
Abstract
Introduction:
Hemiplegia and the Ayurvedic description of ardhanga disease presents with comparable clinical features. This pilot trial compared two traditional procedure-based treatments: Navarakizhi, a massage of cooked navara rice in a medicated hot bolus, and pinda sweda, a similar massage made of a different type of rice. This article also describes the steps of a double-blind trial in Ayurveda, which was hitherto considered difficult to perform.
Methods:
Eighteen (18) patients suffering from hemiplegia with disease duration of 6 months to 2 years received treatment with navarakizhi or pinda sweda for 7 days. Both groups received the same Ayurvedic oral medications for 14 days. All steps of randomization and blinding of procedure-based therapy in Ayurveda are described. The physiotherapist evaluated muscle tone, muscle strength, tendon reflexes, range of movement, and balance of functional abilities at baseline, 7 days, and 14 days after starting therapy. Both patient and the assessing physiotherapist were blinded.
Results:
Intraquartile range values showed better range in patients who received navarakizhi than those who received pinda sweda.
Discussion:
A larger trial is needed to confirm the superiority of navarakizhi over the rice varieties in treating hemiplegia. This study demonstrates that double-blind randomized clinical trials are possible in Ayurvedic settings, ending the long-debated controversy in trial methodology involving procedure-based traditional medicines.
Introduction
I
Currently, long-term physiotherapy is recommended for management of patients with hemiplegia. However, Ayurveda emphasizes the drugs and procedures that alleviate vitiated manifestation of vata properties are the common line of treatment for imbalance of vata. 2 Clinically observed features of vata 3 are xeroses on inspection (ruksha), light (laghu), cold (sheeta), xerosis on palpation (khara), minuteness (sookshma), and mobility (cala). In ardhangaroga, there is no affliction of primary life force other than vata 4 ; the treatment should, therefore, stabilize the primary life force of motion, in this case to achieve vata alleviation. 5 Pinda sweda (pinda is bolus and sweda is to sweat) prepared using nourishing (called brumhana 6 ) drugs is beneficial. 7 The drugs and therapies that nourish the body achieve vata alleviation 8 due to their action opposite to vata properties. They include heat, sweat, etc., which help to overcome cold and xerosis, respectively. The rice exudates and the massage provide nourishment and muscle stimulation, respectively. Navarakizhi, a form of pinda sweda, provides a nourishing effect to persons suffering from ardhangaroga (hemiplegia). 9 In this procedure, navara rice is grown for 60 days, cooked, and tied in cloth to form a bolus (pinda). The pinda is then used for a full-body hot massage. Classical literature in Ayurveda describes navara rice as superior to other varieties of rice due to its oiliness (snigdha), sweet (madhura), stable (sthira) properties and capacity to normalize three primary life forces. 10
This study is the first trial that compared two varieties of pinda sweda using two different types of rice. The objective was to determine whether navara rice could act as brumhana, alleviating vata and improving muscle tone and action with the aim of providing evidence-based treatment in Ayurveda.
Materials and Methods
Two rice varieties, Navara rice (golden yellow glumed navara variety) 11 and Palakkadanmatta rice were cultivated for the purpose of this trial at Community Agrobiodiversity Centre, M.S. Swaminathan Research Foundation, Wayanad, Kerala. Ethical approval was obtained from the institutional ethics committee of Community Agro Biodiversity Centre.
As a pilot study, the sample size determined to be was 18. These patients were recruited from the referrals made to the Institute of Applied Dermatology from peripheral clinics during the study period (from September 2009 to December 2010).
Patients were randomized into two treatment groups, using the method described below. The following protocol was then applied to all patients: According to the randomized groups, patients were treated with either Navara rice (golden yellow glumed navara variety) 11 (Group A) or Palakkadanmatta rice (Group B) (Fig. 1).
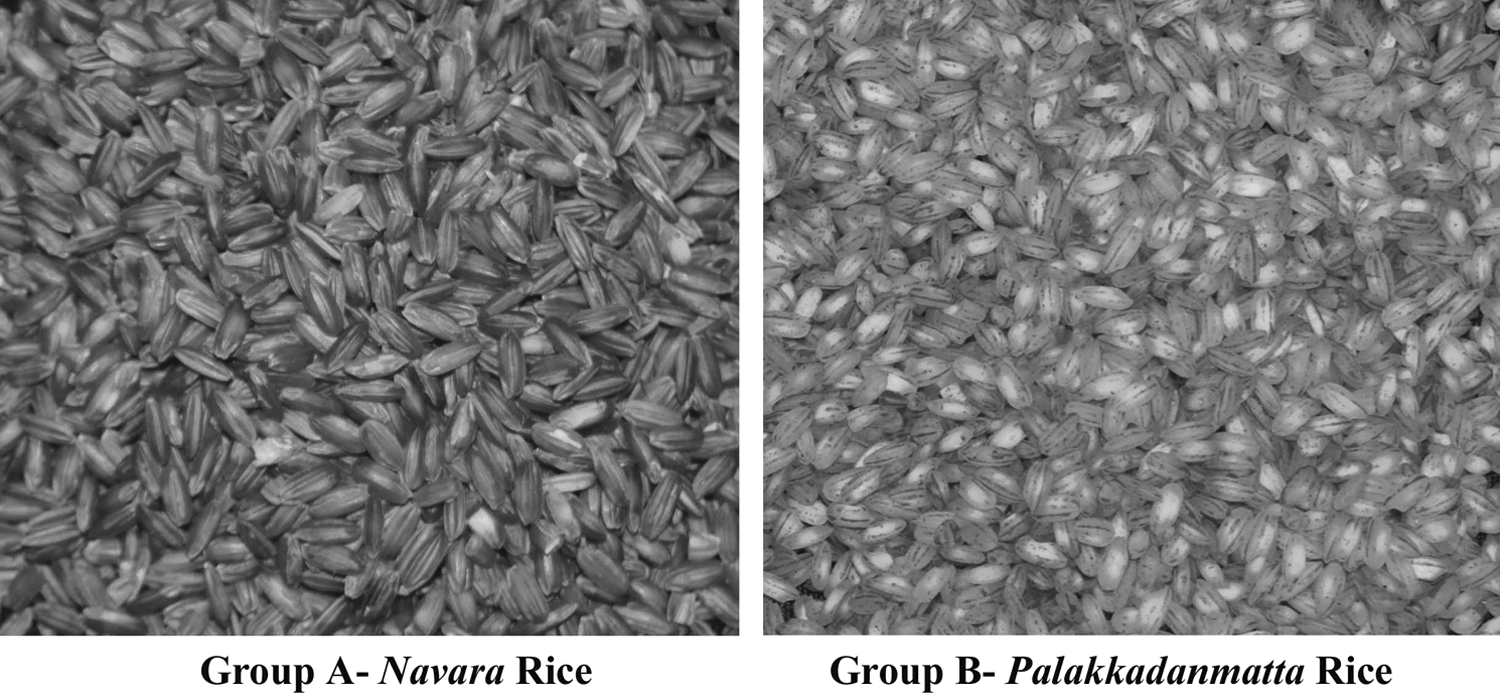
Navara rice and Palakkadanmatta rice used for comparison in the trial. Both types of rice have the same color and require the same amount of time to cook.
Treatment protocol
1. Counseling to explain the disease physiology, treatment, and possible outcomes. This was followed by obtaining written consent.
2. Baseline Ayurvedic and physical evaluation was done by a consultant Ayurvedic doctor and physiotherapist.
3. Laboratory investigations were done, as follows: full blood count, hemoglobin percentage, postprandial blood glucose, liver function test, renal function test, urine examination, and electrocardiogram.
4. Pinda sweda for 7 days using navara rice or palakkadanmatta rice.
5. Physiotherapist re-evaluated the patient, muscle strength was calculated using the Medical Research Council (MRC) score, and laboratory investigations were repeated on the seventh and 14th days.
Ayurvedic oral medications were given for during the full course, 14 days, starting on the first day of pinda sweda.
Randomization Methods
Blinding the treatment
Eighteen (18) identical yellow bags were selected to pack medicines and rice. Each yellow bag contained seven plastic, airtight 100-mL bottles of Ksheerabalathaila, 12 two bottles of Dhanadanayanadi kashayam, 13 56 tablets of ekangaveera rasa, 14 and a cotton bag filled with 3500 g of either navara rice or palakkadanmatta rice. The concealment was done in the presence of a statistician and a pharmacist, keeping all other team members blinded (Fig. 2). We were unable to blind the S. cordifolia plant because of the possible changes in product weight and consistency during storage. Both groups received 500-g portions (total 3500 g) of S. cordifolia in seven packs within a large plastic bag. In addition, both groups were provided daily with 2 L of milk to prepare the bolus mixture, for a 7-day period.

Concealed and numbered medicinal bags. This bag was given to patients according to the number assigned to the patient by the pharmacist. Only the pharmacist and statistician were aware of its contents.
Patient randomization
A random sequence was generated using the random-number table method. The table was read in top-to-bottom direction and only integers 1–18 were randomly selected. If a number was selected for a second time, it was skipped and the next number was considered. This procedure of sequence generation was done by a statistician. The sequence-generated table was kept in a sealed envelope. The numbers 1–18 were written on the yellow bags according to the group to which they belonged. Bags were given to patients in sequence based on their recruitment into the trial. For instance, the first patient who was selected for participation in the trial was given the bag numbered “1.” In this way, allocation of patients to treatment groups was predetermined in order to avoid allocation bias. Sampling method was simple random sampling without replacement.
Blinding the evaluator
This is a double-blind, randomized study, as patients and outcome-evaluating physiotherapists were unaware of the type of rice used for their treatment. The paramedical workers in the treatment team, Ayurvedic doctor supervising the treatment procedures, and the statistician who enrolled the patients into different groups were not blinded. The physiotherapist evaluated muscle strength using the MRC score, 15 muscle tone using the modified Ashworth scale 16 and deep tendon reflexes. Deep tendon reflexes were scored according to the response; “no response” scored 0, “hypoactive responses” as 1, “hyperactive responses” as 2, and “normal responses” as 3. The manual muscle strength was further assessed through manual muscle testing (MMT). 17 Finally, the functional ability was tested through the Berg balance scale. 18
Patient Selection
Patients showing signs and symptoms of ardhangaroga 1 as described in Caraka samhita were selected for the study. The signs and symptoms according to the classical Ayurveda text and their comparable allopathic terms are displayed in Table 1. A vikruthi table of hemiplegia was developed by Ayurvedic and allopathic doctors from observing the clinical features of the 18 patients. 19
All patients did not exhibit full range of clinical features of Ardhangaroga.
The study was not limited to patients with a particular prakriti (constitution of the body). 20 The patients below 18 years and above 80 years of age, pregnant and lactating women, patients with joint deformities and excessive muscle wasting were excluded from the study. The hemiplegic patients in comatose state, due to cerebrovascular accident and muscle fasciculation within the last year, or acute episodes (less than 1 week) or those needing allopathic care were also excluded from the study. 21
Pre-Pinda Sweda Preparation
Two liters of S. cordifolia decoction was obtained by boiling 500 g of coarsely powdered S. cordifolia dried whole plant, in 8 L of water until it reduced to 2 L. Four hundred grams of rice used for pinda sweda (either navara rice or palakkadanmatta rice) were boiled in 800 mL of water for 40 minutes, to prepare steamed rice. The steamed rice was mixed with 1 L of S. cordifolia decoction and 1 L of cow's milk and boiled over a low flame with constant stirring until it achieved a semisolid state. This mixture was made into a bolus by dividing them into six parts and tied over a no. 10 cotton cloth. This tight, firm, and round bolus was known as pinda. Six such bolus bags were prepared.
One liter of S. cordifolia decoction and 1 L of cow's milk are mixed in a wide-mouthed vessel and kept over a low flame for boil. This was used as heating solution for the bolus. When it started boiling, four bolus bags were dipped in this mixture. Two bolus bags were used as supplement, when other bags were torn or empty.
With the patient sitting, the masseur begins the massage (abhyanga) on the patient's head with circular movements of the palms for 2 minutes. The patient then lies in the supine position, and the massage is continued by two masseurs simultaneously applying ksheerabala oil toward the lower extremities. Specifically, the massage started from the right or left abdominal region, moved through the flanks to the shoulder region toward the palmar region, for a total of 10 minutes. This was then repeated with the patient in the prone position. At the end of this abhyanga procedure, the patient returned to the supine position to begin pinda sweda.
Pinda sweda
The hot bolus bags (pinda) were boiled in a mixture of bala solution and cow's milk. Initially the bolus was lightly patted over the body to test the tolerability of the patient and prevent scalding. The masseurs standing on both sides of the patient gently rubbed the pinda in to-and-fro movements, starting from the lower limbs and extending to the abdominal region, thorax, and upper limbs (Fig. 3).

The hot bolus of rice was gently rubbed on the body starting from the lower limbs. The bolus was exchanged for a new hot bolus when the masseur felt that the bolus was cooling down. It was squeezed periodically during the procedure to gently release medicinal contents.
The masseuses squeezed the pinda during the massage to push its contents out and apply the medicinal paste all over the body. As the pinda lost heat, it was reheated in the boiling mixture of S. cordifolia solution and cow's milk, while another boiled pinda was used for massage. This procedure was done for 45 minutes, with the patient lying supine and prone. Immediately after the pinda sweda, the applied medicinal paste was removed by scraping with coconut leaves, with the patient sitting. The patient rested for 20 minutes and bathed in warm water without using soap.
This procedure was repeated daily for 7 days. During these days, patients were advised to avoid direct sunlight, breeze, physical exertion, and mental worries. Patients were enrolled in inpatient care to control these factors.
Patients were advised on eating nourishing vegetarian food such as milk, green gram, and were advised to avoid tobacco chewing, smoking, and alcohol intake.
Statistical Measures Used for the Analysis
Nonparametric tests were used to find the results in ordinal data. All parameters were analyzed based on median and intraquartile range (IQR). All the data were analyzed using SPSS 16 (SPSS Inc., Chicago, IL).
Results
In total 18 patients were recruited (13 male, 5 female) with a mean age 65 years (age range 48–75). Twelve patients were not working due to chronic illness. The families of nine patients were dependent on the income generated by these patients. Thirteen patients had a history of alcoholism and tobacco use.
Muscle strength
Figure 4 shows the changes in MRC grades for group A and group B. After 14 days of treatment, group A and B had biceps muscle strengths scores of a median of 0 with IQR of 0–2 and 0–0.5, respectively. For triceps muscle strength, group A had a median of 1 and group B had a median of 0 with an IQR of 0–2 and 0–0.5, respectively. Quadriceps muscle strength score had a median of 1.5 in group A and a median of 0 in group B with an IQR of 0–2.25 and 0–1, respectively. Group A and Group B had a median score of 0 for hamstring muscle strength with an IQR of 0–1.5 in group A and 0–0.75 in group B. Although p-values were not significant, group A showed better IQR in all four muscles, compared to group B, after 14 days of treatment.

The assessment intraquartile range and median of muscle strength after 7 and 14 days of treatment. Group A received Navarakizhi and Group B received Palakkadanmatta rice. The numbered dots indicate extreme values.
Muscle tone
Figure 5 shows the changes in MRC grades for group A and group B. Muscle tone was calculated by using the modified Ashworth scale. Group A had a median score of −1 and group B had a median score of 0 for biceps muscle tone after 14 days of treatment. The IQR of both groups were −1.75–0 and −0.5–0.5, respectively. For hamstring muscles, group A's median was −1 and group B's median was 0 with an IQR of −1.75–0 in group A and −0.5–1 in group B.
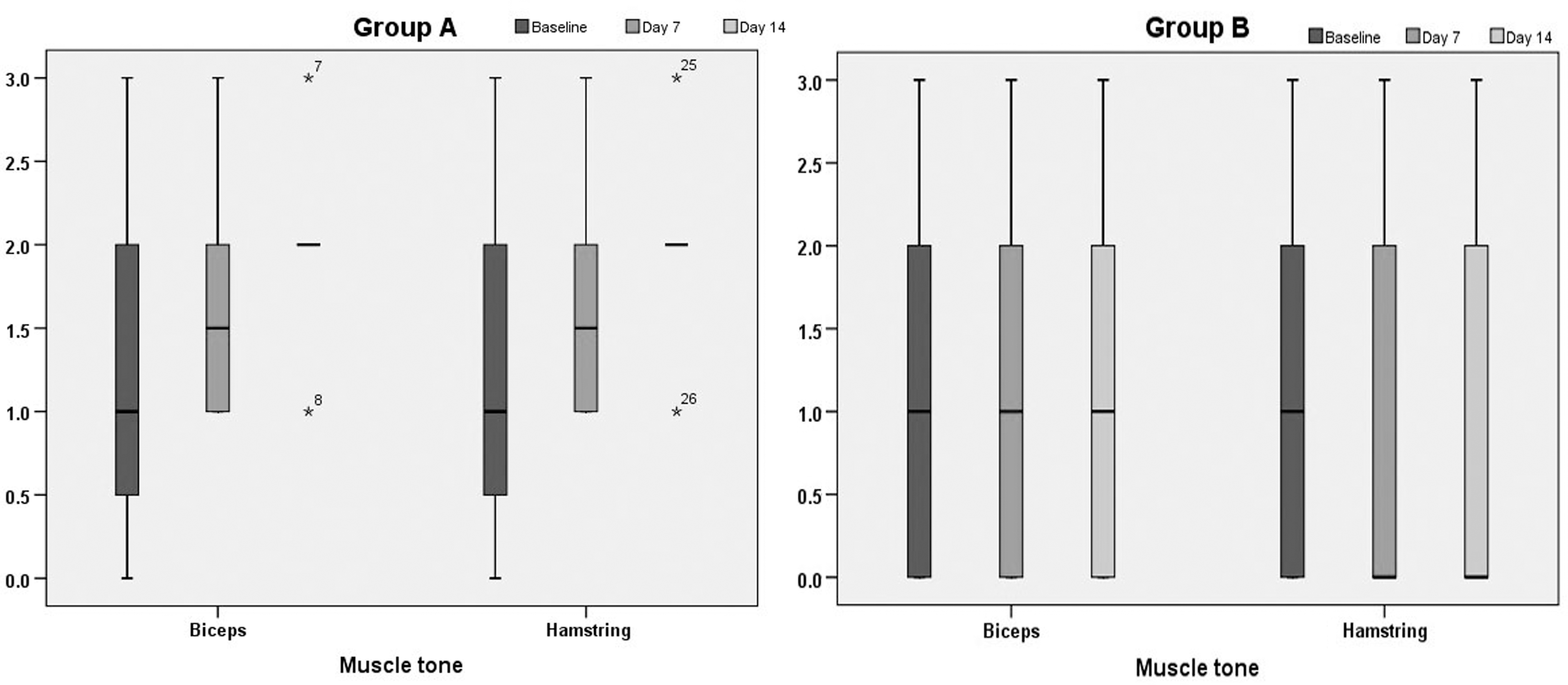
The assessment of intraquartile range and median of muscle tone in two groups after 7 and 14 days of treatment. Asterisks indicate outlier values.
Deep tendon reflexes
For deep tendon reflexes, group B showed a median score of 0 in all muscle tendons, whereas group A had a median score of 0.5, 0, 1, and 0 with an IQR of 0–2.5, 0–1, 0–2.75, and 0–0.75 in biceps, triceps, quadriceps, and Achilles tendon after 14 days of treatment (Fig. 6).
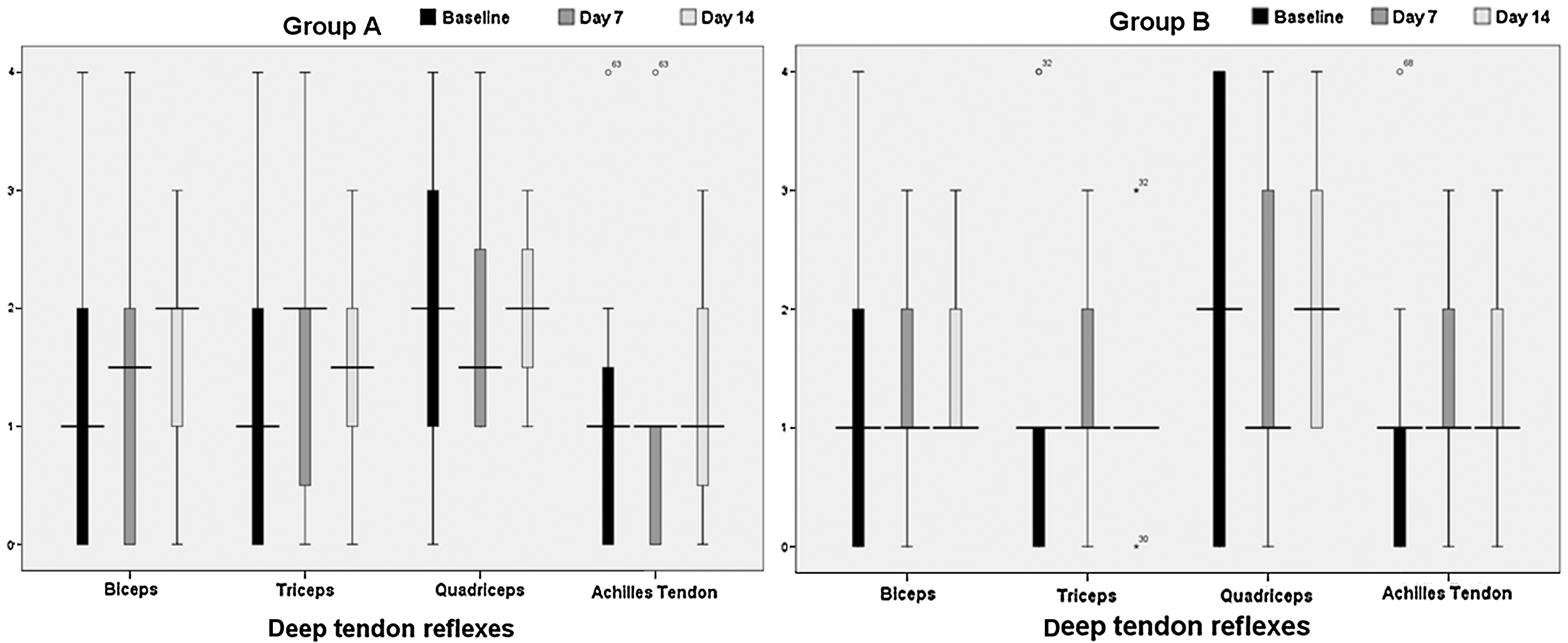
The assessment of intraquartile range and median of deep tendon reflexes in two groups after 7 and 14 days of treatment. The numbered dots indicate extreme values.
Manual power assessment
Manual power of both upper and lower limbs is shown in Table 2.
Group A: Navarakizhi; Group B: Palakkadanmatta rice; IQR, interquartile range.
Functional ability
The difference in functional ability after 14 days of treatment was 9.5 in group A and 7.3 in group B, which is significant (p-value is 0.017 in group A and 0.027 in group B) in the 5% level. However, the difference between the two groups was insignificant (p=0.588) (Table 3).
Group A: Navarakizhi; Group B: Palakkadanmatta rice. Score ranges from 0 to 56; the higher value indicates better functional status, significant if p<0.05.
No adverse events were reported from the 18 patients who underwent the treatment procedures.
Discussion
Our double-blind randomized pilot trial of 18 patients with hemiplegia shows that the Ayurvedic treatment procedure Navarakizhi is more effective in improving functional ability than the Ayurvedic procedure pinda sweda using a different type of rice. Although the etiology and pathological basis of hemiplegia and ardhangaroga are described differently in allopathy and Ayurveda, patients with these diseases present with comparable clinical features (Table 1). We constructed a vikruthi (“disease”) table of comparable clinical features after allopathic doctors and Ayurvedic doctors examined the patients together. 19 Developing the vikruthi table followed the model of the clinical comparison in dermatology. 21 This meant that doctors of both systems of medicine were examining the same disease, although each understood the etiology and causative factors differently. In such situations, according to the guidelines of the Department of Health, Government of India, treatment available for ardhangaroga could be studied in trials on the clinical diagnosis of hemiplegia. 22 The classical Ayurvedic texts have discussed prescription of Navarakizhi in ardhangaroga, allowing the direct use of this procedure in clinical trials in India. 9
We have observed in practice that most Ayurvedic treatment centers perform muscle-nourishing procedures using other varieties of rice or cereals because navara rice is expensive and not easily available. Classical Ayurvedic literature describes navara rice as superior to other varieties of rice for this treatment. However, a comprehensive literature search of Ayurvedic publications revealed no studies to support this traditional claim. 23 We therefore undertook a double-blind, randomized, comparative pilot clinical trial to compare the nourishing effect of navara rice with another type of rice, palakkadanmatta.
Outcome measures included muscle strength, muscle tone, median and IQR of deep-tendon reflexes, median and IQR of manual power of both upper and lower limbs, and the individual patient responses in functional ability were assessed through the Berg balance scale. Measures were assessed at baseline, 7 days of pinda sweda procedure, and after 14 days of the treatment with oral medications. The difference observed between the two groups was not significant, since p-values remained above 5% significance levels. IQR analysis demonstrated that navarakizhi was preferable. The reason for nonsignificant values reflects the limitations of this study. Because this trial was a pilot, we recruited only nine patients in each exposure group. In order to avoid spontaneous reduction of symptoms, treatment was performed for 7 days. Ayurveda recommends that navarakizhi should be given for 14 days and followed by an additional procedure called panchakarma for better results. Both recommendations were not included in this pilot trial. Furthermore, Ayurvedic treatment relies upon using fresh ingredients; thus, by concealing the ingredients, we may have reduced the efficacy of the therapeutic agents contained within them. This was highlighted to be an issue with S. cordifolia plant, which showed changes in size over time, due to possible water loss. We found no differences in laboratory results in both groups after administering the treatment.
There is much debate on conducting randomized controlled trials (RCTs) of procedure-based therapies in traditional medicine and Ayurveda.
24
Experts are still divided on this. In this study, we conducted a RCT, using palakkadanmatta rice as control (Table S1, Fig. S1; Supplementary Material is available online at
Conclusions
In conclusion, the outcome of this pilot double-blind randomized clinical trial in nine patients with hemiplegia showed better IQR values for the navara rice group compared to the other nine patients with hemiplegia who were treated using another variety of rice. Navarakizhi needs a larger trial of treating patients with hemiplegia to confirm its superiority over palakkadanmatta. Further research is needed to define the benefits of Navarakizhi in the treatment of hemiplegia and other varieties of neuromuscular diseases similar to ardhangaroga. The authors have also described a method for conducting double-blind, randomized, controlled trials in procedural-based therapies, as found in Ayurveda treatment.
Footnotes
Acknowledgments
We thank National Medicinal Plants Board, Department of AYUSH, Government of India for the funding support (No. NGO/TN–4/2005). We acknowledge the contribution of Dr. M. Chakrapani, Professor, Department of Internal Medicine, Kasturba Medical College, Mangalore and Dr. Narayana Pradeepa, research consultant, Institute of Applied Dermatology for developing the vikrithi table of comparable biomedical terms. We thank Dr. N. Sreekumaran Nair, Professor and Head, Department of Statistics, Manipal University, Manipal, for statistical evaluation. We also thank Prof. M. S. Swaminathan and Dr. K. S. Bose for their constant support and inspiration for taking up this study.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.