
Abstract
Background:
The use of surgically implanted electronic devices for vagus nerve stimulation (VNS) is expanding in contemporary allopathic medical practice as a treatment option for selected clinical conditions, such as epilepsy, depression, tremor, and pain conditions, that are unresponsive to standard pharmacologic interventions. Although VNS device surgeries are considered minimally invasive, they are costly and have surgical and device-related risks; they can also cause serious adverse effects from excessive vagus nerve stimulation.
Objectives:
For millennia, acupuncturists have treated those same clinical conditions by piquering acupoints that are located proximate to the sternocleidomastoid muscle site where the VNS device is implanted on the vagus nerve. The hypothesis of this study is that these acupuncture points produce clinical benefits through stimulation of the vagus nerve and/or its branches in the head and neck region.
Methods:
By using reference anatomic and acupuncture texts, classical and extraordinary acupoints in the head and neck region were identified that are anatomically proximate to vagus nerve pathways there, where the VNS electrode is surgically implanted. The clinical indications of these acupuncture points, as described in the acupuncture reference texts, were examined for similarities to those of VNS.
Results:
This analysis demonstrated marked correspondences of the indications for those lateral head and neck acupoints to the clinical effects (beneficial and adverse) documented for the VNS device in the medical literature. This clinical correspondence, in conjunction with the anatomic proximity of the acupoints to the vagus nerve in the lateral neck, strongly suggests that vagus nerve (and hence the autonomic nervous system) stimulation is fundamental in producing the clinical effects of the acupoints.
Conclusion:
By having anatomic access to the vagus nerve and parasympathetic chain that permits electrical stimulation of those nerves in clinical practice, acupuncture may offer a less costly and safer alternative to implanted VNS devices for treating medically refractory epilepsy, tremor, depression, and pain conditions.
Introduction
T
The vagus nerves are the main conduits of the PANS between the central nervous system and the viscera. The vagus (from the Latin vagus meaning “wandering”) nerves are also known as the pneumogastric nerves because of their known innervation of the lungs and stomach. An estimated 80%–90% of each vagus nerve is composed of afferent fibers that relay the state of the viscera and other peripheral tissues to the central nervous system, 2,3 while their efferent fibers contain about 75% of all parasympathetic outflow. 4 The visceral efferent fibers of the vagus nerves provide parasympathetic innervation to all the organs except the bladder, sexual organs, and distal portions of the colon and ureters. 4 –6
In clinical research trials, neuromodulation of the vagus nerve via implanted electrical stimulators has been demonstrated to have several therapeutic benefits. Several authors have published data concluding that vagal nerve stimulation (VNS) can benefit medication-resistant depression. Nahas et al. reported improvements in Hamilton Rating Scale scores in patients with refractory major depression over a 2-year study period. 7 Dorr and Debonnel demonstrated that VNS produces a large time-dependent increase in the basal neuronal firing rate of dorsal raphe nucleus (serotonergic) and locus coeruleus (adrenergic- norepinephrine) neurons that was not observed in patients receiving long-term antidepressive medications. 8 In a pilot study, Harden et al reported improved mood in patients receiving VNS treatment for refractory seizure disorder. 9 Several studies have already been published on the beneficial role of VNS in the treatment of medication-resistant epilepsy. 10 –13
The U.S. Food and Drug Administration has approved VNS for treatment of medication-resistant seizure disorder and depression, yet this surgical procedure is associated with significant morbidity. 14 Beyond the inherent surgical risks of anesthesia and infection (3%–7%), long-term VNS use may reduce airway flow and respiratory effort 15,16 and worsen obstructive sleep apnea symptoms during stimulation intervals. 16 Sleep apnea is common in persons with chronic epilepsy. 17 Upper airway narrowing may occur with long-term VNS because of chronic contraction of laryngeal and pharyngeal muscles by vagus motor efferent stimulation. 18 Voice alteration (19%), cough (6%), paresthesias (4%), and dyspnea (3%) remain persistent problems among patients 1 year after implantation of VNS and have contributed to a 28% device discontinuation rate within 3 years. 19 VNS may cause sternocleidomastoid spasm 20 as well as facial and laryngeal pain in previously asymptomatic patients. 21 Long-term VNS is associated with symptoms of parasympathetic excess, including bradycardia and asystole, 22,23 as well as chronic diarrhea. 24 VNS implantation also precludes those patients from having future magnetic resonance imaging.
Acupuncture has been demonstrated in animal and human studies to influence vagus nerve activity, whether directly through direct stimulation of its auricular branches 25 –28 or indirectly through reflex activation. 28 –38 Physiologically this results in parasympathetic effects, including reduction of lower esophageal sphincter tone, 25 increase of gastric tone, 26 increased gastric acid secretion, 29 lowered heart rate variability, 27,28,30 lower blood pressure, 39 and lower heart rate. 31,39 Zhang et al. 37 showed that electroacupuncture at GV-14 could suppress experimentally induced epileptiform activity in rats as effectively as VNS.
The purpose of this paper is to demonstrate, on anatomic and physiologic bases, that acupuncture in the lateral head and neck region could theoretically be used to achieve the clinical benefits of implanted VNS devices with less risk and cost.
Vagus Nerve Pathways
The right and left vagus nerves originate in the medulla oblongata, exit the skull base through the jugular foramina, and traverse the neck in the carotid sheath lateral to the carotid artery beneath the sternocleidomastoid muscles (Fig. 1). 5

Course of vagus nerve (in black) through the lateral neck region with sternocleidomastoid removed.
At the level of the subclavian artery, the right vagus nerve provides its recurrent laryngeal nerve branch, which ascends into the neck between the trachea and esophagus to supply motor innervation to the right larynx for speech. The right vagus nerve then crosses anterior to the subclavian artery to descend posterior to the superior vena cava and right mainstem bronchus while contributing to the pulmonary, cardiac, and esophageal plexuses. The right vagus nerve then forms the posterior vagal trunk at the lower part of the esophagus before passing through the esophageal hiatus of the diaphragm to enter the abdomen. 5,40 The right vagus nerve provides more parasympathetic innervation to the cardiac atria than the does left vagus nerve. 3
The left vagus nerve exits the carotid sheath to pass between the left common carotid and subclavian arteries before descending into the thorax on the aortic arch. At the level of the aortic arch, the left vagus provides its recurrent laryngeal nerve branch that supplies motor innervation to the left larynx for speech. It then contributes to the cardiac and pulmonary plexuses before continuing to the distally to supply to the esophageal plexus before entering the abdomen through the esophageal hiatus of the diaphragm as the anterior vagal trunk. 5
Beyond innervating the laryngeal muscles for speech, the vagus nerves also provide innervation to other laryngeal and pharyngeal muscles, including the cricothyroid; posterior cricoarytenoid; levator veli palatini; salpingopharyngeus; palatoglossus; palatopharyngeus; and the superior, middle, and inferior pharyngeal constrictors.
The vagus nerves provide visceral regulation of heart rate (lower), gastrointestinal peristalsis (increase), and sweating (reduce) while also contributing to important motor functions, including speech production and maintaining patency of the laryngeal airway (the posterior cricoarytenoid muscles are the only abductors of the true vocal cords, a function essential for inspiration and expiration).
In the head and neck region, the vagus nerve anastomoses with cranial nerves (facial, glossopharyngeal, spinal accessory, and hypoglossal nerves), spinal nerves (C1 and C2), and the cervical sympathetic chain. 4 –6 The vagus and spinal accessory nerves have several interconnections; and both have communicating branches to the C1 spinal nerve, which itself receives parasympathetic fibers from the superior ganglion (ganglion petrosus) of the vagus nerve. 4 –6
The vagus nerve at the level of the jugular fossa produces two branches termed the meningeal and auricular branches. Its meningeal branch distributes to the posterior fossa and skull base and anastomoses with the C1 and C2 spinal nerves. Its auricular branch innervates the cranial surface of the ear, conchae, dorsal ear, and the floor and posterior wall of the external acoustic meatus 40 and a small part of the tympanic membrane (Fig. 2). 41 The external ear also receives innervation from the greater occipital (C2) and lesser occipital (C2, C3) nerves, which indicates that those nerves can be considered recurrent interconnections with the vagus nerve through the C2 spinal nerve. 5,41
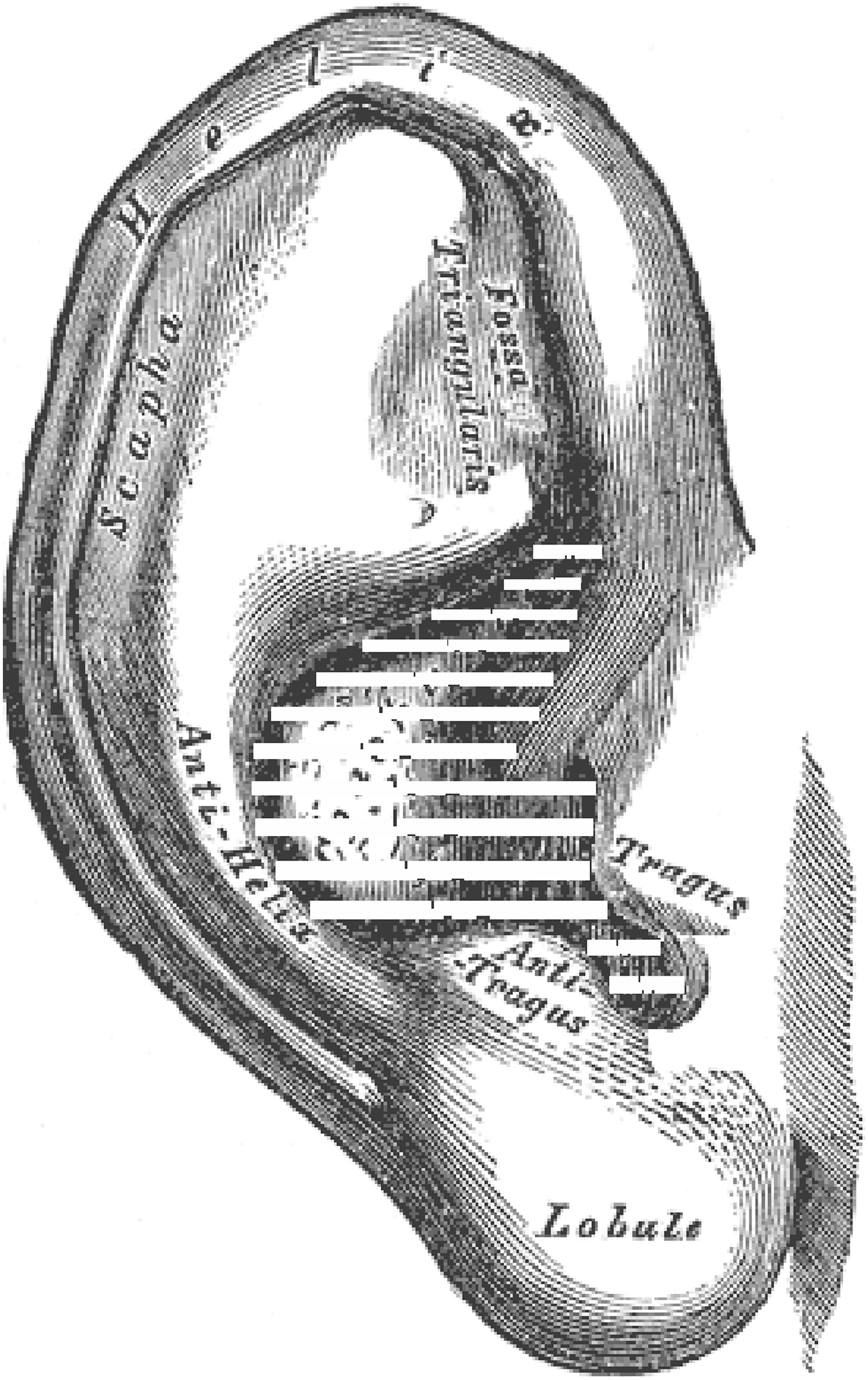
Vagus nerve contribution (shown in white horizontal stripes) to innervation of the external ear.
Acupuncture as a Neuromodulatory Technique Affecting the Autonomic Nervous System
Acupuncture, a part of Traditional Chinese Medicine practice, is a 3000+-year-old healing technique 42 that involves the insertion of fine metal needles into specific body sites to induce physiologic changes that improve pain and illness. There are 787 acupuncture points described in the Shanghai College of Traditional Medicine acupuncture reference, 43 including the 361 “classical” acupoints that were mostly described by 200 AD and reflect the most clinically important points discerned from thousands of years of clinical experience. The approximate locations of these acupoints are described in acupuncture references 43 –45 and are palpable at those sites as a depression in the body surface; at those sites, the acupuncture needle is then inserted to a described depth until the patient experiences a sensation of deqi (a dull, aching, burning, or paresthesias), which is the “true” location of the acupuncture point.
Hui et al. have determined that the deqi sensation represents activation of A-delta and C-fiber afferents. 46 This is compatible with morphologic studies of acupoints that demonstrate a vertical column of loose connective tissue, surrounded by denser connective tissue, just under the skin. Underneath this column, a neuromuscular bundle is present containing lymphatics, arterioles, venules, and small myelinated and unmyelinated nerve fibers. 47 –49
In vivo, Chung et al. have demonstrated that A-δ fiber stimulation produces analgesia outlasting the needle stimulation, 50 and Liu et al. found that C-fiber stimulation has to occur to achieve descending pain inhibition. 51 Further, the physiologic effect of stimulating a given acupuncture point can be markedly attenuated or abolished by anesthetic block of the nerves going to the anatomic site of the acupoint 52 or transecting those nerves. 53 This effect is specific to the nerve supplying a given acupoint. Lu found that sectioning the peroneal nerve eliminated or nearly eliminated the analgesic effect of needling acupoint ST-36 in animals, while sectioning the femoral nerve or tibial nerve or isolating the circulation to the point did not. 53 In an animal experiment using dental pulp nociceptive stimulation (which selectively produces A-δ fiber activation), Toda and Ichioka 54 found that ipsilateral radial nerve stimulation (but not ulnar nerve stimulation) was nearly as effective and followed the same time course as stimulation of LI-4 in producing an analgesic response. 55
This peripheral nerve stimulation with acupuncture in turn produces physiologic effects on other central nervous system structures, including the dorsal horn of the spinal cord, brain stem, reticular formation, nucleus raphe magnus, and nucleus reticularis magnocellularis. 56,57 This has been confirmed with neuroimaging. Functional magnetic resonance imaging studies demonstrate that acupuncture produces specific activation of brain areas associated with both the sensory and the affective interpretation of painful stimuli. Wu et al. identified that the stimulation of certain acupuncture points (LI-4 and ST-36) activates central structures, such as the hypothalamus and nucleus accumbens, but inhibits the rostral part of the anterior cingulate cortex, amygdala formation, and hippocampal complex. 57
As previously noted, acupuncture has been demonstrated in animal and human studies to influence vagus nerve activity, whether directly through direct stimulation of its auricular branches 25 –28 or indirectly through reflex activation. 28 –38 This indirect activation of the vagus nerve may occur from activation of nucleus tractus solitarus, 39,58 a major termination site of vagal afferents. 59
Thus, anatomic, physiologic, and clinical evidence corroborate that acupuncture is a neuromodulatory technique influencing the autonomic nervous system.
Acupuncture Point Anatomic Relationships to the Vagus Nerve
Many important classical acupuncture points are located in the suboccipital and lateral neck regions, where superficial branches of the vagus nerve course. French and Chinese auricular medicine traditions describe ear acupoints influencing visceral function that are located in the conchae of the ears. 41,60 As shown in Figure 2, the auricular branch of the vagus nerve has its distribution primarily to the conchae and the dorsal regions of the ears. 5
Acupoints whose anatomic locations are in the distribution of the vagus nerve and its branches in the head and neck region are as follows: • Skull base acupoints, innervated by meningeal branches of the vagus nerve: GV-15, GV-16, BL-10, GB-12, GB-20, and Anmian (midway between TE-17 and GB-20), as shown in Figures 3 and 4. • Auricular acupoints, innervated by a branch of the vagus nerve to the conchae (Fig. 2). • Anterolateral neck acupoints, innervated by the vagus nerve through its anastomoses with the cutaneous branches of C1–C3 (as shown in Fig. 4): ST-9, ST-10, ST-11, LI-17, LI-18, SI-16, SI-17, TE-16, and TE-17.
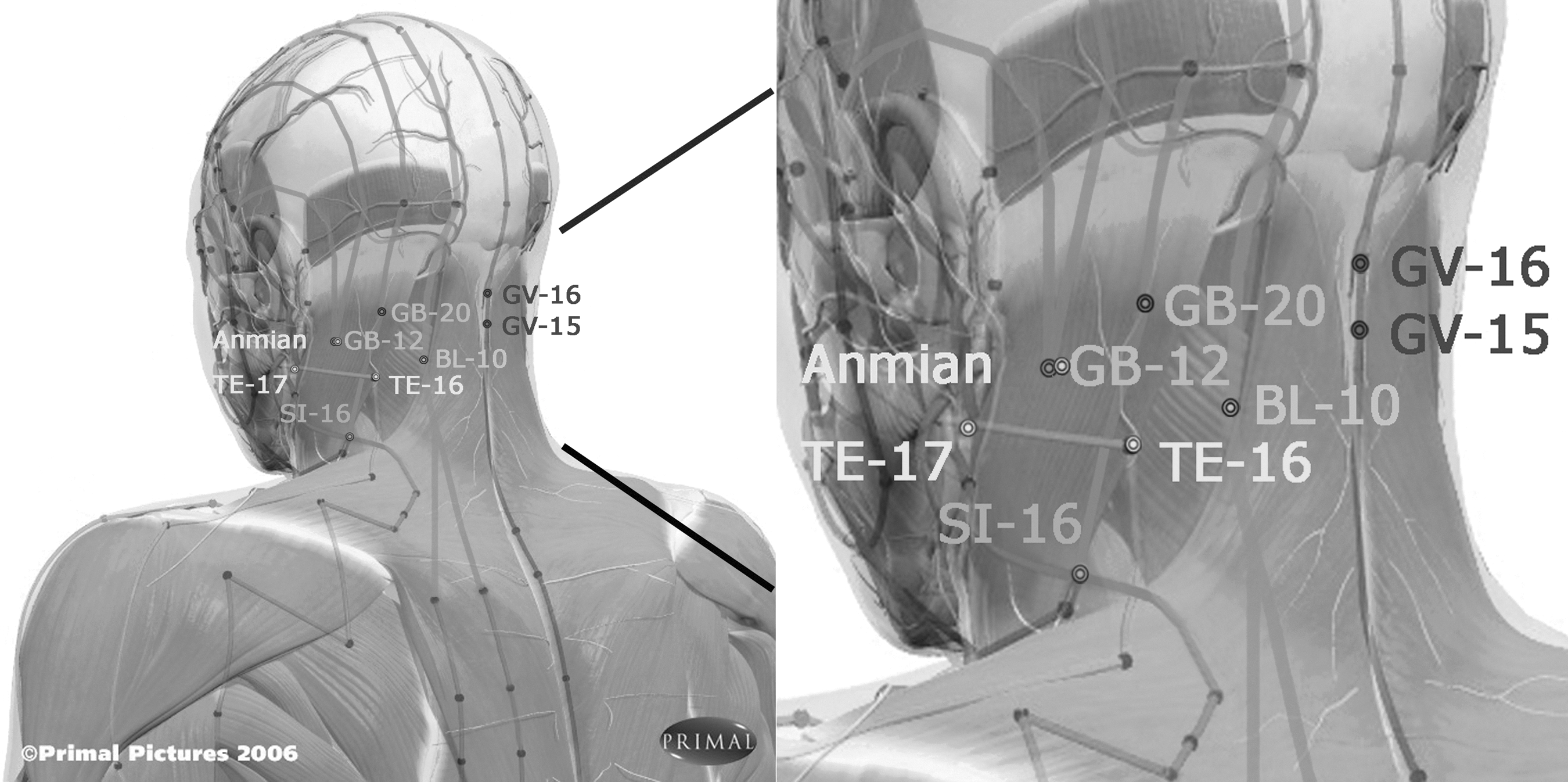
Posterolateral view of head/neck showing acupoints relevant to the vagus nerve.
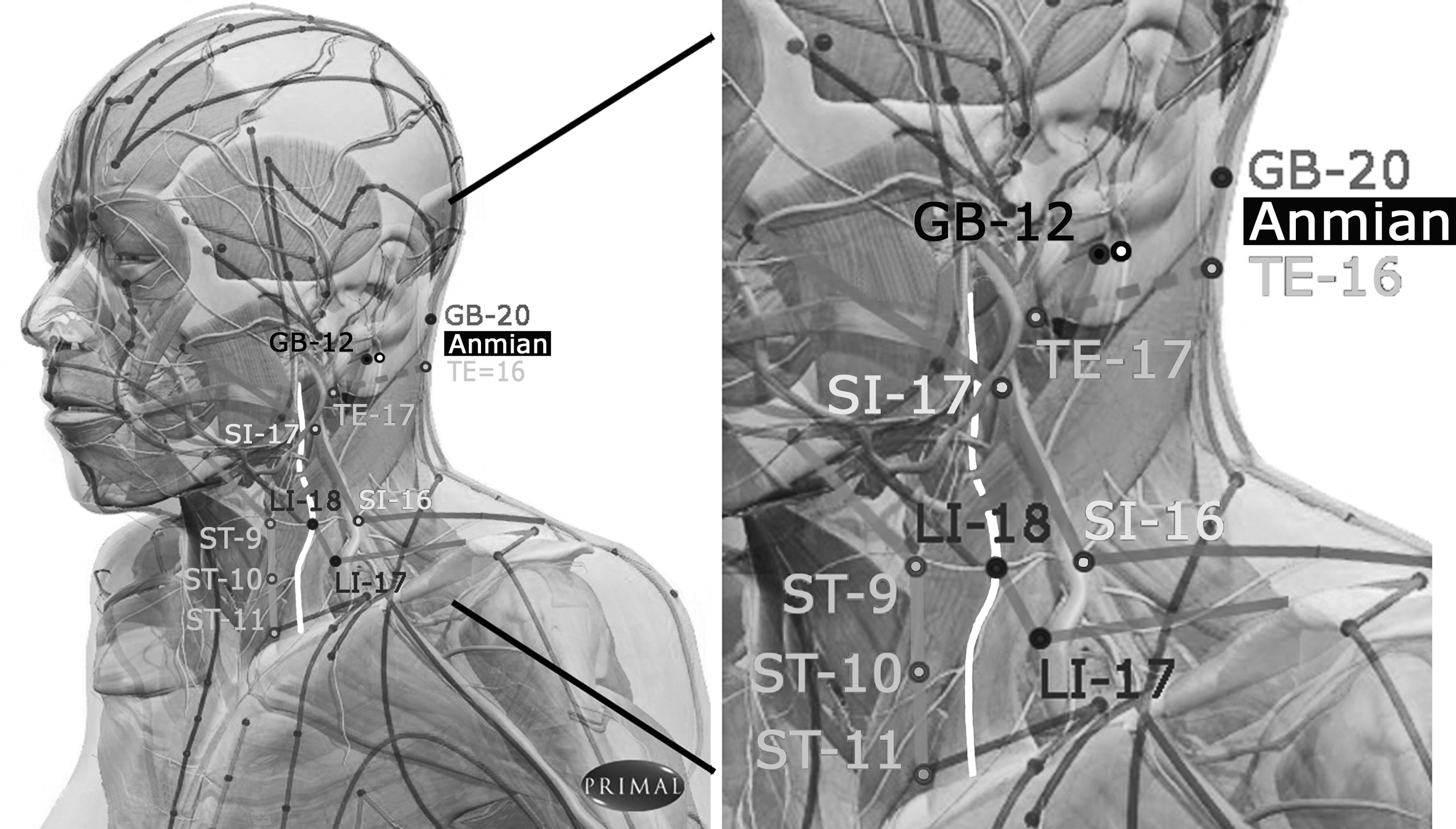
Anterolateral view of head/neck showing acupoints relevant to the vagus nerve (shown in white).
Vagal Nerve Stimulation Devices
In clinical practice, VNS is performed to treat medication-resistant seizure disorder and depression using an electrical stimulator (similar to a cardiac pacemaker) that is implanted in the left pectoral fascia and connected via a tunneled lead to a coil electrode on the left vagus nerve. VNS typically consists of 20- to 30-Hz frequencies, with 30-second pulses of stimulation, repeated every 5 minutes throughout the day. 61
Vagus nerve stimulation with VNS devices produces recurrent contraction of laryngeal and pharyngeal muscles, which may cause upper airway narrowing, 18 increase respiratory effort by reducing airway flow, 15,16 and worsen obstructive sleep apnea symptoms during stimulation intervals. 16 Persistent voice alteration (19%) and cough (6%) also result from chronic laryngeal and pharyngeal stimulation with VNS. 19 VNS may cause laryngeal pain, 21 and long-term stimulation may produce other serious parasympathetic adverse effects, including bradycardia and asystole 22,23 as well as chronic diarrhea. 24
Electrical stimulation of acupoints has commonly been performed in acupuncture treatments since 1930, using frequencies of 1–300 Hz. 62 β-endorphin and enkephalins are released in the central nervous system with low-frequency (2–10 Hz) electrical stimulation, which produces cumulative clinical effects with repeated stimulation. Higher-frequency (≥100 Hz) stimulation releases dynorphins, which have short-duration anti-inflammatory properties in the central nervous system. 62
Acupuncture Effects On Parasympathetic Nervous System Functions
Numerous human experimental studies demonstrate that acupuncture influences PANS activity. Auricular acupuncture reduces lower esophageal sphincter tone in patients with achalasia 25 and heart rate variability in healthy humans. 27,28 Electroacupuncture at body acupoints that included ST-36 reduces vagus-mediated gastric acid secretion. 38 Stimulation of PC-6 reduces the parasympathetic mediated, low-frequency component of heart rate variability in patients with coronary artery disease, 30 and magnetopuncture of PC-6 and GV-14 had similar effects in healthy individuals. 35 Human heart rate is reduced through acupuncture stimulation of PC-4, with this effect at least in part mediated via the vagus nerve (because atropine attenuates this heart rate reduction). 36 Acupuncture at LI-4 and LU-6 31 and ST-36 34 similarly reduces heart rate in humans.
Similar clinical effects of acupuncture on parasympathetic nerve activity have been noted in animal (rat) studies. Auricular acupuncture in rats has been demonstrated to increase gastric tone/pressure 26 and reduce systolic blood pressure and heart rate. 39 Stimulation of body acupuncture point ST-36 in rats enhances gastric acid secretion, an effect which is eliminated by vagotomy. 29 Electroacupuncture at ST-36 increases gastric motility and reduces heart rate variability 26,39 that reflects increased vagus nerve activity. 39 Longhurst and Zhou 63 have postulated that the acupuncture stimulation inhibits SANS activity, modulates the endocrine system, and modulates the activity of cardiovascular presympathetic neurons in the rostral ventrolateral medulla as well.
As shown in Table 1, review of acupuncture reference texts demonstrates that acupoints located in the vagus nerve distribution in the suboccipital and neck regions (Figs. 3 and 4), including GV-15, GV-16, GB-12, GB-20, TE-17, and Anmian have clinical indications and effects that are similar to the known clinical indications and effects of VNS. 43 –45,60,64,65 These indications include epilepsy and bipolar disorder, 43,44,65 as well as palpitations and hypertension. 43,44,65 We postulate that the heart rate and blood pressure reductions result from increased parasympathetic tonus produced by stimulation of the vagus nerve branches in the suboccipital and mastoid regions where these acupoints are located.
References 4 and 5.
Reference 43.
Reference 65.
Reference 44.
The other acupoints in Table 1 are in the lateral neck region anatomically adjacent to the sternocleidomastoid muscle (Figures 3 and 4) which overlies the vagus nerve there. The described clinical indications of these acupoints differ substantially from those in the suboccipital and mastoid regions; generally they are indicated more for pharyngeal, laryngeal, and pulmonary disorders, such as sore throat, difficulty swallowing, hoarseness, voice loss, cough, dyspnea, asthma, and hypotension. 43,44,65 These clinical states may be those of parasympathetic excess that can be treated by sedation of these acupoints to reduce parasympathetic tonus.
Discussion
Acupuncture is the most enduring healing tradition, having been in continuous clinical use for approximately 3000 years. The acupuncture literature has published experimental and anecdotal evidence of its beneficial effects on a long list of conditions, including seizures, depression, allergies, and bowel diseases.
The veracity of acupuncture's benefits in treating seizures has been questioned, 66 –68 and a recent Cochrane Collaboration study reviewed 11 small trials with over 914 participants to examine the effectiveness of acupuncture for seizures. Despite finding that acupuncture reduced the duration and frequency of seizures episodes, the authors concluded that because the examined studies were of poor methodologic quality and had only short-term follow-up, there was insufficient evidence to recommend acupuncture as a treatment for epilepsy. 69 As previously discussed, Zhang et al. 37 have shown that in a rat model, electroacupuncture at GV-14 suppresses experimentally induced epileptiform activity as effectively as VNS.
The current anatomic and clinical analysis presents 13 classical acupuncture points and one extrameridian acupoint (Anmian) that are demonstrated to be anatomically proximate to the vagus nerve and its branches in the suboccipital, mastoid, and sternocleidomastoid regions (Table 1, Figs. 3 and 4). Acupuncture reference texts 43,44,65 document that six of these acupoints are located along the mastoid and suboccipital regions and have indications that include treatment of seizures and manic-depression (such as VNS), while the other eight acupoints are anatomically adjacent to the sternocleidomastoid muscle and have indications for treating pharyngeal, laryngeal, and pulmonary disorders including sore throat, difficulty swallowing, hoarseness, voice loss, cough, dyspnea, asthma and hypotension. These findings imply that stimulation of vagus nerve branches along the mastoid and suboccipital region (rather than in the lateral neck site used for VNS implantation) may have greater clinical efficacy in treating refractory seizure and depression disorders while simultaneously reducing risks of cardiovascular, pulmonary, gastrointestinal, and speech adverse effects. 14 –24 These findings should be studied experimentally in animal models.
The fundamental clinical overlap of the clinical effects of these 14 acupoints with the known clinical effects of VNS benefitting seizure and depressive disorders (as well as its cardiac, pulmonary, gastrointestinal, and speech adverse effects), in conjunction with the anatomic correspondence of these acupoints with the course of the vagus nerve and its branches in the suboccipital, mastoid, and lateral neck regions, strongly suggests that these the clinical effects of these acupoints result from stimulation of the vagus nerve and its branches there. This could be confirmed by anesthetic block or transection of appropriate vagus nerve branches in an experimental setting.
Acupuncture has been demonstrated in animal and human studies to influence vagus nerve activity, whether directly through direct stimulation of its auricular branches 25 –28 or indirectly through reflex activation. 28 –38 This indirect activation of the vagus nerve may occur from activation of nucleus tractus solitarus, 39,58 a major termination site of vagal afferents. 59 These studies confirm that acupuncture has neuromodulatory effects on the autonomic nervous system, which can be used clinically to normalize autonomic balance and potentially favorably alter the course of disease. Combining modern neuroanatomic knowledge with the extensive clinical knowledge provided by Traditional Chinese Medicine could lead to more efficacious, less expensive interventions with fewer adverse effects than implanted stimulation devices or pharmacologic agents.
Conclusion
Vagus nerve stimulation devices have been introduced in the last two decades as a novel treatment for refractory seizure and depression conditions. For millennia, however, Traditional Chinese Medicine practitioners have treated those same clinical conditions by piquering acupuncture points that are anatomically proximate to the vagus nerve or its cutaneous branches to the ear, mastoid, and suboccipital regions. Acupuncture has in both animal and human studies been demonstrated to directly or indirectly modulate parasympathetic nervous system activity through the vagus nerve. Other observed clinical effects of vagus nerve stimulation, including voice alteration, cough, dyspnea, bradycardia, and diarrhea (symptoms of parasympathetic excess), as well as sternocleidomastoid spasm, mirror the clinical effects described for classical acupoint stimulation in the sternocleidomastoid region, where the vagus nerve anatomically courses deep to the sternocleidomastoid muscle.
These findings, which are based in neuroanatomy as well as basic and clinical research evidence, suggest that stimulation of the autonomic nervous system is of fundamental importance in acupuncture's clinical effects. This could be validated by future experimental and clinical research studies that examine how anticholinergic drugs as well as anesthetic blockade or transection of vagus nerve branches in the head and neck region influence the clinical effects produced by acupuncture point stimulation there.
Footnotes
Author Disclosure Statement
No competing financial interests exist.