
Abstract
Objective:
Evidence is accumulating, predominantly among clinical trials in adults, that yoga improves blood pressure (BP) control, with downregulation of the hypothalamic–pituitary–adrenal (HPA) axis and the sympathetic nervous system (SNS) projected as underlying mechanisms. This pilot study assessed whether Hatha yoga has the potential to reduce BP among youth and whether dampening of the SNS and/or HPA activity is a likely pathway of change.
Design:
Thirty-one seventh graders were randomly assigned to a Hatha yoga program (HYP) or attention control (AC) music or art class. Baseline and 3-month evaluations included resting BP; overnight urine samples; and saliva collected at bedtime, upon awakening, and at 30 and 60 minutes after awakening for α-amylase and cortisol assays.
Results:
Twenty-eight (14 in the HYP group and 14 in the AC group) students were assessed both before and after the intervention. BP changes from pre- to post-intervention were −3.0/−2.0 mmHg for the HYP group and −0.07/−0.79 mmHg for the AC group (p=0.30 and 0.57, respectively). Changes in systolic BP (SBP)/diastolic BP (DBP) for the prehypertensive (75th–94th percentiles for SBP) subgroup analyses were −10.75/−8.25 mmHg for the HYP group (n=4) versus 1.8/1.0 mmHg for the AC group (n=5) (p for SBP=0.02; p for DBP=0.09). Although no statistically significant group differences were observed with changes in SNS or HPA awakening curves (area under curve for α-amylase and cortisol, respectively), a small to moderate effect size was seen favoring a reduction of α-amylase activation for the HYP group (Cohen d=0.34; prehypertensive d=0.20).
Conclusions:
A school-based Hatha yoga program demonstrated potential to decrease resting BP, particularly among prehypertensive youth. Reduced SNS drive may be an underlying neurohormonal pathway beneficially affected by the program. A large-scale efficacy/effectiveness randomized clinical trial is warranted.
Introduction
E
Long-term exposure to psychological stress has been identified as an independent risk factor for EH. 7,8 Persistent hyperactivation of the sympathetic nervous system (SNS) and the hypothalamic–pituitary–adrenocortical (HPA) axis have been implicated as two underlying mechanisms linking stress exposure to EH development. 9 –12 Briefly, acute stress exposure stimulates the SNS, characterized by release of catecholamines, norepinephrine, and epinephrine, which have inotropic and chronotropic influences on the heart that lead to increased heart rate and decreased pre-ejection period, as well as vasoconstrictive mediated increases in BP. 13 The HPA axis is also activated, as denoted by release of cortisol. The HPA axis affects BP regulation mainly via effects of cortisol on sodium reabsorption and volume homeostasis. 14 Collectively, the SNS and HPA axis stimulate multiple BP regulatory systems, including the renin–angiotensin–aldosterone system. Angiotensin II is released, which increases BP via direct vasoconstriction, and results in further activation of the SNS and potentiation of the effect of norepinephrine. Angiotensin II also induces increased aldosterone production, and their combined effects influence volume homeostasis through stimulating thirst centers and proximal tubular reabsorption of sodium. This increase in sodium and water retention leads to a rise in cardiac output and delayed BP recovery. The augmented sodium retention enhances vasoconstrictive effects of norepinephrine on peripheral vasculature, which further increases BP via increased total peripheral resistance. 15 –17 These interconnected responses all contribute to acute vasoconstrictive mediated BP increases and/or delayed BP recovery to prestress exposure levels. Repeated cascading of hormonal and peptide activity across systems contributes to morphologic alterations and vascular dysfunction, leading to EH. Chronic stressors affect the balance of these hormone levels, and repeated life stressors have been reported over time to desensitize the HPA axis by blunting diurnal and reactive cortisol levels while also heightening sensitivity in SNS activity during acute stresses. 14,18,19
Evidence indicating that chronic stress contributes to EH and CVD development has resulted in a plethora of mind–body stress reduction programs, including various forms of yoga, among hypertensive adults and those at high risk for EH (e.g., stage 2 prehypertension). 20,21 Most of these studies have been case reports or uncontrolled trials with numerous methodologic limitations and infrequent evaluation of underlying neurohormonal mechanisms, such as SNS and/or HPA axis function (see reviews 22 –25 ). To our knowledge, only six randomized controlled trials (RCTs) have investigated effects of yoga on BP in adults with prehypertension or EH. Collectively, these RCTs ranged in duration from 6 weeks to 9 months, with observed changes in SBP/DBP ranging from −1/−2.6 to −33.4/−26.3 mmHg. 26 –31
Epidemiologic evidence supports the importance of maintaining BP control during childhood. 32 BP percentile ranking relative to peers is relatively consistent from late childhood into adulthood and predicts future EH. 33 Thus, youth with BP between the 75th and 94th percentiles for age, sex, and height have an increased risk of developing EH and CVD. 34 –36 Furthermore, incidence of EH has risen in recent years among youth, 37 particularly among minority groups, in which rates are now estimated at 5%–12%. 38 Early onset of EH contributes to earlier deleterious morphologic and functional changes to the kidneys, heart, and vasculature and in youth is expressed in part via left ventricular hypertrophy, decreased elasticity, and damage to arterial walls. 39 Collectively, these changes contribute to earlier manifestation of diabetes, end-stage renal disease, stroke, and heart failure, 39 thus increasing lifelong medical costs and premature death and disability. 3,32
Although yoga has received attention as a mind–body alternative approach to reducing BP in adults, little is known about its effect on BP control in youth. 40,41 No pediatric RCT appears to have evaluated effects of yoga on BP and indices of SNS or HPA axis function. This pilot RCT was designed to investigate preliminary indications of the effect of a school-based Hatha yoga program on resting BP and indices of SNS and HPA axis activation on youth. On the basis of previous yoga trials with adults 26 –31 and youth, 42,43 it was predicted that those who practiced Hatha yoga for 12 weeks would exhibit greater reductions in resting BP and SNS (i.e., salivary α-amylase), and HPA axis (i.e., salivary cortisol) activation compared with an attention control group.
Materials and Methods
Study population
Fifty seventh-graders from a Charleston, South Carolina, science and math charter school were invited to participate in the 12-week study. Exclusion criteria included previous exposure to formalized yoga programs and youth identified as hypertensive according to percentiles of age, sex, and height. 35 No youth participated in school-based physical education classes during the study. Thirty-one students were enrolled after informed parental consent and child assent were obtained. The students were then randomly assigned by school administrators to a semester-long Hatha yoga program (HYP) or music or art program (attention control [AC]). A battery of physiologic measures (described below) was taken before and after the 12-week protocol. The Charleston County Public Schools and Medical University of South Carolina review boards granted permission to conduct the study.
Measures
Anthropometrics
Testing at the school included height (via stadiometer) and weight (via Detecto scale, Cardinal Scale Manufacturing Co., Webb City, MO) taken by trained research staff using established protocols. 44
Resting BP and HR
Supine heart rate, SBP, and DBP were recorded from the right arm at heart level, while the patient rested, by using GE ProCare 200 monitors (GE Healthcare, Milwankee, WI) for 10 minutes (readings at minutes 0, 6, 8, and 10). BP measurements for all participants were taken at the same time of day at each assessment (i.e., before or during the first class of the day). BP was assessed by averaging the last three readings on each evaluation. Youth with BP ≥95th percentile were excluded from the study and referred for further screening by a health care professional. 35
Saliva sampling
Salivary cortisol and α-amylase are correlated to HPA axis and SNS response in adults and young adults, respectively, and are used as a noninvasive method to study these mechanisms. 45 –47 Following BP screening, students were provided four 1.5-mL cryovials placed vertically in a small cardboard tray. A demonstration of the procedures and written instructions for parental assistance were provided. Saliva samples were collected with a minimum of 0.5 ml (0.75 ml desired) per vial, with times recorded on the vial at bedtime, upon awakening and before leaving the bed, and 30 and 60 minutes afterward. Sampling vials were returned in a sealed cardboard box to the school that morning. All samples were subsequently frozen at −80°C. Salivary cortisol and α-amylase levels were assayed in duplicate in a single-batch assay at the Cortlab Assay Laboratory at the University of Trier (Trier, Germany). Cortisol concentration was determined by using a time-resolved fluorescence immunoassay. The α-amylase levels were measured through absorbance measured by a kinetic plate reader at 405 nm using substrate solution (CNP-G3).
Study intervention
Both groups (HYP and AC) received 90-minute sessions on alternating days in accordance with the school calendar (cycles of two sessions 1 week followed by three sessions the next week structured in a classroom setting). Hatha yoga was practiced by the children in the HYP group, whereas the AC group attended and participated in music and art classes that were led by a teacher and were part of the regular school curriculum. Both HYP and AC groups received the same frequency and duration of instruction in their respective sessions.
Hatha yoga focuses on strength and flexibility training 48 and was taught by a team of four Yoga Alliance–certified instructors. Instructors rotated teaching days, with one instructor present during class time. The schedule for each yoga session is described in Table 1. Content for each session was built on the knowledge of prior classes. General concepts were introduced and practiced early in the intervention, with progressively more poses and variations of instruction incorporated throughout the 12-week period. Worksheets illustrating the postures were given to each student. During the class, discussion included ways to use yogic techniques outside of class and at home by applying what they learned in different environments.
Statistical analysis
Groups were compared at preintervention for baseline differences using independent t-tests for continuous variables and chi-square tests for categorical variables. BP and anthropometric change scores from pre- to postintervention were calculated for each group and compared using pooled t-tests. Subgroup analysis of change scores for prehypertensive participants used both t-tests and nonparametric Wilcoxon rank-sum tests. Following van Veen and colleagues' approach, 49 the series of four salivary cortisol and α-amylase levels for the entire sample were examined by using area under the curve (AUC) for each participant at pre-and postintervention. Normality was tested by using square-root transformations and Shapiro-Wilk tests. Differences between groups were assessed using the Wilcoxon rank-sum tests and longitudinal analysis using mixed models adjusted for preintervention AUCs. The Cohen d was used to calculate effect size. Data were analyzed by using SPSS WIN V.17 software (version 19.0; IBM, Armonk, NY) and SAS software, version 9.3 (SAS Institute, Inc., Cary, NC). Given the pilot nature of the study, no adjustments for the multiple analyses/outcomes were used to minimize type II errors
Results
Figure 1 shows the flow of study participants. After the study exclusion criteria were applied, 31 (18 male) students agreed to participate, with 16 and 15 in the HYP and AC groups, respectively. Three students were excluded during the trial because of nonadherence or extraneous reasons (i.e., missed school days, change in schools, hypertension at preintervention), which left 28 participants (14 in the HYP group and 14 in the AC group; 43% African Americans; 57% girls; mean age±standard deviation, 12.3±0.4 years) in the final analyses.
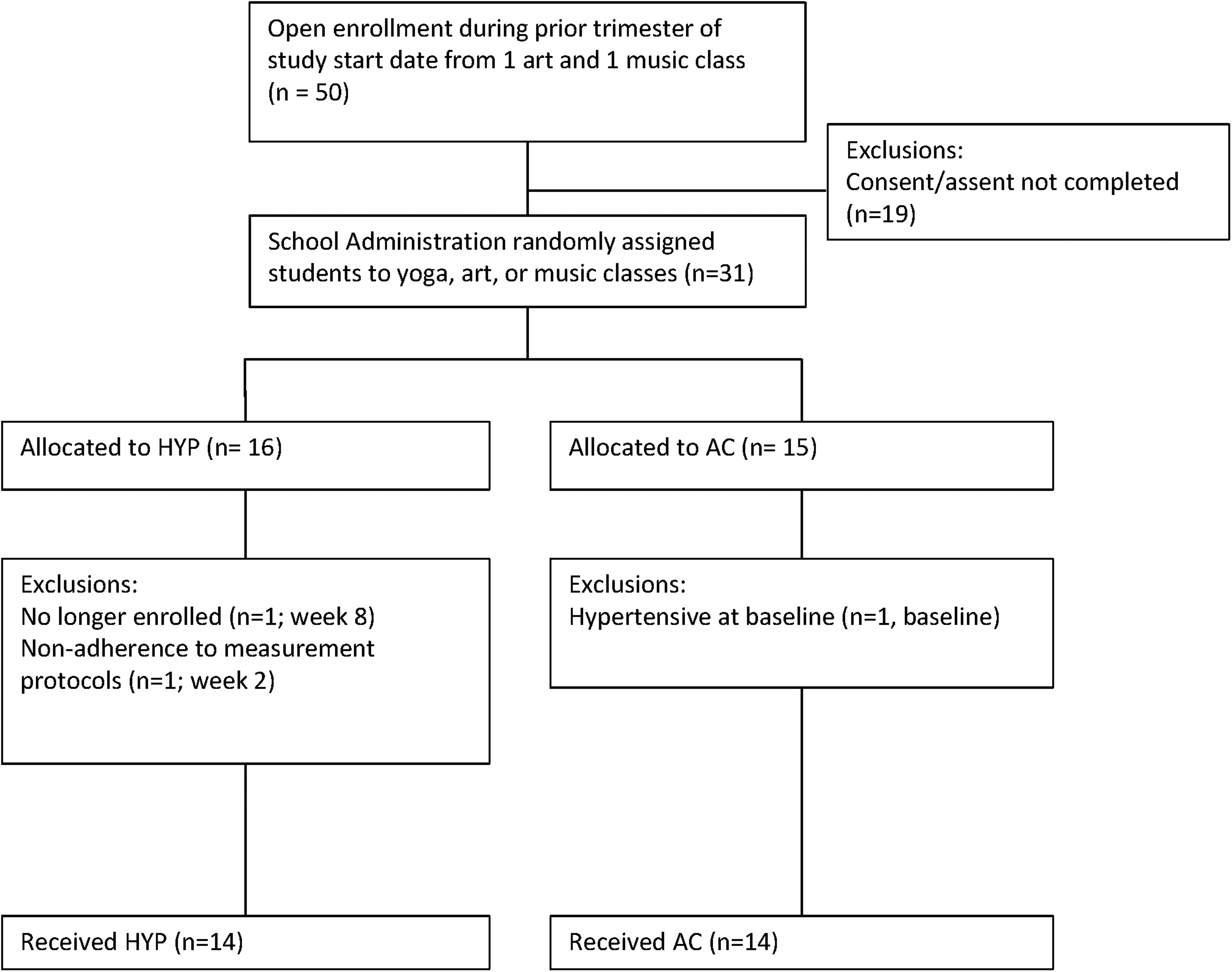
CONSORT (Consolidated Standards of Reporting Trials) diagram. AC, attention control group; HYP, yoga group.
Descriptive characteristics
No statistically significant group differences on any preintervention baseline characteristics were found (Table 2). Groups did not significantly differ for ethnicity and sex (p>0.45 for all comparisons) or for attendance to school sessions (92.8% in the HYP group and 95.8% in the AC group; p=0.09).
Unless otherwise noted, values are expressed as mean±standard deviation. The p-values were calculated by using chi-square tests and t-tests.
HYP, yoga group; AC, attention control group; BMI, body–mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Resting BP and heart rate
Analysis involving the entire cohort revealed that the HYP group exhibited changes in SBP/DBP of −3.0±7.0/−2.0±5.5 mmHg, compared with −0.07±7.8/−0.79±5.6 mmHg in the AC group (SBP: p=0.30; DBP: p=0.57) (Table 3). Subsequent subgroup analyses with the prehypertensive subgroup (SBP 75th–94th percentile) were conducted by using the Wilcoxon rank-sum test (HYP group: n=4; AC group: n=5). The prehypertensive HYP subgroup showed large BP reductions for both SBP (HYP group: −10.75±4.3; AC group: 1.80±5.7 mmHg; p=0.02) and DBP (HYP group: −8.25±4.5; AC group: 1.0±6.2 mmHg; p=0.06). No change was found for resting heart rate or any other anthropometric variable between groups (all p>0.11). Percentile change in prehypertensive classification status revealed that 100% (4 of 4) of the HYP group compared with 40% (2 of 5) of the AC group changed classification to normotensive after the intervention, with a mean percentile change of −34th/−16th percentile (SBP/DBP percentile scores; SBP: p=0.03) for the HYP group compared with almost no change in the AC group.
Values calculated as postintervention value minus preintervention value (reported as mean±standard deviation).
For all patients, p-values were obtained from independent sample t-test. For the prehypertensive group, p-values were obtained from Wilcoxon rank-sum test.
p<0.05.
Saliva sampling bioassays
Participants who completed all four salivary time samples on both evaluations (27 of 28) were included in the analyses for α-amylase (4 missing data points; HYP group: n=13; AC group: n=12) and cortisol (4 missing data points; HYP group: n=14; AC group: n=13). Complete data were used for each time point if data were complete for both pre- or postsalivary measures for the respective assay, although AUC analysis used only complete data (α-amylase: n=21; cortisol: n=23). Missing samples may be the result of nonadherence to the protocol or unusable samples. The intra-assay coefficient of variation for cortisol was between 4.0% and 6.7%, with the corresponding interassay coefficients of variation between 7.1% and 9.0%. The intra- and interassay coefficients of variation forα-amylase were 2.8%–6.3% and 5.5%–7.6%, respectively.
Salivary cortisol
Test for normality revealed a normal skewness of 0.4 and kurtosis of 1.9 with an approximately normal Q-Q plot using the Shapiro-Wilk test. Table 4 shows the deltas at each time point for pre- and postintervention. No statistically significant pre-to-post differences were observed for each group, with differences of the changes between groups (all p>0.38). Figure 2 depicts pre- to postintervention AUCs by group. Table 5 showed that no statistically significant differences were found for cortisol between groups for Wilcoxon rank-sum test (p=0.54), or when mixed modeling was used (adjusted means±standard error, 0.23±0.27; p=0.41). A small effect size was observed for the prehypertensive HYP subgroup favoring a decrease in cortisol (prehypertensive Cohen d=0.19), while a small to medium increase was seen in the AC group (Cohen d=0.25; prehypertensive Cohen d=0.47).

Awakening curves for salivary α-amylase and cortisol in the yoga (HYP) and attention control (AC) groups across four time points (bedtime [bed], upon awakening [wake], and 30 and 60 minutes after awakening) at pre- and postintervention.
Values expressed in postintervention – preintervention mean±standard deviation.
p<0.05. Significance determined using Wilcoxon rank-sum test.
Area under the curve expressed from four time points of salivary assays with area under the curve±standard deviation. Differences expressed with Wilcoxon rank-sum test and effect size (Cohen d).
Salivary α-amylase
Tests for normality resulted in a skewness of −0.1 and kurtosis of 0.8 with a Q-Q plot approximately linear and Shapiro-Wilk test indicating a normal distribution. Deltas between pre- and postintervention values at the four time points for α-amylase showed no statistically significant between or within groups differences (all p>0.21). α-Amylase showed a marked drop from pre- to postintervention in the HYP group, as shown in Figure 2. Although AUC analysis of the difference between groups (Wilcoxon W p=0.34; Table 5) and longitudinal mixed modeling (adjusted means±standard error, 0.24±0.21; p=0.28) showed no statistically significant differences between HYP and AC groups, a small to moderate effect size was seen in the HYP group favoring a reduction of α-amylase (Cohen d=0.34; prehypertensive d=0.20), while α-amylase increased in the prehypertensive AC group (prehypertensive Cohen d=0.30).
Discussion
This pilot trial is the first to study the preliminary effect of a 3-month Hatha yoga intervention on resting BP and underlying neurohormonal mechanisms of SNS and HPA axis activation in healthy nonhypertensive youth. Intention-to-treat analyses revealed a modest 3.0-mmHg reduction in resting SBP for the HYP group compared with relatively little change (−0.07 mmHg) among the AC group. Subgroup analyses involving prehypertensive participants revealed a much greater benefit of Hatha yoga upon SBP/DBP reductions (−10.75/−8.5 mmHg) compared with the AC group (1.8/1.0 mmHg). Examination of repeated saliva sampling from bedtime through 1 hour postawakening suggested that the HYP group experienced reductions in α-amylase at 60 minutes, which may have been clinically relevant to change the shape of the morning awakening curve postintervention. These findings suggest that reduced SNS activation may have partially contributed to reductions in BP.
As stated earlier, no RCT has used yoga for BP management in adolescents. 40,41 However, studies have been performed with youth using breathing awareness meditation. With regard to normotensive youth, Barnes et al. (2004) conducted a 3-month school-based RCT on breathing awareness meditation among a sample of nonhypertensive sixth graders. 50 The meditation group performed 10-minute sessions twice daily: once at school and once at home. The meditation group exhibited a 2.7-mmHg reduction in resting SBP, which mirrored the findings involving the entire Hatha yoga group.
Similar to our prehypertensive subgroup findings, Bagga and Ghandi (1983) observed that prehypertensive 17- to 20-year-old women who engaged in a 3-month yoga program exhibited a 7.3-mmHg reduction in SBP compared with no change in a control group. 43 RCTs involving adults with prehypertension or hypertension have collectively found that 2–4 months of transcendental meditation, breathing meditation, relaxation response, or yoga resulted in resting SBP changes ranging from −4.7 to −8.4 mmHg compared with little or no change among control groups. 21,51 –53 A common feature between the yoga program and many of the meditation programs involved in the above RCTs was use of various breathing techniques and exercises to help increase parasympathetic drive and counter arousal of the sympathetic nervous system. 54
The underlying neurohormonal links between yoga and its influence on BP have not been fully delineated. As stated earlier, salivary α-amylase is a biomarker of SNS activation, 55 while cortisol is a marker for HPA axis regulation. 46 Reduction in these markers infers a shift in SNS and HPA axis regulation toward parasympathetic dominance that relates to decrease BP. 11,24,45,55 In one 3-month RCT of Iyengar yoga that involved 57 prehypertensive adults and those with stage 1 hypertension, no statistically significant pre-to-post changes in urinary or salivary cortisol single sampling–based levels were noted, although a 6-mmHg decrease in 24-hour ambulatory SBP was observed in the yoga group. 31 In another study with normotensive adults using a 4-month yoga therapy program for stress reduction, resting SBP decreased from 115.5 to 113.7 mmHg (Cohen d=0.15) in the yoga group, along with a small nonsignificant increase in single sample salivary cortisol levels (Cohen d=0.56). In the same study, the cognitive-behavioral therapy group showed a slightly larger decrease in SBP (117.6 to 112.9 mmHg; Cohen d=0.41 and similar increases in cortisol levels (Cohen d=0.31). 56 The authors stated that it was difficult to interpret the results because even though both cognitive-behavioral therapy and yoga participants' cortisol levels increased, reductions in epinephrine (Cohen d=0.53) and norepinephrine (Cohen’ d=0.29) were also shown. The increases in cortisol may have been linked to seasonal fluctuations or some common chronic work stressor. Because the balance of these hormones' effect on BP is complex, the drop in SNS activity may have been more responsible for the SBP reduction. A Japanese study found a 1-month yoga program resulted in a significant reduction from pre- to postintervention in a single sampling of salivary α-amylase in young and older adults directly after a 90-minute yoga class. 57
Other yoga studies have relied on a single sampling strategy and did not use repeated samplings to capture neurohormonal variability over time that may better explain change in BP. 31,56,57 Repeated sampling of cortisol and α-amylase at bedtime and then through early awakening, termed “morning awakening curve,” has been used in various psychophysiologic stress assessments involving SNS and HPA axis function. 47,55 Using this assessment approach, we found indications of reduction in salivary α-amylase morning awakening curve. Inconsistency in changes in cortisol and SNS activity in previous yoga studies may be partially due to reliance on single sampling methods. Other methodologic issues that may account for inconsistency in findings include the type of yoga style, frequency and duration of sessions, trial durations, small sample sizes, and statistical considerations. 11,24
Several limitations must be discussed in interpreting the results of this pilot trial. The small sample size precludes assertions that the findings are definitive. This is especially true of the prehypertensive subsample comparisons, which, although underpowered, showed large differences in SBP reductions between the HYP and AC groups. These promising results require a larger, adequately powered efficacy study using prehypertensive youth to investigate effects of the HYP intervention on neurohormonal and BP responses. A second limitation was the lack of objective measurement of the intensity and duration of physical activity outside of the school environment, although each group had similar self-reported types and proportions of extracurricular sports. Accelerometry would better assess the activity levels of the students but was not possible because of budget limitations. Another limitation was the lack of information on whether yoga participants engaged in additional yoga sessions outside of the school-based sessions. Higher engagement of Hatha yoga practices may have a dose-response effect. Twenty-four-hour or overnight urine sodium excretion rates were not recorded; these data would help explain whether improved sodium handling was a potential mechanism responsible for reduced BP levels. Finally, it is unknown whether participants practiced just the breathing exercises with or without abbreviated combinations of postures outside of school for relaxation or stress-related coping strategies.
Future yoga trials would benefit from objectively monitoring the amount of yoga techniques engaged in outside of formalized sessions. Recent advances in wireless mobile health technologies can objectively monitor adherence to yoga and meditation programs by measuring heart rate and body movement patterns. 58,59 Other ecologic momentary assessment tactics (e.g., frequency, severity, and type of stress exposures; cognitive and affective state responses) can be captured by using this technology. Future yoga BP control studies would benefit from repeated 24-hour BP evaluations in conjunction with smartphone-enabled ecologic momentary assessment techniques to monitor the frequency and intensity of the participants' intrinsic and extrinsic stressor exposure, fluctuations in affective states, and use of components of yoga asanas and/or breathing techniques when feeling stressed. This information would provide greater clarity regarding the beneficial impact of yoga programs on participants' coping resources and their associations with BP control in the natural environment, as opposed to solely clinic or laboratory settings. 60,61
If yoga programs can be shown to have long-lasting sustained benefit on BP, likelihood of dissemination increases throughout various settings in addition to school systems. The relatively low costs and ease of implementation make yoga a viable option for community organizations (e.g., YMCA or health/recreation centers), or via individual delivery (e.g., gaming systems/mobile applications) at home or in other settings. Having an array of empirically validated nonpharmacologic lifestyle programs for prehypertensive youth and adults, such as yoga, tai-chi, or various meditation techniques, in addition to already validated diet and physical activity programs, will increase likelihood of their engagement and sustained use over time. 62,63
Conclusion
This study showed that a Hatha yoga program for youth produced beneficial changes in BP along with indications of reduced SNS drive, as reflected by reductions of salivary α-amylase, especially in the prehypertensive subgroup. However, these findings need to be interpreted cautiously because of the limited sample size and lack of follow-up evaluations. A large-scale efficacy RCT with prehypertensive youth is needed to comprehensively assess the underlying SNS, HPA axis, and other mechanistic pathways potentially responsible for BP control. Importantly, a larger, adequately powered study with a longer duration is needed to assess sustainability of postintervention effects.
Footnotes
Acknowledgments
This publication was supported by the South Carolina Clinical & Translational Research Institute, with an academic home at the Medical University of South Carolina, Clinical & Translational Science Award National Institutes of Health/National Center for Advancing Translational Sciences (NCATS), grant UL1RR029882. The content does not represent the official views of the National Institutes of Health or the NCATS. The authors thank Mary Davis and Kelsey Gonto for their assistance with data collection.
Author Disclosure Statement
No competing financial interest exists.