
Abstract
Objective:
This study was performed to characterize the physiologic effects of rhythmical massage (RM), an anthroposophic therapy whose effectiveness is supported by empirical observations and a prospective observational study.
Methods:
Patients referred to RM at the Paracelsus Hospital Richterswil for any indication were continuously enrolled. They received an average of 10 RM sessions, which included not only the massage but also therapeutic rest in the supine position immediately thereafter. Effects of RM on surface temperature and on heart rate variability (HRV) were determined with infrared imaging (IRI) and electrocardiography (ECG), respectively. IRI of the patients' dorsal region was performed without clothes, in standing position, at the start and at the end of two waiting periods before and after RM. ECG was performed from the beginning of the first waiting period until the end of the second one.
Results:
Results on IRI from 9 and ECG from 11 patients could be analyzed. RM led to an immediate increase in dorsal temperature. Furthermore, comparison of the IRI images for consecutive RM sessions showed a tendency toward improved warmth distribution as a progressive therapy effect. Analysis of the EGC results recorded during the waiting periods—in the sitting position—-showed a significant increase of HRV after RM, as detected by the standard deviation of the beat-to-beat periods and a relative increase of low-frequency power. During the course of the RM sessions, the change in HRV during the therapeutic rest period depended on the initial value: Low initial values were enhanced, whereas high ones were reduced.
Conclusions:
RM led to an immediate increase in the patient's dorsal surface temperature, as well as increased HRV and sympathetic stimulation. In the long term, RM resulted in a progressive improvement of warmth distribution and regulation of the resting HRV.
Introduction
R
RM is used for acute and chronic conditions and for a wide range of indications, including circulatory, respiratory, digestive, and neurologic disorders; orthopedic conditions; insomnia; migraine; depression; and pain management. Observational studies addressing anthroposophic medicine as a whole system suggest that RM can have clinically relevant effects in chronic conditions. 2 The only prospective cohort study, which specifically addressed the effectiveness of RM, found a long-term reduction of chronic disease symptoms and improvement of overall health status. 3
Infrared imaging (IRI) can be used to study thermoregulation and for diagnostic purposes because various pathologic processes (e.g., tumor-induced cell proliferation, vasodilatation, and angiogenesis) are related to local changes of skin temperature. 4 IRI has been proposed as a noninvasive screening method for detection 5,6 and prognosis determination 7 of breast cancer as well as detection of melanoma. 8 Further applications concern diagnosis and study of thermal instability in premature infants, 9 clinical assessment of peripheral perfusion and tissue viability in diabetes, 10 vascular disorders, 11 and inflammatory processes. 12 Also some movement exercises 13 and therapeutic massage 14 can be associated with changes in skin temperature detectable by IRI.
Measures of the heart rate variability (HRV) analysis in the frequency domain correlate with the activity of the autonomic nervous system. 15 –18 Both sympathetic and parasympathetic activities contribute to the low-frequency band, but only the parasympathetic activity is associated with a higher power density in the high-frequency band. The ratio log (low frequency to high frequency)—the so-called stress quotient—is considered an index of the sympathetic/parasympathetic balance and exhibits high values for mental and physical stress and low values for deep relaxation states. 15 –17 Usually, higher HRV is associated with better health and improved prognosis. Previous studies revealed that two therapies characteristic of the anthroposophic medicine (therapeutic eurythmy 19 and speech therapy 20 ) can favorably influence HRV.
Despite considerable clinical evidence for the effectiveness of RM, no data on its physiological effects are available. Because RM is likely to affect fluid circulation, such as that of blood and lymph, we hypothesized that its application might be associated with changes in skin temperature. Furthermore, because it is used in the clinical praxis to alleviate mental and physical stress, we expected it to favorably affect autonomic balance. The aim of the present study was to determine whether RM triggers measurable changes of body surface temperature and of HRV in patients with different diagnoses. This exploratory study was embedded in a larger cohort study on RM effectiveness.
Materials and Methods
Study design, participants, and therapy
This single-arm prospective exploratory cohort study in a real-world medical setting was performed at the Paracelsus Hospital Richterswil in Switzerland. Its primary objective was to document the effects of RM on body temperature distribution and HRV by IRI and electrocardiography (ECG), respectively. The study was approved by the Ethics Committee of the Canton Zürich, Switzerland, and was conducted according to the principles of the Helsinki Declaration. Written informed consent for participating in the study was obtained from all patients before enrollment. In addition, one patient explicitly consented for IRI publication (Fig. 1). This study was part of a larger, questionnaire-based cohort study on RM, which is still ongoing and within which the patients could accept or decline ECG and/or IRI.
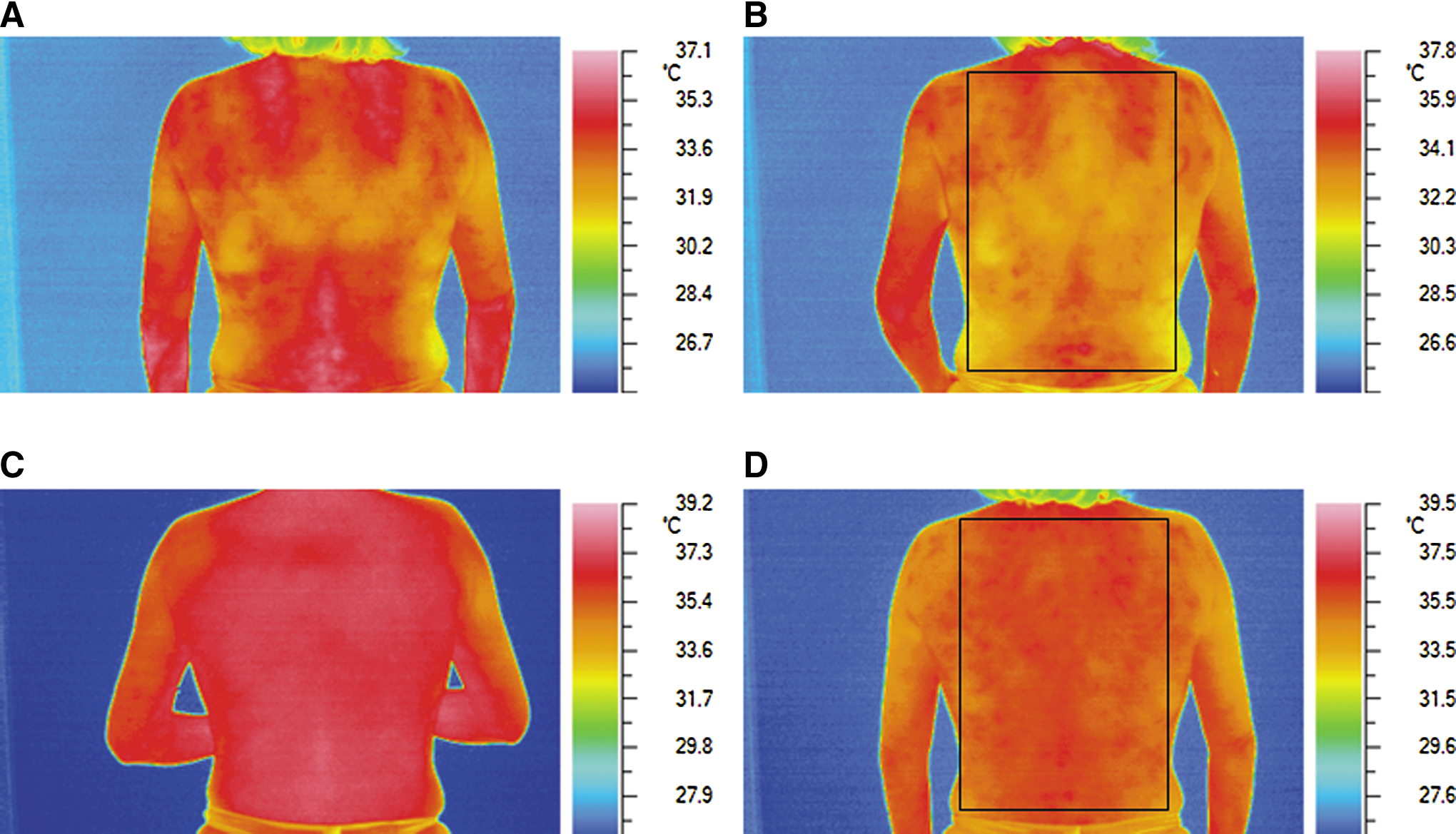
Infrared images of a study patient before and after rhythmical massage (RM). Infrared images of patient's back were taken at four different occasions.
Inpatients and outpatients referred to RM for any indication were continuously enrolled in this study. Exclusion criteria were (1) RM treatment within the 12 months preceding enrollment; (2) age younger than 18 years or older than 75 years; (3) infections with pathogens; (4) fever; (5) furuncles, eczema, and fungi; and (6) burns and open wounds. RM was performed by two experienced RM therapists with certification from the School for Rhythmical Massage of the Ita Wegman Hospital (Arlesheim, Switzerland) and from the Swiss Erfahrungs Medizinisches Register. The study patients received an average of 10 RM sessions (range, 7–16) once or twice weekly. Each session encompassed a 30-minute massage and at least a 20-minute rest period in the supine position. Other therapies and medications were allowed during the RM treatment (from first to last session), and self-reported information on them was collected.
Data collection
Physicians documented eligibility criteria at study entry. IRI and ECG were performed by study investigators (G.S. and C.W.) or by one therapist (B.S.). IRI of the dorsal area was performed at each therapy session at four different time points (see below) with an AVIO TVS 700 camera (Goratec Technology GmbH, Erding, Germany). The camera was mounted on a tripod. For all recordings, the tripod was placed in the same position with respect to the patients, who stood while the dorsal images were obtained.
ECG was performed with an MK3 Scientific ECG device (TOM Medical Entwicklungs GmbH, Graz, Austria) with a 4-kHz sampling rate for beat-to-beat detection (RR-interval recording); the ECG potential data were used to calculate ECG-derived respiration, as well as artifact correction in the time series of normal-to-normal intervals.
The measurements were obtained according to the following sequence. All IRI was done in the standing position. The first IRI images were taken immediately after arrival and undressing. The electrodes were placed on the chest of the patient, and ECG recording was started. After 5–10 minutes in the sitting position, the second IRI set was performed; an RTI therapist performed the individualized massage for 30 minutes, during which the patient was in the supine or the prone position, occasionally alternating. The massage was followed by a therapeutic rest (at least 20 minutes), always in the supine position, during which the patient was covered with a light blanket. The third set of IRI images were obtained right after this therapeutic rest. After 5–10 minutes in the sitting position, ECG recording was stopped, the last IRI set was performed, and the patient dressed and left. The waiting periods in which the patients were seated without clothes allowed for thermal equilibration. They also allowed direct comparison of HRV data collected before and after therapy. Most sessions took place in the morning in a darkened, draft-free therapy room at 20–22°C. The patients were asked to avoid showering, smoking, and drinking tea and coffee before the sessions.
Data analysis
Data analysis was performed on all patients fulfilling eligibility criteria with at least five sets of IRI images or four ECG recordings available for analysis.
For quantitative analysis of IRI, the biggest possible rectangle included in the dorsal area (Fig. 1) was tentatively determined and its temperature profile analyzed by using Thermography Studio 2003 Realtime software (Goratec Engineering, Neufraunhofen, Germany); in particular, maximum (Tmax), minimum (Tmin), and mean temperatures were computed. Data were entered into an Excel spreadsheet (Microsoft Office Excel 2003®; Microsoft, Redmond, Washington) and analyzed using IBM SPSS® Statistics, version 19 (Chicago, Illinois).
Artifact correction and frequency analysis of HRV were performed by using SimpleView© software version 2.2, release 15 (TOM Medical), as well as Kubios-HRV software, version 2.0 (Biosignal Analysis and Medical Imaging Group, University of Kuopio, Kuopio, Finland). All time series of the normal-to-normal intervals were treated with respect to statistical time domain analysis and fast Fourier HRV frequency domain analysis according to the 1996 North American Society of Pacing and Electrophysiology guidelines. 15 The frequency analyses were conducted in 5-minute intervals in the middle of the waiting periods in sitting position, as well as during the period of massage and therapeutic rest. Spectrograms were calculated showing the power density distribution of HRV modulating frequencies over RM, as displayed in Figure 3. The following variables were considered: minimum, mean, and maximum heart rate in beats per minute; respiration in cycles per minute; pulse-respiration quotient; standard deviation of normal-to-normal intervals time series (SDNN); total spectral power (total in ms2); and high-frequency (0.15–0.4Hz), low-frequency (0.04–0.15Hz), and very-low-frequency (0.0033–0.04 Hz) spectral power band densities, as well as stress quotient (log [low frequency/high frequency]). Because body position might influence these variables, only values obtained in the same position (either sitting or lying) were compared.
Statistical significance (p≤0.05) of differences between measurements performed at two different occasions was detected with the paired t-test; statistical tendencies were defined as 0.05<p<0.15 (paired t-test). Unless otherwise specified, data are shown as mean±standard error of the mean.
Results
Patient recruitment
From August 2008 (first patient began treatment on August 23, 2008) to May 2010 (last patient began on May 20, 2010, and ended on October 26, 2010), 18 patients who agreed to undergo IRI and/or ECG were included in the study; 13 of these patients completed the study. Of these, 10 agreed to undergo IRI and 11 to undergo ECG. IRI images from 9 and ECG recordings from 11 of these patients could be analyzed.
Baseline characteristics
Table 1 shows the characteristics of the 12 patients whose IRI and/or HRV data were analyzed. The mean patient age was 54.8±3.8 years (range, 34–69 years), and most patients were women (10 of 12). The most frequent main diagnoses were malignant neoplasms (n=6; diagnostic codes C00–D48 according to the International Classification of Diseases, Tenth Edition) and mental diseases (n=2; F00–F99). The most frequent symptoms were sleep disorders (n=6), back pain (n=5), joint pain (n=3), exhaustion (n=3), and depression (n=2) (not shown). Eight of the 12 patients reported using adjunctive therapies for the same therapeutic goals for which they underwent RM (mostly anthroposophic and/or other complementary and alternative therapies [Table 1]). The main goals of RM as stated by the therapists were to relax (n=12), warm (n=8), deepen and improve the breathing (n=7), and increase body awareness (n=2). Massage was always performed with massage oil or cream, in most cases peat-fiber oil (n=10). The massaged areas differed from patient to patient and are shown in Table 1 for each patient by order of importance.
As reported by the patients at the beginning and/or end of the treatment period in answer to the question “Are the goals of RM [rhythmical massage] also being treated with other therapies?”
As reported by the RM therapist for each massage, in order of importance.
Patients 9 and 11 received an infusion right after RM and had no sitting period after treatment.
HRV, heart rate variability; ICD-10, International Classification of Diseases, 10th Revision; IRI, infrared imaging; RM, rhythmical massage.
Temperature distribution
IRI images from 9 patients and 70 RM sessions overall were available for analysis. Figure 1 shows a typical sequence of IRI made during one session and therefore concerns short-term effects of RM. Figure 1A was obtained immediately after the patient had undressed and shows an uneven temperature distribution, with cold regions and warm spots. After 5–10 minutes of sitting (Fig. 1B), the temperature distribution becomes more homogenous; the average temperature is lower than upon arrival. Figure 1C, obtained after the complete RM treatment (i.e., after massage and therapeutic rest), reveals surface temperatures higher than before RM; in contrast to parts A and B, the temperature distribution is very homogenous. After an additional 5–10 minutes of sitting (Fig. 1D), the mean temperature is lower than in part C but still higher than in parts A and B; moreover, the temperature distribution is still clearly more uniform than in parts A and B. Considering all IRI images together, Tmax immediately before RM was 36.0±0.81°C, Tmin 31.9±1.43°C. After RM, both measures increased markedly, up to 36.7±0.60°C and 33.9±0.86°C, respectively (p<0.001).
Figure 2 shows how several aspects of average dorsal temperature varied during the course of the therapy sessions, illustrating long-term effects of RM. Both Tmin and Tmax measured before RM tended to increase over the therapy course (Fig. 2A). Tmin after RM increased slightly with increasing number of RM sessions, whereas Tmax tended to decrease (Fig. 2B), resulting in a decrease of temperature amplitude after RM (Tmax-Tmin, Fig. 2C). In contrast, temperature amplitude before RM remains more or less constant over the whole therapy course (Fig. 2C). To correct for possible differences in the initial conditions, the temperature amplitude before RM was subtracted from the temperature amplitude after RM; a trend toward more negative values with increasing therapy session number could be observed (Fig. 2D). A similar trend was apparent in most patients (6 of 9). At therapy beginning (first session), the differences in temperature amplitude ranged from −2.1°C to −0.2°C (−1.07°C±0.45°C); at therapy end (last session), the values ranged from −3.3°C to −0.4°C (−1.76°C±0.63°C). When these values were compared for all patients at the first and the last treatment session, a statistical tendency for a reduction could be detected (p=0.102).
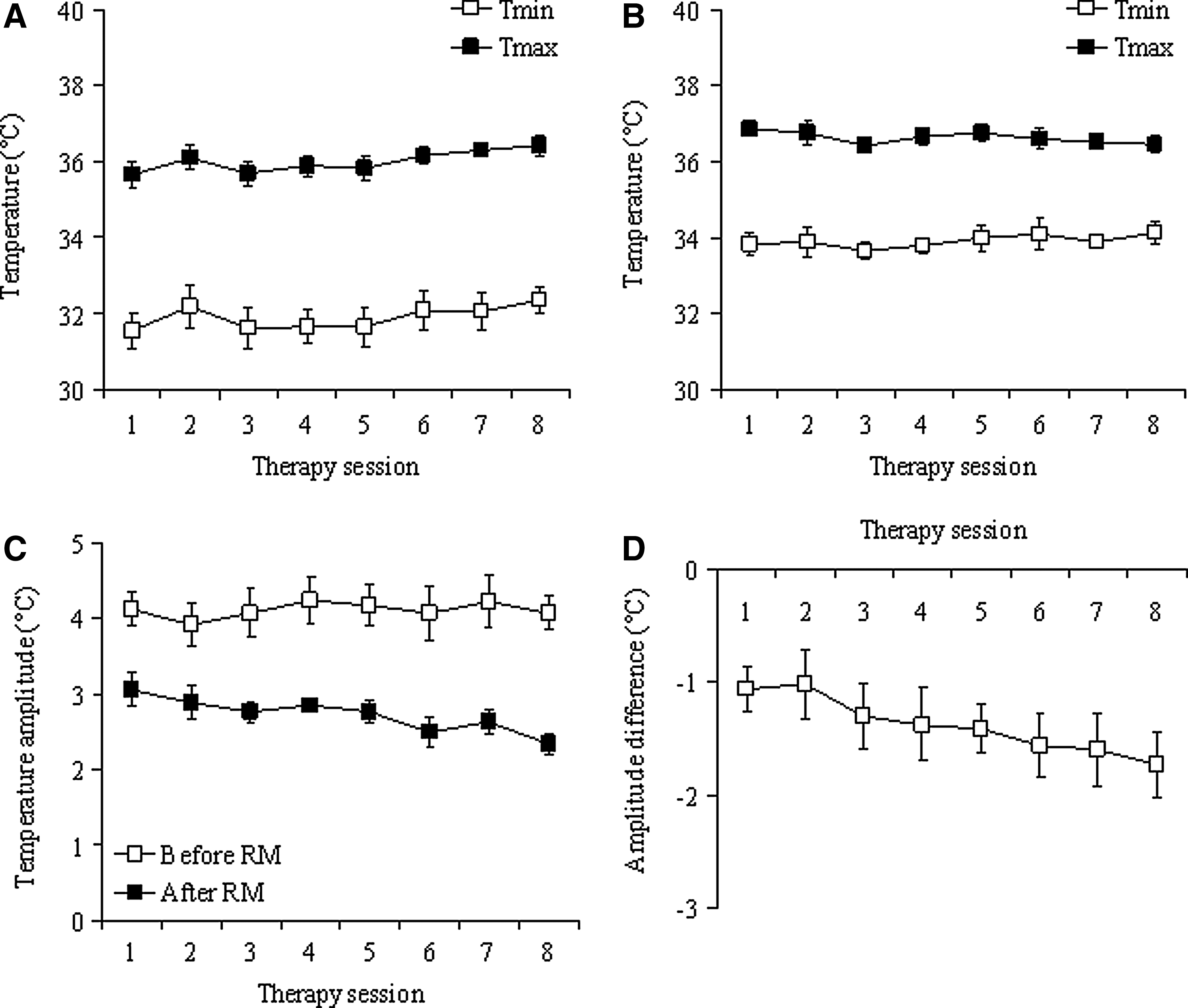
Mean values of maximal temperature (Tmax), minimal temperature (Tmin), and temperature amplitude over the whole therapy.
HRV
Sixty-seven of 83 recorded ECGs were analyzable for comparison of the pre- and post-RM waiting periods. All 83 ECGs could be analyzed for comparison of massage treatment and therapeutic rest. Figure 3 shows an exemplary spectrogram of the HRV analysis during an RM session; as in the case of Figure 1, short-term effects of RM are depicted. The appearance of high power density in the low-frequency band during the massage indicates increased circulation. The narrow red line in the high-frequency band during therapeutic rest indicates strong modulation of heart rate by respiration.
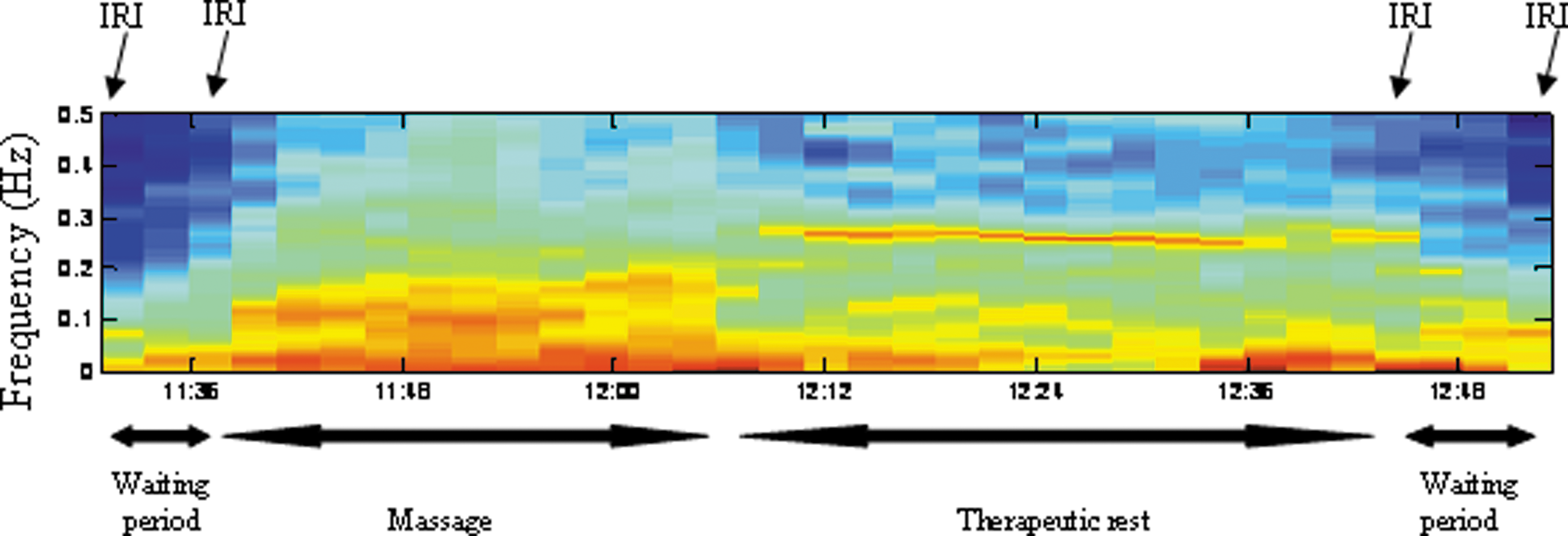
Spectrogram of the frequency analysis of heart rate variability during one typical therapy session. The various steps of the therapy session are shown under the spectrogram, including the waiting periods before and after rhythmical massage. The time points at which infrared imaging (IRI) was done are indicated above the spectrogram. Colors indicate the band intensity at the various frequencies (blue corresponds to none or low, yellow to intermediate, and red to high power density of the corresponding frequency).
24
Color images available online at
The ratio log(low frequency/high frequency) is reduced during therapeutic rest compared with values obtained during massage (Table 2). Likewise, a lower modulation of heart rate in the very-low-frequency band and a stronger modulation in the low-frequency and high-frequency bands were observed during therapeutic rest compared with massage, while the mean heart rate itself remained fairly constant (Table 2). Comparison of variables during the waiting periods in the sitting position before and after RM reveals significant differences (Table 2): Heart rate and high frequency are decreased after RM, while SDNN, low frequency, and log(low frequency/high frequency) are increased. These changes are accompanied by decreases in minimum heart rate and respiration, as well as by reduction of total spectral power, and pulse-respiration quotient (data not shown).
Values obtained during the waiting periods in the sitting position before and after rhythmical massage were compared with each other.
Values obtained during therapeutic rest in the supine position were compared with those obtained during massage. Data are shown as mean±standard deviation.
p<0.05.
p<0.001.
HF, high frequency; HR, heart rate; LF, low frequency; SDNN, standard deviation of normal-to-normal intervals time series; VLF, very low frequency.
A long-term effect was found for SDNN values obtained during therapeutic rest of consecutive RM sessions. In patients with low initial SDNN values, SDNN increased with increasing therapy session number (Fig. 4A), while in patients with high initial values, SDNN decreased (Fig. 4B). The variation of SDNN was therefore inversely proportional to the initial SDNN, exhibiting a hyperbolic behavior with a 0 at approximately 35 milliseconds initial SDNN (Fig. 4C).
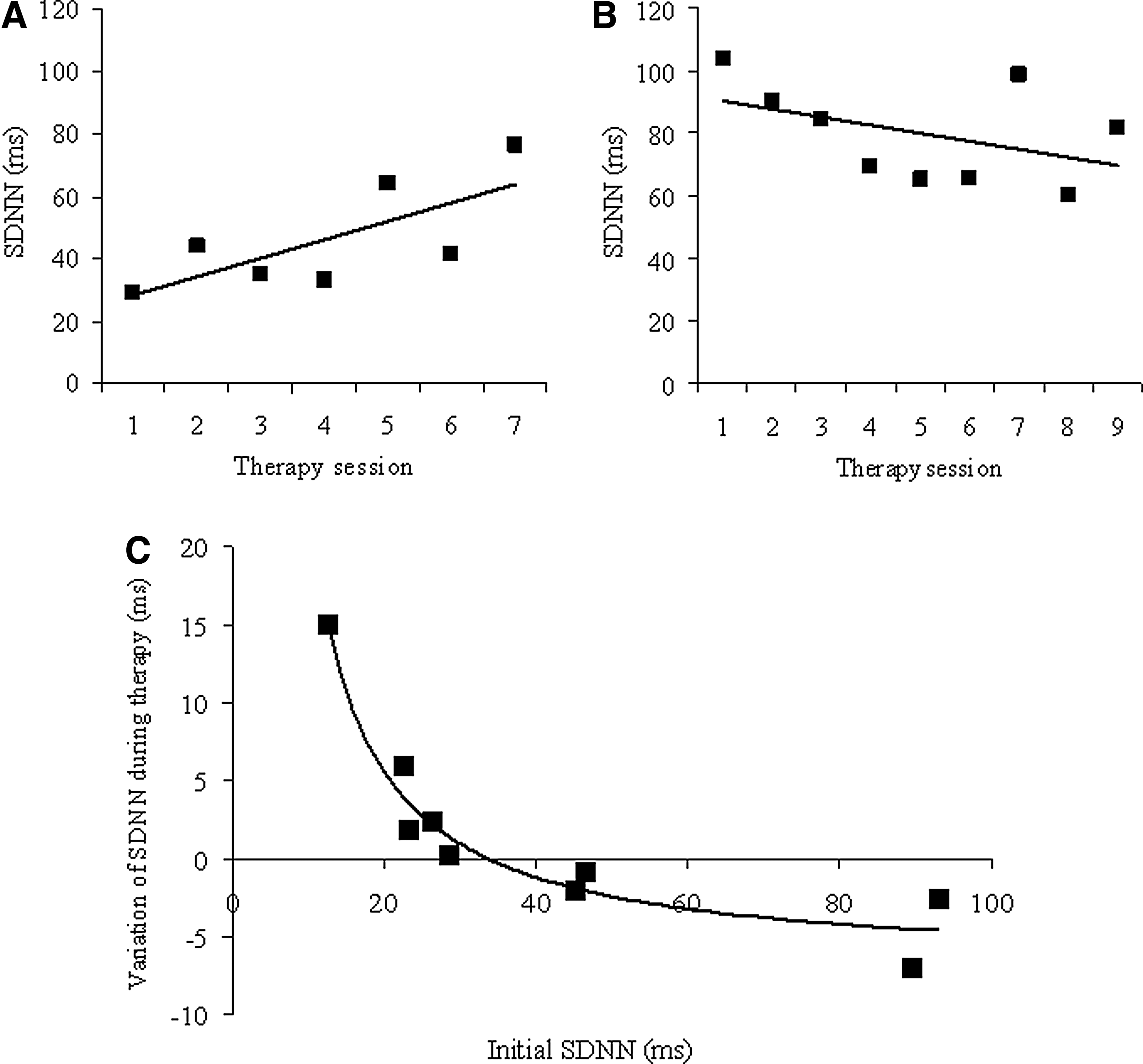
Heart rate variability during therapeutic rest in the course of the therapy sessions.
Discussion
The beneficial effects attributed to massage therapies, such as tissue repair and pain suppression, are thought to be due mainly to improvements in local blood and lymph flow, which are often triggered by alterations in autonomic balance. 21 In the present study, two methods with potential to detect autonomic balance-related alterations were used to study the physiologic effects of RM. IRI allowed the assessment of skin temperature, which is closely related to skin perfusion and is known to be regulated by the interplay between the noradrenergic and the cholinergic components of sympathetic activity. 22 HRV provided an insight into the interaction between the parasympathetic and sympathetic components of the autonomic system. Although most data concern short-term effects of RM, some tendencies were detected with consecutive therapy sessions, which hold therapeutic potential.
Frequency domain analysis indicated short-term effects of RM on HRV that are usually considered associated with a better health state. The comparison of frequency domain measures such as log(low frequency/high frequency) between massage treatment and therapeutic rest revealed the development of deep relaxation states after RM. In contrast, comparisons between pre- and post-RM waiting periods indicated sympathetic stimulation with higher alertness. At the same time, RM led to a decrease in heart and respiratory rates, indicating a more relaxed performance of the organism. Taken together, these effects might indicate an efficient regeneration of patients during RM. An increase of SDNN and low frequency accompanied by a decrease in high frequency has been previously shown to happen during head and neck massage. 23
Concomitant with the stimulation of the sympathetic system, RM led to an immediate increase in skin temperature, as revealed by IRI. Direct stimulation of the cholinergic component of the sympathetic subsystem could explain such a temperature increase. In addition, an indirect warming effect on nonmassaged areas can be postulated because autonomic thermoregulation is not likely to stop immediately at the border of the massaged area, as shown previously. 14 Additional explanations for the increase in temperature upon RM include the frictional component of RM that in part was performed on the dorsal region. Previous work indicates that conduction of heat from the hands of the therapist toward the patient is less likely to have contributed to the changes in skin temperature (compare with Sefton et al. 14 ).
Although momentary warming effects of RM were to be expected, the present work also revealed a surprising, long-term effect of RM on temperature distribution; the difference between temperature extremes after RM became smaller during the course of the treatment sessions. This long-term effect can be interpreted as a more harmonious interplay between the noradrenergic and the cholinergic components of the sympathetic system. Interestingly, RM also had a progressive effect on SDNN during the rest period: always from the initial value toward an intermediate value of SDNN around 35 milliseconds. Such progressive effects might reflect a healing process. Further studies are necessary to elucidate these findings.
A limitation of the study is the small number of patients, which stemmed from an unwillingness to undergo several physiologic measurements; these were in some cases perceived as disturbing the healing potential of RM. In particular, the waiting periods before and after RM were not appreciated and might have led to an underestimation of RM beneficial effects. Further study limitations include the lack of a control group and the fact that the patients could use other therapies and medications. Although this study design has the advantage of reflecting clinical practice, it usually prevents the demonstration of causality between therapy and clinical outcomes. In the present study, physiologic outcomes were compared immediately before and after therapy or during massage and therapeutic rest. Therefore, these comparisons reflect intraindividual changes and are rather robust against interference of the concomitant therapies and medications. With respect to the long-term observed improvements, however, a contribution of these therapies and medications cannot be excluded.
Conclusions
This prospective exploratory cohort study focused on physiologic effects of RM in patients with different diagnoses. Whereas IRI revealed that RM resulted in immediate increases in patients' dorsal temperature, HRV analysis suggested an increased sympathetic activity after RM. These alterations were probably associated with improved alertness or empowering of the patients.
Interestingly, those stimulatory effects occurred after a period of intense relaxation and parasympathetic activity during the therapeutic rest period of RM, which might have contributed to the regenerative capacity of the therapy as a whole. RM might therefore offer a way to set patients' awareness free from situations of discomfort and disorder, thus enabling regeneration.
During the course of the therapy sessions, RM seemed to lead to a progressive improvement of warmth distribution and regulation of HRV. These long-term effects suggest that RM might favorably influence the course of disease but also that some advantages of the therapy might occur only if several sessions are performed.
Footnotes
Acknowledgments
This study was funded by the Foundation Merkur-Rafael (Zürich, Switzerland), Weleda AG (Arlesheim, Switzerland), Software AG (Darmstadt, Germany), and the Swiss Association for Rhythmical Massage (Marbach, Switzerland). The authors gratefully acknowledge the participation of all study patients and thank Professor Rhyner (Paracelsus Hospital, Richterswil, Switzerland) for use of the infrared camera. This study was published in abstract form: Eur J Integ Med. 2012;4S:114, OP-243.
Disclosure Statement
During the study, A.P.S.W., C.W., and D.K. received research grants from the pharmaceutical company Weleda, which produces some of the anthroposophic massage oils and creams used in the study. Otherwise, all authors declare that they have no competing financial interests.