
Abstract
Objective:
To determine the effects of participation in a 2-year community-based dance class on disease severity and functional mobility in people with Parkinson disease (PD).
Design:
Randomized controlled trial.
Settings/Location:
Dance classes took place in a community-based location. Outcome measures were collected in a university laboratory.
Patients:
Ten individuals with PD were randomly assigned to the Argentine tango (AT) group (n=5 [4 men]; mean age±standard deviation, 69.6±6.6 years) or the control group (n=5 [4 men]; mean age±standard deviation, 66±11.0 years).
Interventions:
The AT group participated in a community-based AT class for 1 hour twice weekly for 2 years. Control group participants were given no prescribed exercise. Blinded assessments occurred at baseline and 12 and 24 months.
Outcome measures:
Movement Disorder Society-Unified Parkinson Disease Rating Scale (MDS-UPDRS) III, Mini-Balance Evaluation Systems Test (Mini-BESTest), gait velocity (forward and backward), Timed Up and Go and dual-task Timed Up and Go, Six-Minute Walk Test (6MWT), MDS-UPDRS II, MDS-UPDRS I, and Freezing of Gait Questionnaire.
Results:
There were no differences between groups at baseline. A significant group-by-time interaction (F [2,8]=17.59; p<0.0001) was noted for the MDS-UPDRS III, with the AT group having lower scores at 12 and 24 months than the controls. Significant interactions were also noted for the Mini-BESTest, MDS-UPDRS II and I, and 6MWT.
Conclusion:
This is believed to be one of the longest-duration studies to examine the effects of exercise on PD. Participation in community-based dance classes over 2 years was associated with improvements in motor and nonmotor symptom severity, performance on activities of daily living, and balance in a small group of people with PD. This is noteworthy given the progressive nature of PD and the fact that the control group declined on some outcome measures over 2 years.
Introduction
P
Pharmacologic treatments, most commonly carbidopa/levodopa, are useful in reducing tremor and rigidity in people with PD; however, the effects of medications on balance and gait are less clear. 10 –12 In addition to pharmacologic treatment, surgical intervention known as deep brain stimulation has also been used with the goal of reducing motor symptom severity in people with PD. However, postural instability and gait difficulty are improved by deep brain stimulation to the same extent as the other cardinal symptoms of PD. 13 As such, nonpharmacologic and nonsurgical interventions are needed to address balance and gait deficits for patients with PD.
Exercise has been supported as an effective adjunct therapy to the traditional pharmacologic treatments. Common forms of exercise used for people with PD, which include treadmill, resistance, balance, and cueing training have been reported to improve gait and balance and reduce overall disease severity for people with PD. 14 –17 Despite these benefits, an individual's ability to consistently exercise may be hindered by the notion that this mode of exercise is not sufficiently appealing or socially engaging. This creates the need for physical therapists and other healthcare professionals to devise ways to keep exercise interesting and interactive to promote long-term adherence to exercise.
Dance is another form of exercise that can challenge gait and balance impairments in those with PD. Many modes of dance include walking as a primary step, which encourages task-specific practice. Challenges to dynamic balance are often incorporated in dance as the participant has to accommodate to a constantly changing environment while moving. 18 Additionally, investigators have reported that older adults believe dance is more enjoyable than traditional exercise, in turn promoting adherence and motivation to exercise. 19 However, most programs that have been studied have lasted 3 months or less, and only one has studied the effects of dance on functional mobility in PD for more than 1 year. 20,21 We previously reported in a randomized controlled trial that participation in a community-based dance program over 1 year led to significant improvements in many aspects of functional mobility. 22 However, it is unclear whether these improvements would be maintained if dance participation were continued for an additional year.
The purpose of this study was to determine the effects of participation in a 2-year community-based dance class on functional mobility in people with PD. We hypothesized that gains noted at 1 year would be maintained with continued dance participation for an additional year and that function in controls would continue to decline over the course of the study.
Methods
Participant recruitment
Participants were recruited through the Washington University School of Medicine's Movement Disorders Center as a part of a larger randomized controlled trial. 22 Participants were included if they had received a diagnosis of “definite” idiopathic PD, were older than age 40 years, and were receiving levodopa medication. 23 Phone interviews were conducted before baseline assessment to determine whether the participant was eligible for the study according to the following exclusion criteria: (1) a serious medical condition, (2) history or evidence of neurologic deficit other than PD, (3) evidence of brain abnormality other than PD-related changes on brain imaging (previously done, not a part of this study), or (4) history or evidence of a musculoskeletal problem that limited movement. All eligible participants provided written informed consent in accordance with the policies and procedures of the Human Research Protection Office at Washington University.
Study design
Before the baseline assessment, participants were randomly assigned to the Argentine tango (AT) or control groups. Those assigned to the AT group were informed that they were to participate in twice-weekly, 1-hour community-based dance (AT) classes. AT was chosen because previous studies showed that it conveyed more benefits with respect to physical function for people with PD when compared with more common forms of exercise. 24 Classes were instructed by two volunteers with extensive experience in the performance of AT. Control group participants were given no prescribed exercise. They were instructed to maintain their current levels of physical activity during the study, and none of them reported any form of dancing as part of their normal activities. Before completion of the dance class at 1 year, AT participants were given the option to continue dancing for an additional year. Control patients who were matched by age, sex, and Movement Disorder Society-Unified Parkinson Disease Rating Scale (MDS-UPDRS) III score to AT participants who chose to continue dancing were also followed over the second year of the study. All participants agreed to complete evaluations at baseline and 12 and 24 months.
Outcome measures
The gold standard for measuring PD nonmotor and motor symptom severity, as well as the influence of PD symptoms on performance of activities of daily living (ADLs), is the MDS-UPDRS. 25 Sections I–III of the MDS-UPDRS were used in this study. Nonmotor symptoms were assessed by using the MDS-UPDRS I. 25 This section includes 13 items, and scores for each item range from 0 (no symptoms) to 4 (severe symptoms), with a total possible score of 52. A higher score indicates a greater degree of nonmotor symptom severity.
Performance of ADLs was assessed by using the MDS-UPDRS II. 25 This questionnaire is composed of 13 items. Each item presents an ADL and requires the participant to report on the difficulty experienced when attempting to perform that ADL. A score of 0 represents no difficulty completing the ADL, while a 4 represents severe difficulty. The ADLs assessed in the MDS-UPDRS II include, but are not limited to, speech, chewing/swallowing, dressing, grooming, and eating.
The MDS-UPDRS III was used to assess motor symptom severity in patients with PD. 25 This measure includes 33 items, individually scored on a scale of 0–4, with 4 representing the highest degree of severity. The maximum possible score is 132. From this assessment, participants were assigned a Hoehn and Yahr (H&Y) stage.
Balance was assessed using the Mini-Balance Evaluation Systems Test (Mini-BESTest). 26 This tool comprises 14 balance tasks, which are scored on a scale of 0–2. A score of 2 on an item represents no impairment in balance. The maximum possible score is 32 because two items have left and right components, and higher scores indicate better balance.
Using a GAITRite ® (CIR Systems, Sparta, NJ) walkway, walking velocity was assessed. Gait velocity was collected during forward and backward walking. Three trials of each condition were averaged to determine mean gait velocity. For both forward and backward walking, participants were instructed to walk at their normal, comfortable pace. Other measures collected related to gait included the Timed Up and Go (TUG), dual-task TUG, Six-Minute Walk Test (6MWT), and Freezing of Gait Questionnaire (FOGQ). 27 To complete the dual-task TUG successfully, participants performed the TUG while saying aloud random numbers between 0 and 100.
Assessment protocol
Participants were assessed while they were off anti-PD medication (i.e., 12 or more hours since last administration) at baseline, 12 months, and 24 months. A trained physical therapist, blinded to group assignment, completed all evaluations. Using custom designed forms, the rater gave all participants the same instructions at each evaluation. All outcome measures were administered in the same order at each visit: (1) MDS-UPDRS I, (2) MDS-UPDRS III, (3) Mini-BESTest, (4) gait velocity (forward and backward), (5) TUG and dual-task TUG, and (6) 6MWT. The questionnaires (MDS-UPDRS II and FOGQ) were completed by the participants before each evaluation and checked for completion by the rater.
Data analysis
Descriptive statistics were used to describe mean sample characteristics for age, sex, and MDS-UPDRS III and to characterize H&Y stages. To test for differences between groups at baseline, independent sample t-tests were used for age and MDS-UPDRS III scores, and Mann–Whitney U tests were used for sex and H&Y stage. Repeated-measures analyses of variance (2×3) were used to examine main effects of group (AT versus control) and time (baseline, 12 months, 24 months), as well as group-by-time interactions. Tukey–Kramer post hoc tests were then used as warranted. Main effects or interactions were considered significant at α ≤0.05. All analyses were conducted by using NCSS software (NCSS LLC, Kaysville, UT).
Results
In total, 10 participants, 5 in the AT group and 5 in the control group, completed evaluations at baseline, 12 months, and 24 months. Mean ages±standard deviation were 69.6±6.6 years in the AT group and 66±11.0 years in the control group (Table 1). At baseline, the mean number of years since PD diagnosis for the AT group was 6.6±7.5 years. The control group was diagnosed with PD a mean of 11±3.9 years before the baseline assessment. Demographic characteristics at baseline did not differ between groups.
Tango and control participants are matched by number.
F, female; H&Y, Hoehn and Yahr; M, male; PD, Parkinson disease.
Regarding disease severity measures, there was no difference between groups for the three MDS-UPDRS measures at baseline. Significant main effects of group (F [1,8]=5.99; p=0.04), time (F [2,8]=9.98; p=0.001), and a group-by-time interaction (F [2,8]=17.59; p<0.0001) were noted for the MDS-UPDRS III. Within the AT group, MDS-UPDRS III scores at 12 and 24 months were lower (i.e., better) than at baseline, but there was no difference between scores at 12 and 24 months. At 12 and 24 months, MDS-UPDRS III scores for the AT group were significantly lower (i.e., better) than for controls at all three time points. Significant interactions between group and time were noted for the MDS-UPDRS II (F [2,8]=3.53; p=0.05) and I (F [2,8]=5.10; p=0.02). MDS-UPDRS II scores for the AT group at 12 and 24 months were significantly lower (i.e., better) than for controls at 24 months. There were no within-group differences for either group for MDS-UPDRS II scores. MDS-UPDRS I scores for the AT group at baseline were significantly different from those for controls at 12 months. At 12 and 24 months, the AT group reported significantly lower nonmotor symptom severity compared with controls at 12 months and 24 months (Fig. 1).

Movement Disorder Society-Unified Parkinson Disease Rating Scale (MDS-UPDRS) III
There was no difference between groups on the Mini-BESTest at baseline. A significant interaction between group and time was noted for the Mini-BESTest (F [2,8]=11.33; p<0.001). At 12 months, the AT group had significantly higher (i.e., better) balance scores than the control group at 12 and 24 months. The AT group at 24 months had significantly better scores than the control group at all time points. Within the AT group, Mini-BESTest scores were significantly better at 12 and 24 months compared with baseline, but there was no difference noted for 12 versus 24 months (Fig. 2).
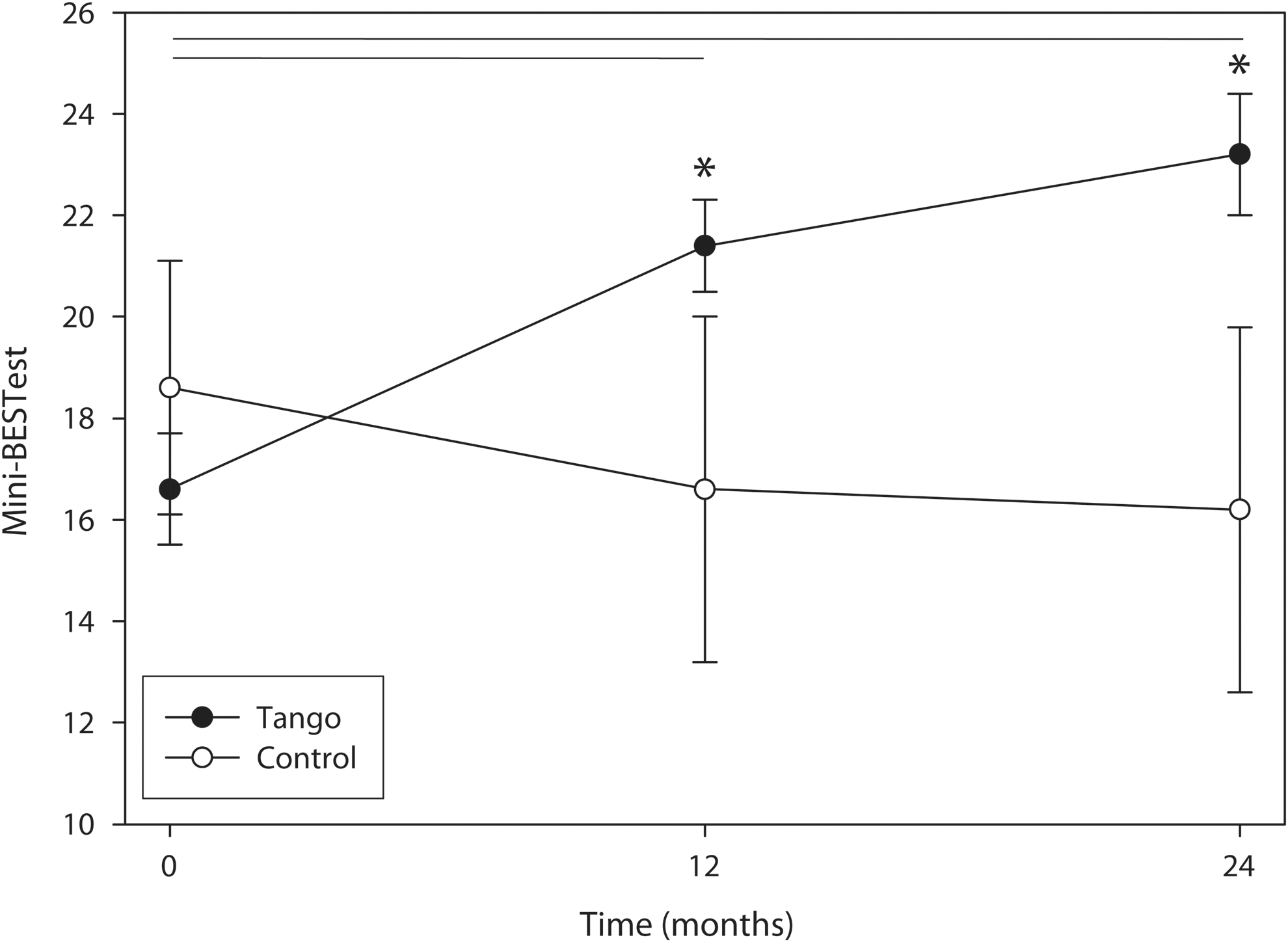
Mini-Balance Evaluation Systems Test Mini-BESTest scores at baseline and 12- and 24-month evaluations for the Argentine tango (AT) (filled circles) and control (open circles) groups. Values are means±standard error of the mean. Asterisks denote significant differences between AT and control groups within that time point. Each horizontal line indicates a significant difference within the AT group between the two time points spanned by the line.
For all gait measures, there was no difference between groups at baseline. No significant main effects or interactions were noted for forward walking velocity, backward walking velocity, TUG, or FOGQ. For the dual-task TUG, a significant interaction between group and time was noted (F [2,8]=3.7; p=0.048), with AT improving dual-task TUG performance over time and control performance worsening over time, but there were no significant differences between groups at any time point. There was a significant main effect of time (F [2,8]=11.33; p<0.001) and a significant group-by-time interaction for the 6MWT (F [2,8]=5.67; p=0.013). The AT group at baseline and 12 months walked significantly greater distance in 6 minutes compared with the control group at 24 months. There were no within-group differences in the AT group; however, 6MWT distance of the control group at 24 months was significantly lower compared with baseline and 12 months (Fig. 3). Table 2 presents a simplified summary of results.

Forward walking velocity
AT, Argentine tango; MDS-UPDRS, Movement Disorder Society-Unified Parkinson Disease Rating Scale; TUG, Timed Up and Go.
Discussion
This is believed to be the first study to determine whether improvements in disease severity, balance, and functional mobility gained through AT dancing for 1 year, which have already been demonstrated, can be maintained or increased if patients with PD continue to dance for an additional year. 22 The primary outcome measure for this study was the MDS-UPDRS III because it is the gold standard used by many neurologists to assess PD motor symptom severity. The substantial improvements at both 12 and 24 months in MDS-UPDRS III for the AT group exceed both the minimal detectable change and the substantial minimal clinically important difference for the MDS-UPDRS III. 28 As expected, the control group did not improve at any time point and actually had a 6-point worsening in MDS-UPDRS III score, although this was not significantly different from baseline. These findings agree with those reported in a previous randomized controlled trial that assessed individuals off anti-PD medication after participation in a year-long AT class. 22
The gains noted in the MDS-UPDRS I score, which reflects reduced nonmotor symptom severity, for the AT group suggest that dance may not only improve motor symptoms of PD but also have a positive effect on nonmotor symptoms. Steffen and colleagues noted similar improvements in people with PD after long-term treadmill training. 29 Although not extensively studied, this suggests that exercise, in any form, may have a generalized effect on nonmotor symptom severity in PD. Improvement in MDS-UPDRS II scores, reflecting less difficulty with ADLs, for the AT group over time might have been related to reductions in motor symptom severity and improvement in balance, both of which could positively affect ability to perform many ADLs.
Regarding mobility measures, we suspect that the improved Mini-BESTest scores for the AT group can be attributed to dance because the intervention incorporates many challenges to balance through starting, stopping, and frequent directional changes. 18 Duncan and Earhart reported a similar increase in Mini-BESTest scores after 1 year of AT in people with PD. 22 The AT group demonstrated improvements in forward and backward walking velocity at 24 months compared with baseline, while velocity in controls declined. Significant increases in forward walking velocity and nonsignificant increases in backward walking velocity after individuals danced for 1 year have been previously reported. 22 It is also important to note that AT group demonstrated reductions in both forward and backward walking velocity from 12 months to 24 months, which suggests that these improvements might be reduced with time or that the intensity of the AT dance class was insufficient for maintaining the improvements noted at 12 months. The significant interaction noted for the 6MWT was probably due to the substantial reduction in distance walked by the control group at 24 months. The maintenance of 6MWT in the AT group (31.4-meter reduction) was in contrast to the steeper decline noted in the control group (151.8-meter reduction). The slowed decline in those who danced may be related to engaging in regular physical activity, which might positively influence cardiovascular endurance. Improved balance might be another factor that led to less decline in 6MWT distance for the AT group, as Falvo and Earhart have reported that balance significantly affects 6MWT performance. 30
Findings reported in this study should be interpreted with caution in light of several limitations. First, individuals in the AT group were given the option of continuing to dance after 1 year and as such represent those motivated to continue participating, while those who decided to stop dancing after 1 year were lost to follow-up. This represents a potential source of participant bias in which it is possible that only patients experiencing benefits from dancing continued. Second, the sample size was relatively small given the pilot nature of this study. Despite this small sample size, strict matching criteria were implemented for participants in the two groups. Finally, organizing and conducting these community-based dance classes can be difficult, for several reasons. The cost of these classes, including compensation for expert instructors, was supported by grant funding. As such, the classes were offered at no charge to participants. Transportation to and from the classes was not provided in any capacity; however, the participants relied on spouses, caregivers, and/or carpooling with other participants in the class to ensure regular attendance.
In the future, investigators should attempt to implement larger-scale community-based exercise classes and track outcomes for those with PD over the long term. To further understand which types of exercise may convey more substantial benefits for individuals with PD, it is imperative that investigators compare different modes of exercise over time in people with PD. Finally, through the use of neuroimaging, investigators should begin to study the neurologic mechanisms underlying the functional improvements in those with PD after dance and other forms of exercise.
Conclusion
Participation in community-based AT classes over 2 years led to improvements in motor and nonmotor symptom severity, subjective ADL performance, and balance in a small group of people with PD. All gains were achieved by the 12-month time point. Although no additional improvements were noted from 12 to 24 months, most gains were maintained at 24 months. This is noteworthy given the progressive nature of PD and the fact that participants in the control group showed no improvements and in fact declined on some outcome measures after 2 years. Of the long-term exercise studies, this appears to be one of the longest-duration interventions yet to be studied. 31,32 This and other studies continue to support the importance and potential impact of exercise in the management of PD, and support the notion that exercise should be adopted by individuals with PD for the duration of the disease.
Footnotes
Acknowledgments
This study was funded by the Parkinson's Disease Foundation. General support for the second year of dance classes was also received from the Greater St. Louis Chapter of the American Parkinson Disease Association (APDA) and the APDA Center for Advanced PD Research at Washington University. Thanks to Ruther Porter, DPT, John Michael Rotello, Robin Girard, and Maya Matheis for AT class instruction, and to the many volunteers who assisted in the AT classes.
Author Disclosure Statement
No competing financial interests exist.