
Abstract
Background:
Traditional Chinese acupuncture (TCA) is an effective alternative treatment in migraine headache. The aim of this study was to compare the therapeutic effect of Yamamoto new scalp acupuncture (YNSA), a recently developed microcupuncture system, with TCA for the prophylaxis and treatment of migraine headache.
Methods:
In a randomized clinical trial, 80 patients with migraine headache were assigned to receive YNSA or TCA. A pain visual analogue scale (VAS) and migraine therapy assessment questionnaire (MTAQ) were completed before treatment, after 6 and 18 sections of treatment, and 1 month after completion of therapy.
Results:
All the recruited patients completed the study. Baseline characteristics were similar between the two groups. Frequency and severity of migraine attacks, nausea, the need for rescue treatment, and work absence rate decreased similarly in both groups. Recovery from headache and ability to continue daily activities 2 hours after medical treatment showed similar improvement in both groups (p>0.05).
Conclusion:
Classic acupuncture and YNSA are similarly effective in the prophylaxis and treatment of migraine headache and may be considered as alternatives to pharmacotherapy.
Introduction
M
Acupuncture is a traditional Chinese intervention that has been widely used in the prevention and treatment of migraine headaches. A Cochrane review suggested that acupuncture is at least as effective as, or possibly more effective than, prophylactic drug treatment, and has fewer adverse effects. 3 However, there is no consensus that classic acupuncture is more effective than sham interventions. 4 –7 Yamamoto new scalp acupuncture (YNSA) is recently developed variation of acupuncture that has been proposed to be effective in the treatment of acute and chronic pain and neurologic disorders. 8 There appear to be no other studies comparing the efficacy of Traditional Chinese acupuncture (TCA) and YNSA in the treatment of migraine headache. This study was conducted to compare the effects of these two treatment modalities on the frequency and severity of migraine attacks, response to rescue treatment, daily activity, and nausea and vomiting.
Methods
Between March 2009 and April 2011, a total of 80 patients with migraine headache aged 18–65 years referred to an acupuncture clinic were enrolled. Migraine was diagnosed according to diagnostic criteria of the International Headache Society. 9 Patients with other severe pain disorders; bleeding diathesis; or severe diseases of the heart, lung, liver, kidney, or other organs, as well as pregnant or lactating women were not enrolled. All patients receiving medical treatment for headaches were advised to continue their treatment, and those not receiving any treatment were advised to take 650 mg acetaminophen for their migraine attacks. Patients were randomly assigned to receive TCA or YNSA. Block randomization was done by a table of random numbers. The study was approved by the regional ethics committee, and written informed consent was obtained from all patients.
Baseline evaluation for pain characteristics and presence of complications was performed using a questionnaire that included a pain visual analogues scale and migraine therapy assessment questionnaire. One resident of anesthesiology who was blinded to the assignments recorded outcome measures from the baseline period to the 12th week after randomization in predefined intervals.
Intervention protocol
In the TCA group, on the basis of clinical symptoms and traditional Chinese physical examination and diagnosis, several points from the LI4, ST8, ST36, BL2, GB14, TB5, GB8, tai yang, SI3, BL10, BL60, GB20, LIV3, KID1, DU20, si shen cong, LU7, SP6, LIV2, ST36, and REN6 acupuncture points were selected. Needling was performed by using steel needles (Huan Qiu, China) with different sizes and diameters for different points. In the YNSA group, on the basis of clinical symptoms and diagnostic points in the hands, neck, and abdomen, different points, especially A1-7, M1-3, and Y psilon points, were selected for the intervention (Fig. 1). Needling was done with 25-mm steel needles (Huan Qiu). Needles were inserted to a depth of 10–15 mm and were manually manipulated by rotation methods to achieve de qi. The interventions in the two groups were performed by an experienced physician who had worked with acupuncture for 15 years.
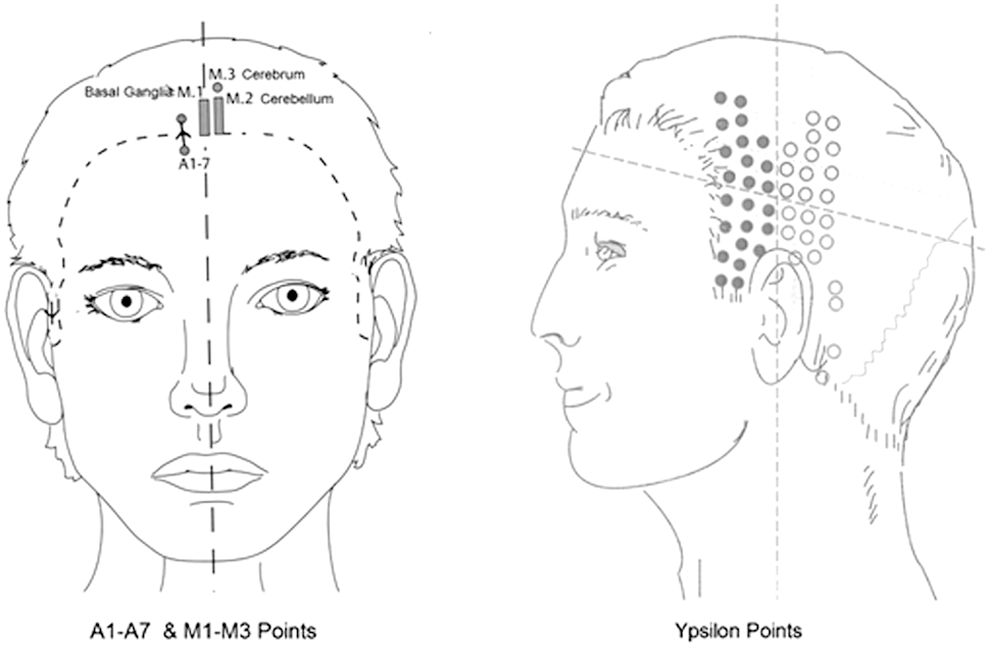
Yamamoto new scalp acupuncture points.
A total of 18 sessions of acupuncture treatments (30 minutes each) in three courses were performed. Each course included six sessions of acupuncture treatments given every other day, with 1 week rest between the courses. The patients fulfilled the questionnaire at the end of the second and eighth weeks of treatment, as well as 1 month after the last session of treatment.
Statistical Analyses
The required sample size was calculated with respect to severity of headache score. From the literature, a standard deviation of 20 mm was expected, and the analysis was carried out with respect to detecting a difference of at least 15 mm for this parameter. On the basis of a power of 0.8 to detect a significant difference and an α level of 0.05, 36 patients are required for each group. Another 4 patients (10% of calculated sample size) were added to compensate for dropouts. Data are presented as mean±standard deviation. The analyses were performed with Mann-Whitney U test and independent Student t-test for quantitative variables. All the comparisons were two tailed. Any p values<0.05 were considered to represent statistically significant differences. Statistical analysis was performed with SPSS, version 16.0, software (SPSS Inc., Chicago, Illinois).
Results
Demographic variables, duration of migraine, and the frequency of weekly headaches were similar between the two groups (Table 1). All the recruited patients completed the study period and were recruited into the analysis.
Values expressed with a plus/minus sign are the mean±standard deviation.
YNSA, Yamamoto new scalp acupuncture.
The frequency and severity of migraine attacks significantly decreased in YNSA and TCA groups (Figs. 2 and 3). However, there were no differences between the trends in two groups. At baseline, the rates of work absence due to headache were 47.4% in the TCA group and 55.3% in the YNSA groups. One month after the intervention, the rates decreased to 11.1% and 18.9%, respectively (p>0.05). At baseline, the need for rescue treatment for headache was reported in 12.5% of patients in each group. One month after the intervention, this index was similarly decreased to 2.5% of patients in both groups.

The mean frequency of weekly headaches. YNSA, Yamamoto new scalp acupuncture.
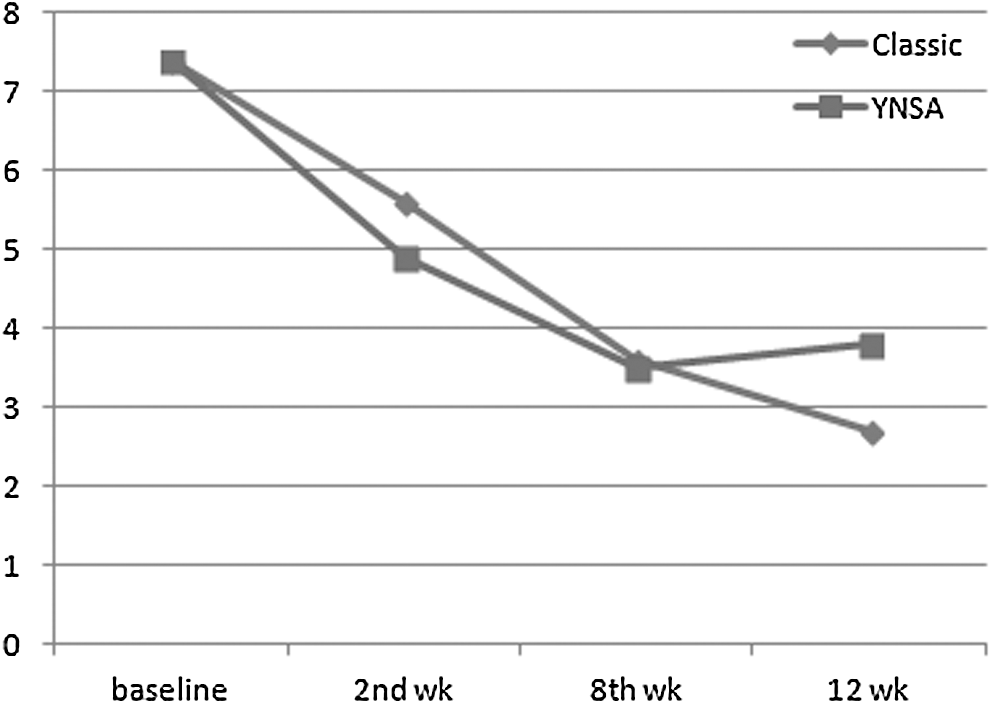
Pain score in assessment intervals.
Recovery from headache and ability to continue daily activities 2 hours after medical treatment showed similar improvement in both groups (p>0.05). Assessment of severity of nausea did not significantly differ between two groups during the follow-up period (Table 2).
Unless otherwise noted, values are the number (percentage) of patients.
YNSA, Yamamoto new scalp acupuncture.
Discussion
Findings of this study show that both YNSA and TCA can effectively reduce the frequency and severity of migraine attacks and improve the response to rescue treatments. Both methods similarly reduced the need for rescue treatment and work absence rate and improved daily activities of patients. Regarding the efficacy and low complication rate of acupuncture methods, 3 this treatment may be appreciated as an appropriate alternative choice for drug prophylaxis in patients with migraine. The current results support the idea that the acupuncture method has little effect on the outcome, suggesting that point-specific effects play a small role in the overall response. 10 Finally, YNSA, which requires less needling than TCA does, may be regarded as an efficacious and feasible modality in experienced hands.
YNSA was introduced by Toshikatsu Yamamoto in 1973. It is a microsystem of the scalp that uses anatomic and channel points to treat disorders. YNSA differs from all other microsystems in that it uses an extra palpatory diagnostic system, YNSA neck diagnosis, to determine which channel point should be manipulated. Using this additional diagnostic tool makes the intervention more specific, with less needling required.
YNSA is not like classic acupuncture in that it uses a different somatotope. 11 YNSA is a microsystem, a brief and direct way to balance the body's system. However, it has limited capabilities compared with the macroacupuncture system, which encompasses clinical, spiritual, and a single body acupoint's specific physiologic effects. Yet when effective, YNSA could be a feasible substitute for TCA, with immediate therapeutic responses. Earlier studies have reported the clinical utility of YNSA in patients with cerebrovascular disorders, particularly those with stroke. 12,13 The findings of this study may extend the clinical application of YNSA to patients with migraine.
Patients with migraine may require more and more drugs for headache prophylaxis. Over the long term, depressed mood and complications of medications can lead to poor compliance with drug prophylaxis in these patients. As can be expected, a significant proportion of patients do not regularly use their medications. In this study, all recruited patients completed the course of treatment. In comparison, another study reported that only 2 of 59 patients randomly assigned to 12 weeks of acupuncture treatment withdrew prematurely from the study. 14 It would be reasonable to assume that in the case of similar efficacy, YNSA may be even better tolerated than TCA because fewer needling sites are required.
In this study, the therapeutic effects of YNSA and TCA methods on all outcome measures increased with more treatment sessions. Patients were followed for 1 month, and further improvement after the interventions was noted. Investigators of most of the earlier trials speculated that the effect would have increased even further with a longer follow-up period. 4,6,15 However, scarce data on the long-term effects of acupuncture exist. One study followed the patients for 9 months after the cessation of treatment and found that the clinical benefits of acupuncture still exist. 16 Contrary to these findings, a small study in 39 patients with migraine headache reported that 6 months after the intervention, 54% of patients had relapsed to their preacupuncture state. 17 Clearly, further studies are required to evaluate the long-term effects of acupuncture, of any method, on the frequency and severity of migraine headache. This will help clinicians plan for acupuncture treatments in proper intervals.
The study did have some limitations. The patients who attended the acupuncture clinic may differ from a cross-section of the population with migraine headache and may not truly represent the characteristics of the affected patients. These patients generally have more positive attitudes toward alternative medicine that may affect their response to treatment. This study did not intend to compare the therapeutic efficacy of TCA and YNSA with sham acupuncture or drug prophylaxis. Patients were followed for 1 month after cessation of treatment. Thus, the long-term benefits of acupuncture of either method are uncertain.
Another limitation of the present study was that the patients were not blinded to the interventions because of the different needling sites in two groups. However, the assessors and the analyzer were blinded to the assignments. For ethical reasons, patients were allowed to continue their medications. This may raise the question about the similarity in the patients' baseline condition. Of note, the primary evaluation confirmed that the frequency and severity of headache, as well as other outcome measures, were similar between the two groups.
Footnotes
Disclosure Statement
No competing financial interests exist.