
Abstract
Background:
This study aimed to examine the correlation of heart rate variability (HRV) and meridian electrical conductance among middle-aged women during an 8-week period of auricular acupressure (AA) treatment for weight reduction.
Methods:
Sixty (60) subjects were randomized either to a control group (n=30) or to a treatment group with AA (n=30). Anthropometric parameters, HRV indices, and meridian levels were measured before treatment, at the 5th week, and 1 week after the 8-week treatment period.
Results:
Although no significant changes were observed in body weight (BW) and body–mass index (BMI) from baseline to 1 week after AA treatment, a significant decrease in Waist Circumference (WC) was observed in the acupressure group. In contrast, the subjects' BW, BMI, and WC were significantly increased from baseline to the 9th week in the control group. With adjustment for baseline low frequencies (LF) of HRV, the LF at the 5th and 9th weeks in the acupressure groups was generally lower than that in the control group, with a p-value=0.027 using the mixed linear model. The meridian levels for Spleen, Bladder, and Gallbladder were significantly lower in the group subjected to acupressure than in the control group at the 5th week.
Conclusions:
The results of the present study indicate that AA tends to inactivate the sympathetic nervous activity demonstrated by both HRV and meridian electrical conductance changes. As a result, AA may modulate the autonomic nervous system to exert its physiological effect through the pathway of the meridian system.
Introduction
A
There are 12 meridians in the body: three yin meridians and three yang meridians for the hand and the foot (one side). Each of the 12 regular or principal meridians is associated with a Chinese organ as follows: The three yin meridians of the Hand, running through the anterior of the upper limbs from the chest to the hands, are the Lung (LU) meridian, Heart (HT) meridian, and Pericardium (PC) meridian. The three yang meridians of the Hand, flowing through the posterior of the upper limbs from the hands to the head, are the Large Intestine (LR) meridian, Small Intestine (SI) meridian, and triple energizer (TE) meridian. The three yin meridians of the Foot, running through the medial side of the lower limbs from the feet to the abdomen and chest, are the Spleen (SP) meridian, Kidney (KI) meridian, and Liver (LI) meridian. The three yang meridians of the foot, flowing from the head through the back downward to the feet, are the Stomach (ST) meridian, Bladder (BL) meridian, and Gallbladder (GB) meridian. 3 Ryodoraku is a technique developed by Yoshio Nakatani that measures the electrical conductance at representative points for each meridian. 4 The 24 measured points of the Ryodoraku are located on the 12 main meridians, and therefore, the resultant electrodermal measurement is regarded as the meridian energy based on TCM theories.
Auriculotherapy or auricular treatment involves stimulating points on the ear with sterile acupuncture needles or acupressure with magnetized pellets or seeds. 5,6 When properly used, auricular acupuncture is an effective method for treating a variety of medical conditions including providing a weight-controlling effect in obese patients. 7 –9 Yeh et al. 10 applied magnetic beads to the five pressing points in the ear; they showed significant decreases in waist circumference (WC) and waist-to-hip ratio of overweight and obese women. In a randomized, controlled clinical trial, Lien et al. 11 demonstrated that auricular stimulation with metal beads has a similar effect to that with auricular acupuncture in reducing physical parameters and obesity-related hormone peptides. However, mechanisms underlying auricular stimulation in reducing weight have not been studied previously.
The autonomic nervous system (ANS) directs involuntary physiologic processes such as digestion, blood pressure, hormonal regulation, energy metabolism, and heart rate. 12 Heart rate variability (HRV) is widely considered a standard method for assessing ANS function. 13 Dysfunction in ANS has been suggested as an important mediator in the development of obesity and obesity-associated diseases. 14 –16 However, only limited evidence available in the literature touches on the ANS activity in the development of weight gain or weight loss. 17 This investigation was undertaken to explore the relation between meridian electrical conductance and ANS under the treatment of auricular acupressure (AA) for weight reduction.
Materials and Methods
Subjects
This was a prospective study conducted from November 2009 to June 2010. All study procedures were approved by the Institutional Review Board at the Taipei City Hospital (TCHIRB-981009-E). Volunteers were recruited from a weight-reduction program for middle-aged women. No criteria for body–mass index (BMI) were included. Initial evaluation included measurements of body composition, namely, body weight (BW), height, and WC. BW was measured to the nearest 0.1 kg using an electronic scale. WC was measured at the level midway between the lateral lower rib margin and the iliac crest. Blood pressure (BP) and resting heart rate (HR) were recorded following a 30-minute resting period while subjects were in a sitting position. BP and HR were measured using an adapted-size BP cuff and an electronic sphygmomanometer. A total of 60 women aged between 39 and 55 years were enrolled into the study. Individuals with the following conditions were excluded: (1) prior cancer and/or tumor histories; (2) prior history of hypertension; (3) cardiac arrhythmia or an implanted cardiac pacemaker; and (4) current use of drugs or TCM that might contradict or interfere with measured outcomes. No concomitant interventions for weight control were performed in both groups.
Group and intervention
After the completion of baseline evaluation, participants were assigned by register code entry on the computer to either the intervention or the control group. The assessors (Fu-Chun Chen and Hsing-Yi Hu) were not blinded to the assignment of participants. The researcher (Chi-Feng Liu and Li-Wei Chien), who was not involved in the intervention procedure, collected and analyzed the data. Sixty (60) women were randomized into the treatment (n=30) and control groups (n=30). Based on the theory of TCM, we chose two auricular acupoints—Liver (CO12) and Spleen (CO13). AA was performed by using seeds named Semen vaccariae, a small object approximately 2 mm in size. Acupoint acupressure protocols using botanical plant seeds have been described in previous investigations. 18,19 Applied by a trained therapist onto the two auricular acupoints selected, the seeds were kept in place by a piece of opaque adhesive patch. Application of acupressure included massaging 20 times on each point at one session. All subjects were asked to apply the AA three sessions per day, beginning 30 minutes after each meal, for 5 consecutive days. After a 2-day rest period, the AA was applied on the other ear in the following week. Treatment was given over a period of 8 weeks. Hence, each ear underwent four treatments alternatively for a total of eight treatments for each subject. Subjects in the control group were not given AA during the study period. At the end of the study, they were offered the same intervention procedure if they wanted it.
HRV analysis
HRV was recorded with subjects in the sitting position after a 5-minute rest and in a quiet room at room temperature using the Heart Rate Variability Analyzer (SA-3000P, Medicore Co. Ltd., Seoul, Korea). The HRV sensor was clipped on the index finger (second finger) of the left hand. The subjects were asked to keep silent and stay inactive during the measurement. The subjects were earlier told to avoid strenuous physical activity, as well as alcohol and coffee intake within 24 hours before the measurement. HRV analysis was performed according to the guidelines of the Task Force of the European Society of Cardiology. 12 The following time-domain parameters were evaluated: SDNN (ms), that is, the standard deviation of the normal-to-normal (NN) intervals. SDNN reflected overall HRV. The frequency domains of HRV components were obtained at low (LF 0.04–0.15 Hz) and high (HF 0.15–0.4 Hz) frequencies, in absolute units (ms2). The LF domain reflects both the sympathetic and the parasympathetic nervous systems, and the HF domain primarily reflects vagal cardiac control; the LF/HF ratio was calculated to determine the sympathovagal balance.
Meridian measurements
The meridian level was examined by MEAD Me-Pro (Hanja International, Taoyuan, Taiwan), which yielded electrical conductance measurements of the 24 meridians (12 for the left and 12 for the right) and is similar to equipment used in previous studies. 20 –22 The design of MEAD is based on the Ryodoraku theory. 4 The measurements were started with very low current, which was gradually increased to a maximum value of 200 μA. Readings of the electrical conductivities of the meridians were directly entered into a computerized system. The conductance values were calculated with voltage supplied by the device and currents measured in meridians and were expressed as the scale between 0 (zero conductivity) and 100 (maximum conductivity). The average conductance value of left and right in 12 meridians of each subject was calculated.
Data analysis
Due to the small sample size, data were expressed by median with interquartile range (the range between 25th and 75th percentiles) and compared by the nonparametric Mann–Whitney U test between the two treatment groups. The changes from baseline to the 9th week within group in BW, BMI, WC, BP, and HRT were tested by the Wilcoxon signed-rank test. Other variables with repeated measurements were analyzed using the mixed linear model. Statistical hypothesis tests were set with a significance level of 0.05. Statistical analyses were performed using the software SPSS 15.0 (SPSS, Chicago, IL).
Results
Demographic and anthropometric parameters
A total of 54 subjects completed this study (Fig. 1). Three subjects in the treatment group and three subjects in the control group dropped out due to missed treatment sessions (n=4) and missed measurements (n=1). The baseline characteristics are summarized in Table 1. The baseline characteristics (age, height, BW, BMI, WC, HR, and BP) for the two groups were comparable (Table 1). In the control group, subjects' BW, BMI, and WC were significantly increased from baseline to the 9th week. BMI in the control group was increased from a median of 22.1 kg/m2 at baseline to a median of 22.6 kg/m2 at the 9th week (p=0.001). WC was increased from the medians of 76.0 cm at baseline to 77.0 cm at the 9th week (p=0.047). In the acupressure group, no significant changes were observed in BW and BMI from baseline to the 9th week. A significant decrease in WC was observed, although the median waistline at baseline and the 8th week were both 75.0 cm; at the 9th week a higher full range of WC was presented as compared to baseline (from 66.0 to 88.0 cm at baseline and 63.0 to 87.5 cm at the 9th week; p=0.003; Table 1).
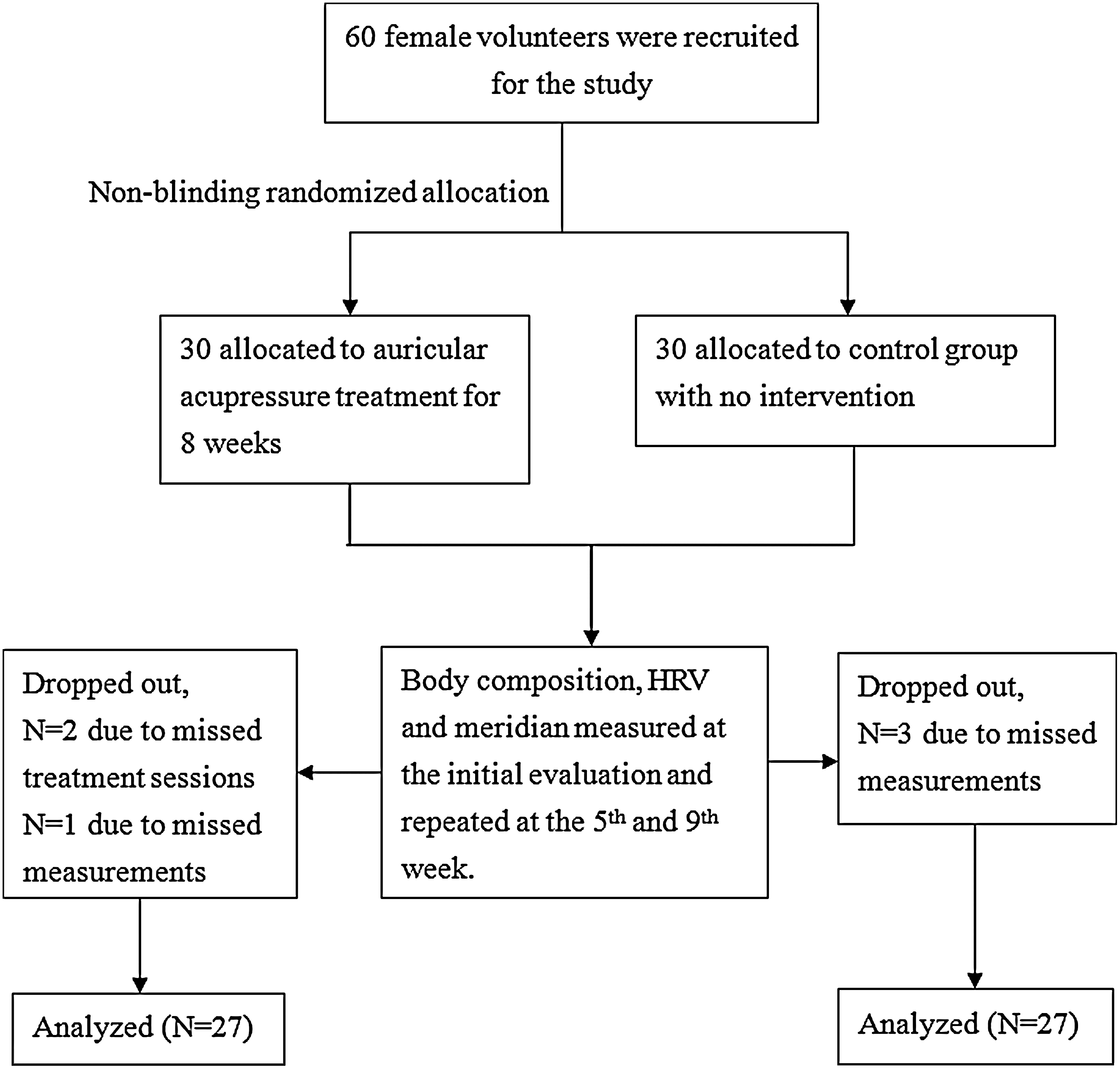
Flowchart of the distribution of the cohort study. HRV, heart rate variability.
Data are expressed as median and interquartile range.
Indicates a significant difference from baseline to the 9th week within group.
BMI, body–mass index; WC, waist circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; HR, heart rate.
HRV
Resting HR at baseline and 9 weeks after allocation showed no significant difference between the treatment and control groups (Table 1). The baseline HF and SDNN in the acupressure group were significantly lower than that in the control group (median at baseline: 123.65 versus 277.74, p=0.028; 25.69 versus 33.99, p=0.030) (Fig. 2B and D). With adjustment for baseline LF, the LF at the 5th and 9th weeks in the acupressure groups was generally lower than that in the control group, with a p value=0.027 by the mixed linear model (Fig. 2A). No significant differences were observed in the LF/HF ratio and total power (TP) both in the mixed linear model and in the group comparisons (Fig. 2C and E). No significant time trend effect in LF, HF, LF/HF ratio, TP, and SDN was also observed in the mixed linear models (Fig. 2A–E).
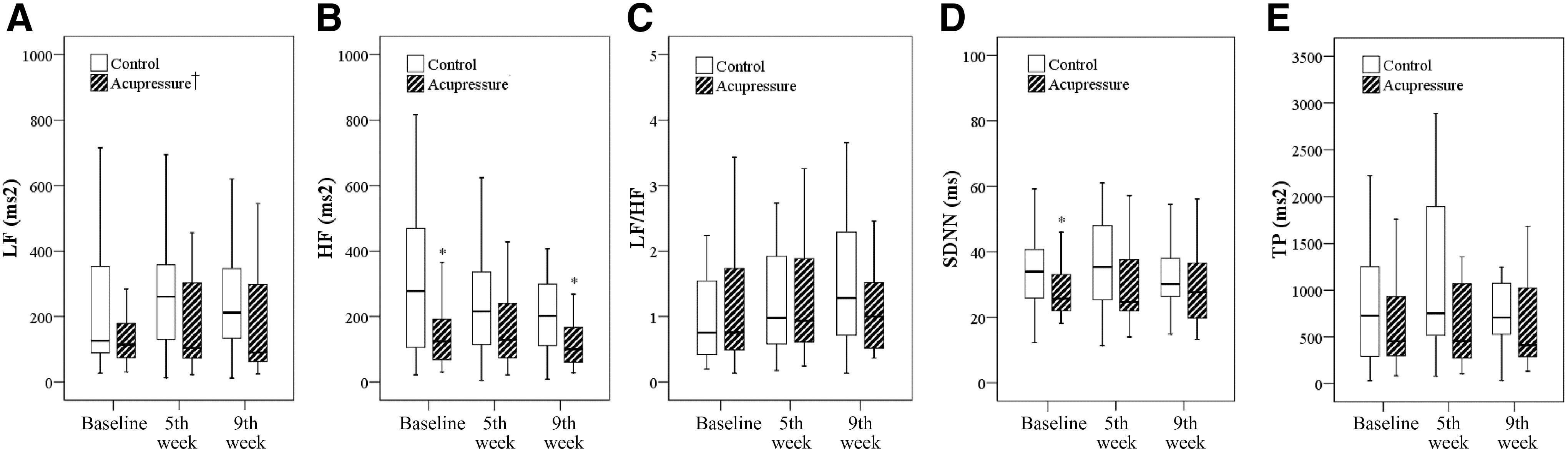
Effect of acupressure on low frequencies (LF)
Meridians
No significant time effect on the 12 meridian levels was observed (Fig. 3). With adjustment for the baseline measurement, significant group effects were observed on the meridian levels of BL (p=0.029). No significant differences between groups in the 12 meridian levels were observed at baseline and the 9th week. However, at the 5th week, the meridian levels for SP, BL, and GB were significantly lower in the group of acupressure than in the control group (median: 46.5 versus 57.25 with p value=0.034 for SP, 41.0 versus 56.25 with p value=0.006 for BL, 34.0 versus 44.75 with p value=0.015 for GB) (Fig. 2). The meridian for ST was also lower in the acupressure group than in the control group at the 5th week, although it did not reach statistical significance (median: 35.0 versus 47.5 with p value=0.055) (Fig. 3).

Balance of the 12 meridian energies. *Indicates a significant difference was observed at the specified time point by Mann–Whitney U test. †Indicates a significant group effect was observed in Bladder (BL) meridian with adjustment for the measurement at baseline in the mixed linear model.
Discussion
We observed that AA reduces weight gain and modulates the sympathovagal balance in middle-aged women. Although BW and BMI were not reduced significantly in the acupressure group after an 8-week treatment, WC decreased significantly after AA. Furthermore, we demonstrated that modulation of ANS presented changes of both HRV and electrical conductance in certain meridians after auricular stimulation. Reduced LF of HRV was observed from the 5th week of treatment until 1 week after the 8-week treatment period in the AA group. Transient changes in the HF and SDNN were also observed during the treatment period. Furthermore, acupressure treatments induced a lower electrical conductance for SP, GB, and BL meridians than those in the control group during the treatment period.
Previous investigations have shown that auricular acupuncture or acupressure stimulation impacts the ANS from both animal and human studies. 23 –25 By stimulating the auricular “heart” point in anesthetized rats, Gao et al. 23,24 demonstrated that auricular acupuncture induces cardiovascular inhibition via the baroreceptor reflex. In agreement with these results, they also showed a significant decrease in HR and a significant increase in total HRV by applying manual AA in healthy volunteers. 25 In a three-armed randomized trial involving 14 healthy men by La Marca et al., 26 acupuncture was conducted on the concha of the ear to evaluate its capacity to increase vagal activity. Electroacupuncture was found to have a positive effect on stimulating the vagal activity compared with placebo, manual acupuncture, and a control condition without intervention. 26 In contrast to these findings, we demonstrated a suppression of sympathetic nervous system (SNS) activity with a transient stimulation effect on the parasympathetic nervous system (PNS) activity after AA. Our results are in accordance with a study by Uchida et al. recording the cardiac sympathetic efferent nerve activity in anesthetized rats. 27 They reported that reductions in HR in response to acupuncture-like stimulation, but not increased parasympathetic vagal outflow, are the result of reduced sympathetic outflow to the heart. 27 Inconsistent results on the effects of acupuncture or acupuncture-like treatment on the ANS in the literatures might be explained by the various approaches of the different studies. 26 Only short-term effects of HR changes within seconds to minutes of acupuncture treatment were observed in previous reports. 25,26 The current investigation, however, involved long-term treatment and follow-up. A lower baseline HF and SDNN level observed in the acupressure group was an unexpected finding. It may be related to the lack of diet and exercise controls in our selection of subjects for investigation. In accordance with findings of SNS suppression during the treatment period of AA, we detected lower electrical conductance levels in certain meridian pathways.
Electrical conductance in the skin is known to be predominantly controlled by the SNS, whereas the cardiac responses such as HRV are controlled by both the SNS and PNS. 28 We found an instant and prolonged decrease of LF accompanied by decreases in SP, GB, BL, and ST meridian conductance during an 8-week treatment period. It might suggest that a sustained effect of suppression of SNS is accompanied by a transient stimulation of PNS activity after auricular stimulation. In a study involving 40 patients under laparoscopic cholecystectomy against 55 healthy controls, Schmidt et al. 20 showed decreased SNS activity during surgery as evidenced by Ryodoraku meridian examination. This study concluded that Ryodoraku is a useful tool for evaluating SNS activity. 20 The Ryodoraku mechanism can be explained by the viscera–skin sympathetic nerve reflex. 20 –22 The impulses from the viscera radiate to the spinal cord. The reflex zones are then reflected onto the skin surface via the efferent sympathetic nerves and appear as a longitudinal connecting system following the classical Chinese meridian pathways. 4,29 Previous studies on meridian suggested that HT, GB, SP, and SI related to the intestine than the other meridians, whereas LI, LR, Sanjiao meridian of the hand shaoyang (SJ), ST, SP, and SI are more closely associated with the stomach than the other meridians under normal physiological conditions. 29 There are circulating pathways of five meridians (LR, SJ, ST, SP, and SI) that directly pass the stomach while four meridians (HT, GB, SP, and SI) directly pass the intestine. 29 The lower energy levels at ST, SP, and GB observed in the AA group of subjects in the current study suggest that treatment at auricular acupoints may have an impact on gastrointestinal function. A characteristic pattern of bradycardia with gastric contraction could be evoked by stimulation of different areas of the auricle in anesthetized rats. 23 In humans, the average coefficient of the electrical conductance in 24 meridians was significantly decreased after weight reduction in a study with oral medication for the treatment of obesity. 30 We speculate that AA might suppress gastrointestinal motility in exerting its weight-control effect. However, whether it is a phenomenon of regulation of ANS activity of the gastrointestinal system or through reduction of appetite from suppression of the satiety center in the central nervous system 31,32 could not be answered from the data presented in the current investigation. Nonetheless, our results provide information regarding physiological effects of AA treatment.
There are several limitations in the current study. First, no sham intervention group was included to control for possible placebo effects. Second, we did not monitor HRV and meridian electrical conductance simultaneously. Whether the modulation of HRV is directly related to the changes in the meridian levels after AA stimulation, or vice versa, could not be determined from the present study. Third, the reliability and validity of equipment in measuring the meridian cannot be determined from the information provided by the literature. 33 Variable contact area, pressure, skin hydration, and, most importantly, the presence of sweat ducts all may confound the current electrodermal devices to one degree or another. 33 In addition, we did not perform correlation analyses for each subject separately. Because HRV and meridian values are highly variable between individuals, further investigations will be required to validate whether these parameters could serve as a reliable and valid approach. Finally, this study involved only middle-aged women with a small sample size and cannot be generalized to the male population as a whole.
Conclusions
The results of present study indicate that AA reduces the weight gain, and modulates the sympathovagal balance in middle-aged women. AA tends to inactivate the SNS demonstrated by HRV and meridian electrical conductance changes. As a result, AA may modulate ANS to exert its physiological effect through the pathway of the meridian system. A large-scale randomized trial would be required to further elucidate the effects of AA on weight reduction in correlation with regulation of the ANS.
Footnotes
Author Disclosure Statement
No competing financial interests exist.