
Abstract

A 22-year-old woman was evaluated with FDG PET/CT for residual Hodgkin disease after eight cycles of chemotherapy and radiation therapy. PET/CT images revealed intense FDG uptake in bilateral inguinal lymph nodes, which were not prominent on the midcycle PET/CT scan (Fig. 1). No other pathologic findings were observed in the rest of the body. The patient had no history of or other findings indicating inflammation or infection. On CT images, soft tissue lesions that had poorly defined margins with mild FDG uptake were detected in the bilateral gluteal adipose tissues. The patient disclosed that she had recently received repeated intramuscular injections of Nerium oleander extracts without her doctor's knowledge. Follow-up PET/CT after 3 months showed significant reduction in size and no uptake in these lymph nodes and no disease recurrence.
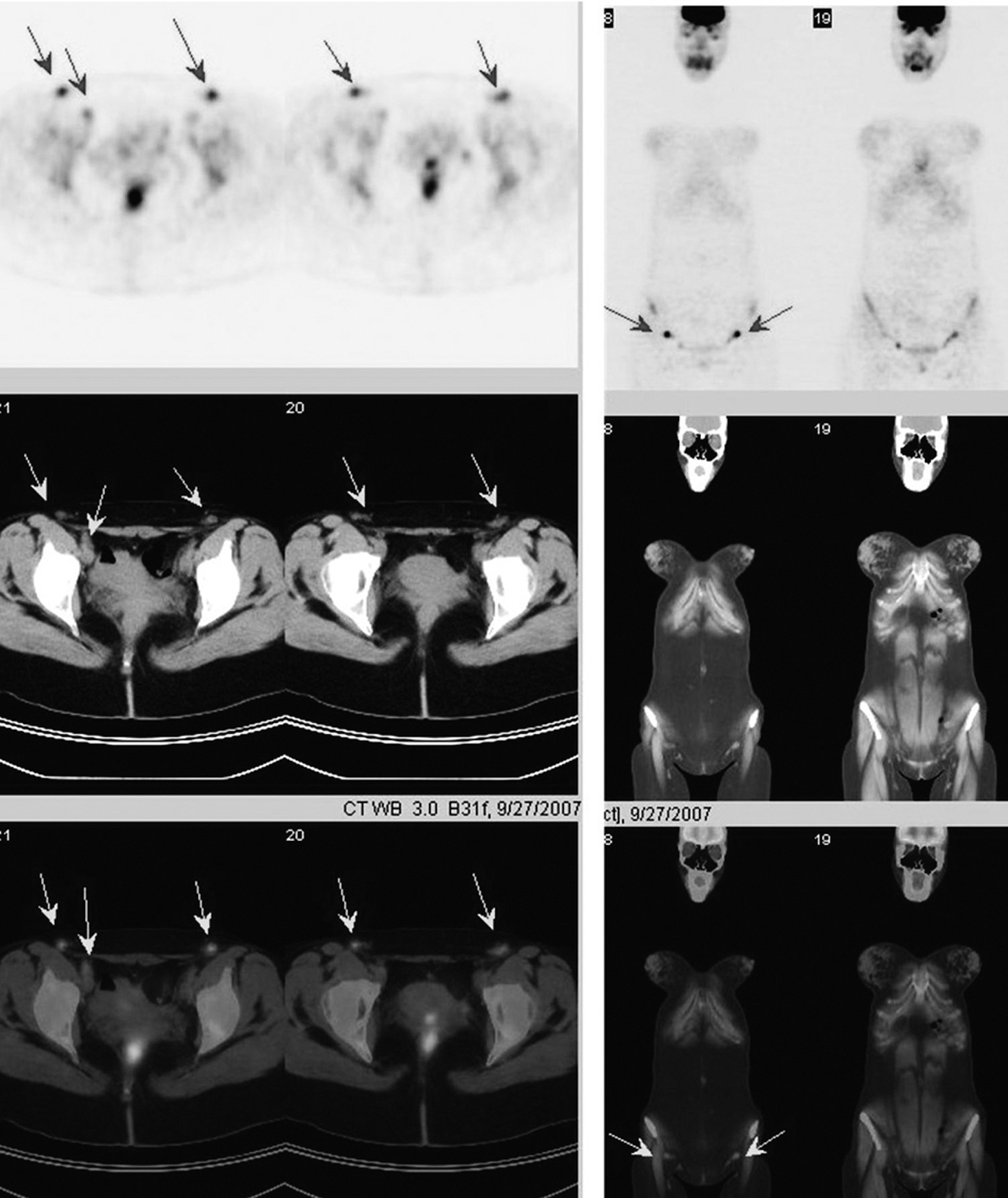
Axial (left) and coronal (right) slices of positron emission tomography (PET), computed tomography (CT), and fused PET/CT images demonstrate bilateral inguinal lymph nodes with intense fluorine-18 fluorodeoxyglucose uptake (maximum standardized uptake value, 7.3.).
The extracts of the plant N. oleander are reported to cause cell death in human cancer cells, and phase II trials have reported on the treatment of patients with advanced malignancies. 1 –3 There is growing interest in evaluating oleander products as antineoplastic agents. 4 Although the indication and use of complementary and alternative medical therapies are not fully approved and their safety and therapeutic effects are not completely understood, such agents are becoming highly popular among oncology patients. These medications may have adverse effects and may interfere with the biodistribution of FDG. In parallel with the increasing frequency of use, clinicians and the imaging community must be aware of potential adverse effects of these administrations. In the current patient, these injections caused an inflammatory response, resulting in intense FDG uptake and enlargement of the lymph nodes.
Many potential pitfalls are known to complicate FDG PET/CT. Influenza and H1N1 vaccines have caused FDG uptake in the regional lymph nodes near the injection site because of inflammatory responses. 5 –7 Nuclear medicine physicians can assist in decision-making by indicating how likely it is that the FDG uptake is a true-positive or a false-positive finding. For this, all patients referred for PET/CT imaging must be fully questioned about all types of medical administrations, as well as patient-based factors such as prior disease location, surgical processes, and other inflammatory diseases. In addition, medical history of all patients scheduled for FDG PET/CT must be evaluated for recent vaccination. False-positive interpretation of PET/CT data can be avoided by the visualization of injection-related FDG uptake in gluteal soft tissues and a detailed patient history.
Footnotes
Disclosure Statement
No competing financial interests exist.