an appointment. Assessment of post-treatment changes in sexual function in a larger fraction of participants is needed as part of further studies to assess this trend.
It was observed that the female participants benefited less from the treatment provided. One possible explanation for this difference may have been the severity of illness. At baseline, female participants had higher scores on the BAI, the BDI-II, and the ASEX, and lower scores on the SFVAS, which all correspond to poorer functioning. It is possible that acupuncture is more beneficial to patients with less severe sexual dysfunction symptoms, or that longer treatment or more sessions might have created a more significant response in women. Alternately, it may be that female patients benefit less from this acupuncture treatment.
A benefit of this intervention was the low level of side-effects reported. In terms of adverse events, two patients reported mild soreness at the site of needle insertion, two reported some local bruising, one reported an electrical sensation, one reported a brief episode of muscle twitching, and one reported feeling more emotional after the initial treatment. One patient consistently reported a reduction of sexual interest and an increase in anxiety throughout the treatment period. A few other patients reported an occasional, temporary worsening of sexual function, but the vast majority of comments at follow-up visits reported increased relaxation, improved mood, energy, and well-being, as well as improved sexual function.
There were several limitations to the study design, which may have affected the results obtained. First, the trial was open label and all participants knew that they were receiving treatment, potentially creating an expectation bias. Additionally, no control subjects were used for comparison, and the number of participants was relatively small.
Another limitation involves the choice of acupuncture points used in the treatment protocol (the points selected were the same for all participants). This process would not be representative of conventional TCM clinical practice where protocols are customized to the individual case presentation. Besides Heart Yin Deficiency and Kidney Qi Deficiency, other patterns of disharmony may have been present and would have been addressed by the acupuncture protocol. Perhaps the points selected may have been better suited for the men in the study than the women, suggesting that site selection bias rather than gender could account for the differences in results between men and women.
Conclusions
Based on this preliminary study, it appears that acupuncture may be beneficial at alleviating sexual dysfunction secondary to SSRI or SNRI use, particularly in male patients. Future investigations in the form of randomized, double-blind, controlled trials will likely be required for the next step. Future studies might examine comparisons of individualized treatment protocols and more standardized protocols (like this one, where all people receive the same acupuncture treatment), to further elucidate the potential role for acupuncture in the treatment of SSRI- and SNRI-induced sexual dysfunction.
While more research is required, these preliminary results suggest that the integration of traditional psychiatric medicine with more complementary and alternative treatments involving collaboration between medical and complementary and alternative practitioners has the potential to significantly improve patient outcomes.
Footnotes
Acknowledgments
We would like to acknowledge the contribution of the clinic volunteers in completing the data entry required for this study.
This study was carried out in accordance with the ethical standards of the Declaration of Helsinki 1975. The study design was approved by the Research Ethics Board at the Center for Addiction and Mental Health.
Disclosure Statement
No competing financial interests exist.