
Abstract
Background:
Few attempts have been made to evaluate the physiology of traditional Eastern health practices. The goal of this study was to evaluate the hemodynamic effects of the mysterious Buddhist practice of tumo. Tumo is a meditative practice that produces inner heat through the alleged cultivation of body energy-channels.
Methods:
This study was performed by members of an international expedition to the Himalayan Mountains in the Republic of India. The study was performed in an unpopulated outdoor mountainous area at an altitude of 16,400 ft with ambient temperatures between −10 and −15°C. Two (2) cohorts of subjects were studied: healthy non-yogi volunteers and tumo practitioners. All of the subjects were stripped down to their underclothes and exposed to the subzero atmospheric temperatures for 5 minutes. The volunteers were then passively rewarmed while the tumo practitioners performed tumo for up to 10 minutes. Blood pressure, heart rate, and stroke volume index (SVI) and cardiac index were measured noninvasively using a NICOM™ hemodynamic monitor, while carotid blood flow and biventricular performance were determined echocardiographically at each stage of the experiment. The total peripheral resistance index (TPRI), left ventricular ejection fraction (LVEF), and tricuspid annular plane systolic excursion (TAPSE) were determined using standard formula.
Results:
Fourteen (14) subjects (six volunteers and eight tumo practitioners) completed the study. There was one female subject in each group. With cold exposure, the SVI and carotid blood flow decreased while the TPRI increased significantly in both groups. In the volunteer group, these changes retuned to baseline with rewarming. Following tumo, the cardiac index (4.8±0.6 versus 4.0±0.5 l/m2; p<0.01), carotid blood flow (445±127 versus 325±100 mL/min/m2, p<0.01), LVEF (68±5 versus 64±7%; p<0.05) and TAPSE (2.9±0.4 versus 2.4±0.5 cm; p<0.01) were significantly higher when compared with baseline, while the TPRI was significantly lower (1786±189 versus 2173±281; p<0.01).
Conclusions:
Tumo was associated with a hyperdynamic vasodilated state with increased biventricular performance. We postulate that tumo results in a massive increase in sympathetic activity with activation of brown adipose tissue and marked heat production. The increased heat production may explain the paradoxical vasodilatation in tumo practitioners exposed to subzero temperatures.
Introduction
F
The authors have observed that tumo appears to consist of three steps or stages, though some techniques differ between practitioners: (1) While sitting in a cross-legged (or Lotus) position, the practitioner exhales as deeply as possible attempting to rid the lungs of as much air as he (she) can (Fig. 1). (2) Without inhaling, the anterior abdominal wall muscles are contracted and relaxed vigorously in an in-and-out or circular motion. Some, but not all practitioners will also shake the body or bounce slightly. On average, the breath is held from 1.5–2.5 minutes while the abdominal exercises are performed. (3) With the spine extended and head held somewhat back, deep inhalation is performed, at which time it is said the actual heat or sensation of warmth will occur. These steps are repeated as necessary but on an average every 3–5 minutes to keep heat generation constant.

Tumo practice.
Study Design
This study was conducted in October 2012 by members of an international expedition to the Republic of India, Himachal Pradesh province in the Himalayan Mountains. A seasoned expedition organizer (RSM) gathered tumo yoga experts, scientists, and physicians (certified in echocardiography). The study was performed at the Rohtang and Kunzum Passes (average altitude of 5000 m/16,400 ft), sites where tumo has traditionally been practiced. The subjects were studied outdoors at an isolated location at subzero temperatures (−10 to −15°C with the wind-chill factor). This study was approved by the Institutional Review Board of Saint Petersburg University (irbspsu@yandex.ru). Written informed consent was translated into all relevant languages and cross translated to assure accuracy. It was signed by all participants after all questions were answered by the scientific team.
Two cohorts were studied, namely (1) six healthy nonyogi volunteers (V) and (2) eight tumo practitioners (T). Demographic (age/sex) and anthropometric data (height, weight, body–mass index [BMI], and body surface area) were recorded on each subject. With subjects sitting in the lotus position, baseline hemodynamic data (detailed below) were obtained in all subjects (measurement No. 1). The subjects then stripped down to their underclothes, exposing themselves to the subzero atmospheric temperatures. The second set of hemodynamic data was obtained on all subjects after 5 minutes of cold exposure (measurement No. 2). The volunteers were then passively rewarmed for 10 minutes and the third hemodynamic profile was then obtained (measurement No. 3). The tumo practitioners rewarmed themselves by performing tumo with the third hemodynamic profile being obtained after about 10 minutes of tumo (measurement No. 3). The subjects were sequentially studied over a 2-day period, with each experiment lasting approximately 20–25 minutes. An outline of the research process is provided in Figure 2.
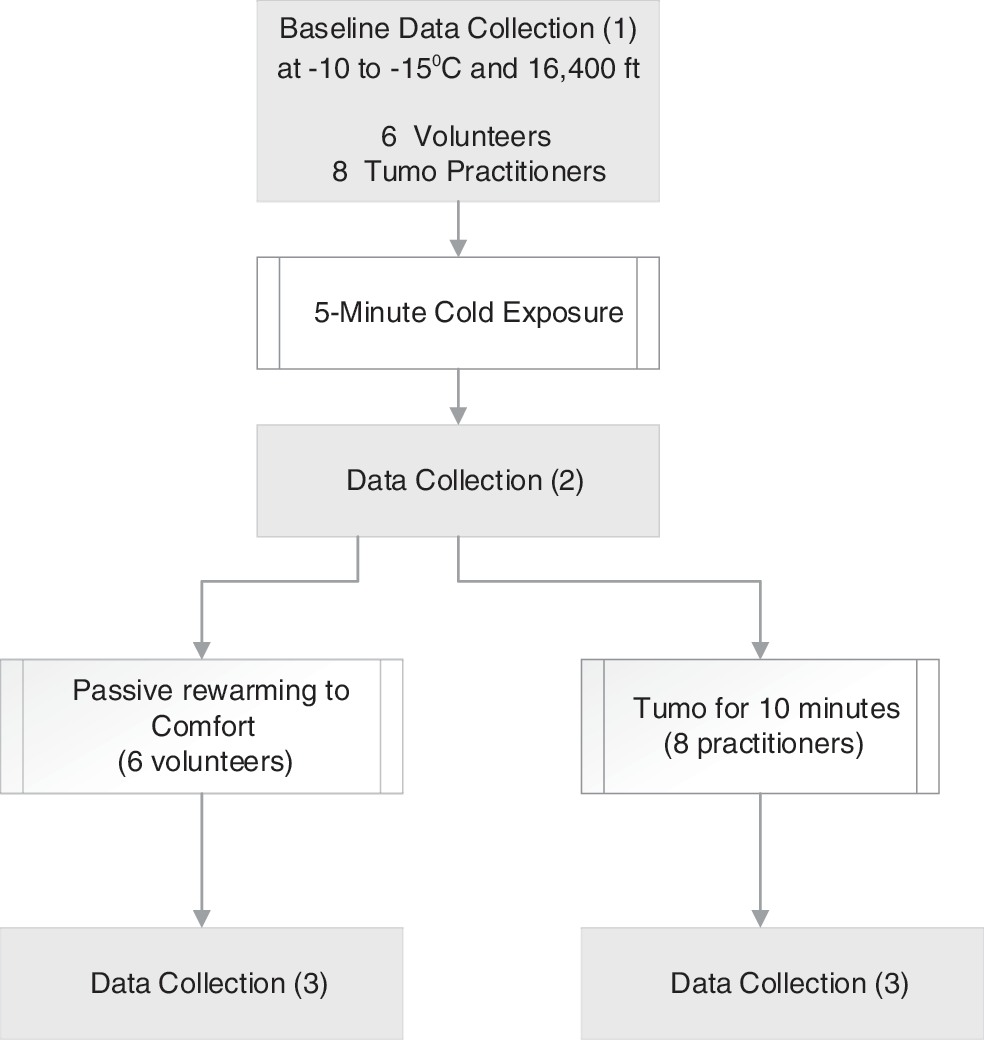
Outline of research process.
Hemodynamic measurements
Two portable ultrasound units (SonoSite Edge, SonoSite, Bothell, WA) with a phased- and linear-array transducer and a bioreactance cardiac output (CO) monitor (NICOM, Cheetah Medical, Vancouver, WA), obtained through an in-kind grant, were used to obtain the hemodynamic profile. Standard echocardiographic views (parasternal long axis, parasternal short axis, substernal, and four chamber) were obtained on all subjects at each time point. Color flow and Doppler analysis, as well as motion mode were used to obtain hemodynamic measurements at the mitral, aortic, tricuspid, and pulmonic valves. Images were saved as video clips and still images for later analysis. Waveform analysis was performed to obtain all metrics used in calculating hemodynamic function and flow. In the tumo practitioners, stroke-volume index (SVI), left ventricular ejection fraction (LVEF), and tricuspid annular plane systolic excursion (TAPSE) were determined echocardiographically at baseline (measurement No. 1) and post-tumo (measurement No. 3). The biplane Simpson's formula was used for calculation of SVI and LVEF. 3 TAPSE, a measure of right ventricular function, was measured with M-mode echocardiography. 4,5 Common carotid arterial blood flow was measured concurrently with the echocardiographic examination by a technique that has been previously described. 6 Briefly, a linear array transducer (10 MHz) was used to image the common carotid artery in long axis. Utilizing color flow, a Doppler gate was placed in the center of the vessel. The velocity time integral (VTI) was determined automatically through digitalized Doppler spectral envelopes. Vascular software allowed calculation of carotid blood flow (in milliliters per minute) from the VTI and vessel diameter (measured from intima to intima).
NICOM® bioreactance technology provides a validated, real-time, noninvasive, and simple method to dynamically measure stroke volume (SV) and CO. 7 –9 Bioreactance SV measurement is based on an analysis of the relative phase shifts of an oscillating current that is applied across the thoracic cavity. 7 The system is portable (with a battery pack) and is truly noninvasive. The system consists of a high-frequency (75 kHz) sine-wave generator and four dual-electrode “stickers” that are used to establish electrical contact with the body. Two (2) stickers are placed on the right side of the body, and two stickers are placed on the left side of the body (below the clavicle and on the lower lateral area of the chest on each side). The stickers on a given side of the body are paired, so that the currents are passed between the outer electrodes of the pair and voltages are recorded from between the inner electrodes. The system's signal-processing unit determines the relative phase shift (ΔΦ) between the input and output signals. The peak rate of change of Φ (dΦ/dtmax) is proportional to peak aortic flow during each beat, allowing calculation of the stroke volume. 10 The device records the heart rate and has an automated noninvasive blood pressure monitor, therefore allowing calculation of the following parameters: SV, SVI, CO, cardiac index (CI), mean arterial pressure, total peripheral resistance (TPR), and total peripheral resistance index (TPRI). These parameters are updated every minute and stored in the device for later review/export.
Data analysis
The subject's data were de-identified, abstracted, and recorded in an electronic spreadsheet (Excel 2010, Microsoft, Redmond, WA). Summary statistics were used to describe the clinical data, grouped by volunteers and tumo practitioners. Paired Student's t-tests were performed to compare the hemodynamic variables at baseline (measurement No. 1) with measurements No. 2 and 3 in each group. We used the Shapiro–Wilk and the Kolmogorov–Smirnov methods to test the data for normality. The correlation coefficient between the SVI measured by NICOM was compared with that measured echocardiographically. Number Crunching Statistical System 8 (NCSS8, Kaysville, UT) was used to perform the statistical analysis. Unless otherwise stated, all data are expressed as mean±standard deviation (SD), with statistical significance declared for probability values of 0.05 or less.
Results
Fourteen (14) subjects completed the study: six volunteers and 8 tumo practitioners. There was one female subject in each group. The mean age of the volunteers was 38±12 years and that of the tumo group was 38±8 years. The BMI of the volunteers and tumo practitioners were 22±3.4 and 24±3.2 kg/m2, respectively. All subjects were able to successfully complete all three stages of the experiment, with none of the subjects shivering during any stage of the study. The subjects' hemodynamic data at each time point are listed in Table 1. Both the volunteers and tumo practitioners demonstrated a significant decrease in SVI with an increase in TPRI after exposure to cold. These changes were largely reversed in the volunteers with rewarming. In the tumo practitioners, the CI, LVEF, and TAPSE increased significantly following the tumo maneuver while the TPRI decreased. The correlation coefficient between the SVI measured by NICOM with that measured echocardiographically was 0.82 (p<0.001).
p<0.05, compared to baseline.
By NICOM.
By Simpson's method.
SVI, stroke volume index; CI, cardiac index; HR, heart rate; MAP, mean arterial pressure; TPRI, total peripheral resistance index; LVEF, left ventricular ejection fraction; TAPSE, tricuspid annular plane systolic excursion.
Discussion
While environmental hypothermia is a common medical problem, the hemodynamic response to environmental hypothermia has not been studied. 11 This study made it possible to follow the hemodynamic changes associated with short-term, severe environmental cold exposure, the response to passive rewarming, and the cardiovascular physiology of tumo during extreme hypothermia. In both the volunteers and tumo practitioners, exposure to cold was associated with a significant increase in total peripheral resistance (vasoconstriction), with a significant decrease in stroke volume and cerebral blood flow. In the volunteers, these changes returned to baseline with passive rewarming. It is well known that the first response to environmental hypothermia is an increase in sympathetic tone, leading to intense arteriovenous constriction as a heat-conserving mechanism to decrease blood flow to the skin. 11 –13 The 34% increase in TPRI recorded in the volunteer group is in agreement with this concept, and validates the technology used in this study. It is noteworthy that the heart rates remained unchanged while the SVI decreased, resulting in a decrease in cardiac index. The decrease in stroke volume may be consequent to the increased ventricular afterload due to intense vasoconstriction. The fall in cardiac index may be somewhat offset by the increase in basal metabolic rate and oxygen consumption associated with hypothermia. 14 There was a smaller increase in TPRI in the tumo group with cold exposure (21%); this may represent some degree of adaptation to hypothermia. Most studies that have investigated the cardiovascular effects of induced hypothermia have been performed following cardiac arrest, where the underlying cardiac disease confounds the hemodynamic picture. 15 However, this study's findings are similar to those reported by He and colleagues, who demonstrated in an ovine mild-hypothermia model that hypothermia was associated with an increase in TPRI and a decrease in SVI, which was reversed with rewarming. 16 It is noteworthy that in the present study, cerebral blood flow decreased by 26% in the volunteers and by 17% in the tumo group. It has previously been reported that cerebral metabolism is depressed 6%–7% per 1°C decrease in core temperature. 12,17,18 It is likely that preserved metabolic coupling with cerebrovascular reactivity accounts for the decrease in cerebral blood flow. 19 These findings are in contrast to experimental studies, which have demonstrated that cooling leads to dilatation of the carotid artery with an increase in cerebral blood flow, while hyperthermia causes cerebral vasoconstriction with a decrease in cerebral blood flow. 20
A single previous study (published in 1985) was identified that investigated the physiologic changes with tumo. 2 Benson and colleagues studied the changes in central and peripheral body temperature in two tumo practitioners. This study was conducted in unheated, uninsulated stone huts in the foothills of the Himalayan Mountains. While the rectal temperature of the tumo practitioners remained constant, finger and toe temperature increased by up to 7.2°C. It was postulated that the increase in peripheral skin temperate was due to vasodilation and increased cutaneous blood flow. Remarkably, the air temperature within the hut increased by up to 3.2°C. It is our supposition that the increased hut temperature can only be explained by the exhalation of warm air by the tumo practitioners.
The hemodynamic changes that were noted with tumo were quite remarkable and remain somewhat unexplained. Despite being exposed to subzero temperatures, the tumo practitioners were able to vasodilate and increase their CO with a marked increase in cerebral blood flow. As the core (and brain) temperature remains unchanged during tumo, 2 and presuming cerebral autoregulation is intact, this would suggest that the increased cerebral blood flow is a consequence of increased brain activity and metabolic demands. In experimental animal models, increased brain activity is associated with intrabrain heat production and increased cerebral blood flow. 21 Furthermore, using single-photon emission computed tomography, Newberg et al. demonstrated an increase in cerebral blood flow in Tibetan Buddhists during meditation. 22 In order to explain the physiologic changes associated with tumo, basal metabolic rate and oxygen consumption must increase dramatically to account for the increased heat production. It is postulated that tumo results in a massive increase in sympathic tone with increased adaptive thermogenesis in brown adipose tissue and skeletal muscle. Mitochondrial uncoupling, the process whereby substrate oxidation is uncoupled from ATP production, results in heat production and is responsible for adaptive thermogenesis. 23 –26 Unlike white adipose tissue, which acts predominantly as an energy storage depot, brown adipose tissue is a thermogenic organ dissipating energy in the form of heat. 23,26 Brown adipose tissue and skeletal muscle are rich in mitochondria, which contain uncoupling protein-1 (UCP-1), which is responsible for adaptive thermogenesis. 23 –26 In addition, cold adaptation results in an increase in the size of the brown adipose tissue depots. 27 β-adrenergic activation of brown adipose tissue increases the availability of fatty acids for oxidative metabolism and increases UCP-1 activity. 26 The authors postulate that tumo increases sympathetic activity with increased expression and activation of UCP-1 with uncoupling of fatty acid oxidation in brown adipose tissue and skeletal muscle. It is noteworthy that after performing tumo, practitioners eat large volumes of clarified yak buttermilk ghee alone or with barley flower (tsampa), presumably to restore their brown fat stores. Remarkably, ghee is thought to be sacred to Agni (as in Agni-Sara), the Hindu god of fire.
Conclusions
Exposure to extreme cold resulted in peripheral vasoconstriction and a decrease in CO, effects that serve to limit heat loss. Tumo performed in the same environmental conditions resulted in an increase in CO with vasodilatation. Further research of the tumo phenomenon could provide insight into the mind–body connection and its effects on physiologic functions. In addition, tumo-induced thermogenesis could potentially have a role in weight-loss programs.
Footnotes
Acknowledgments
We acknowledge the efforts and echocardiographic skills of Alex Levitov, MD, without whose help this project would not have been possible. We thank I.V. Arkhipova, the director of the Faraon studio of historical films and the organizer of international research expeditions to the Himalayas, carried out through the project “V poiskakh utrachennykh znanii” (In Search for Lost Knowledge). We acknowledge SonoSite (Fujifilm) Corporation and Cheetah Medical for the equipment support of the study.
Author Contributions
RSM was the principal investigator for this study. RSM designed the study. RSM, ARB, and RRB were responsible for the recruitment of subjects and execution of the study. DPB provided technical assistance and performed the echocardiography and carotid Doppler studies. PEM and RSM interpreted and analyzed the data. PEM wrote the first draft of the manuscript. All authors helped to critically revise the draft and approved the final version of the report.
Author Disclosure Statement
No competing financial interests exist.