
Abstract
Background:
Caring for a person with dementia can be an unrelenting and burdensome task, one that is often detrimental to the caregiver's health, well-being, and functionality. The enduring stress and frustration of the caregiver role can also contribute to poorer outcomes for dementia sufferers. Building on growing clinical interest in the capacity for Transcendental Meditation® (TM; a relaxation technique) to reduce stress and anxiety in healthy workers, this study examines whether similar improvements could be experienced by dementia caregivers.
Objective:
The study objective was to ascertain whether a TM program can improve psychological stress, quality of life, affect, and cognitive performance of dementia caregivers.
Design:
The study was a pilot prospective, single-center, randomized wait-list controlled trial with two parallel arms.
Setting/subjects:
Community-dwelling carers of persons with diagnosed dementia, residing in metropolitan Adelaide, South Australia, were included in this study.
Interventions:
Participants will be randomly assigned to a 13-hour TM training program or wait-list control over 12 weeks.
Outcomes:
Primary outcomes include quality of life and stress. Secondary outcomes include affect, cognitive performance, cost-effectiveness, and study feasibility. Outcomes will be assessed at baseline, week 12 (postintervention), and week 24 (follow-up).
Results:
Results are expected to be available early in 2014.
Conclusions:
This project responds to a need for robust evidence of the clinical and economic effectiveness of TM for the management of caregiver stress. If Transcendental Meditation is shown to be effective, it could indicate a simple, cost-effective, and easily implemented strategy to assist many of the growing numbers of caregivers to cope with the demanding and often difficult caregiver role.
Introduction
D
The burden on the health system in terms of financial and human resources is also considerable, with direct and indirect health care expenditure on dementia in Australia in 2002 estimated at AU$6.6 billion. 3 Assuming the same cost of AU$40,519 per person with dementia, and the estimated prevalence of dementia reported in 2011 (i.e., 266,000 Australians), 2 the total cost of dementia care in Australia in 2011 is predicted to be closer to AU$10.8 billion. The cost of care provided by family carers, who deliver a large proportion of dementia care in Australia, accounts for a third ($3.4 billion) of this estimate.
The impact of dementia on family caregivers is substantial. In financial terms, carers may experience loss of earnings, either from reduced working hours or relinquished employment. 4 Carers of people with dementia also report high levels of stress, sleep disturbance, depression, anxiety, social isolation, comorbid illness and impaired cognitive performance, as well as reduced quality of life. 5 –8 Studies also indicate a sixfold increased risk of dementia in community-dwelling carers of dementia sufferers when compared to noncaregivers. 9 The enduring stress and frustration of caring for a person with dementia, or caregiver burden, is also associated with poor outcomes for dementia sufferers, including decreased quality of life, reduced functional and psychological status, and early nursing home placement 7,10,11 ; all of this contributes to further distress in the carer. 7 The need to improve the emotional, psychological, and physical well-being of carers thus has important health, social, and economic implications.
Some complementary therapies, specifically relaxation therapies, have demonstrated promising effects in the management of conditions either induced or exacerbated by stress, including anxiety, 12 migraine, 13 and irritable bowel syndrome. 14 This suggests that these therapies may help to reduce caregiver burden. Many of these therapies may work by inducing the relaxation response. Smith's Attentional Behavioural Cognitive relaxation theory proposes that all approaches to relaxation have the potential to evoke one or more of 15 factor-analytically derived relaxation states, or “R-States,” such as physical relaxation, awareness, and feeling energized. 15
One form of relaxation therapy that demonstrates promise as a treatment for stress is Transcendental Meditation® (TM). This therapy, which originated in India in the 1950s, is a form of concentrative meditation that allows an individual's attention to travel naturally to a less active, quieter style of mental functioning, to produce a unique psychophysiological state of restful alertness. 16 Unlike many other forms of relaxation, TM is highly standardized, relatively effortless, easily learned, convenient (i.e., can be practiced anywhere and anytime), and without ongoing cost to the user 16 ; TM has also been shown to produce larger effects in patients with anxiety when compared to other relaxation techniques. 16 These features make TM a suitable and accessible relaxation technique for busy caregivers.
Although there have been no studies to date examining the effects of TM on any outcome in carers, evidence from a small US pilot study of 31 dementia caregivers suggests that another form of relaxation therapy, mindfulness meditation, may be more effective than respite in reducing carer stress. 17 In view of these findings, and the results of an earlier randomized controlled trial showing TM to be comparable with other kinds of relaxation therapies in reducing anxiety in patients diagnosed with anxiety neurosis, 18 it is plausible that TM also may be beneficial in attenuating stress and anxiety in dementia caregivers. This is, in part, supported by evidence from controlled trials examining the effects of TM in workers. 19,20
Given the implications of stress on carers, their family, and the wider community, and the favorable effects of TM on stressful symptoms, while bearing in mind the paucity of trials on TM and stress, the high risk of bias of these studies, and the absence of data on the effects of TM in caregivers, further research in this area is well justified.
This project responds to a need for robust evidence of the clinical and economic effectiveness of TM for the management of caregiver stress. In doing so, the proposed study will address the criticisms of previous TM trials, including (1) using outcome measures with established validity and reliability, (2) ensuring the study design and the reporting of study methods and findings meet the minimum requirements set out in the Consolidated Standards of Reporting Trials (CONSORT) statement, (3) avoiding comparing the effectiveness of TM with other forms of relaxation therapy, and (4) ensuring the study is registered on a clinical trial register, and the study protocol is published in the public domain.
Methods
Study design
The Transcendental Meditation for carers of dementia sufferers trial (TRANSCENDENT) is a pilot prospective, single-center, randomized wait-list controlled trial (RCT) with two parallel arms. This design will control against major sources of bias and attempt to discredit any alternative causal explanation; this will provide a sound basis for evaluating the effectiveness of Transcendental Meditation®, and for determining the feasibility of conducting a larger trial in this area. While participant blinding is not possible in this trial due to the nature of the intervention, staff involved in data collection, data entry, and data analysis will be blinded to treatment assignment.
Objectives
TRANSCENDENT is designed to address the following objectives:
Primary objectives
1. Establish whether TM improves health-related quality of life in community-dwelling carers of dementia sufferers when compared to wait-list control (WLC).
2. Ascertain whether TM reduces psychological stress in community-dwelling carers of dementia sufferers when compared to WLC.
Secondary objectives
1. Determine whether TM improves affect in community-dwelling carers of dementia sufferers relative to WLC.
2. Ascertain whether TM improves cognitive performance in community-dwelling carers of dementia sufferers when compared to WLC.
3. Determine whether TM is cost-effective in improving health-related quality of life in community-dwelling carers of dementia sufferers relative to WLC.
4. Determine the feasibility of implementing the project as a larger RCT.
Participants
Individuals meeting the following selection criteria will be eligible to participate in TRANSCENDENT.
Inclusion criteria
The inclusion criteria were as follows: (1) Nonprofessional, community-dwelling carer of a person with diagnosed dementia; (2) Not received previous instruction on the TM technique; (3) Able to provide written consent; (4) Able to speak, read, and understand English; and (5) Available and willing to complete all intervention sessions and assessments.
Exclusion criteria
The exclusion criteria were as follows: (1) History of any condition causing moderate-to-severe cognitive impairment; (2) Commenced or ceased psychotropic medication within the past 6 weeks; (3) Participated in a clinical trial within the past 30 days, where psychological outcomes and quality of life were outcomes of interest; (4) Practices some form of mind–body therapy on a regular basis (i.e., at least once a month); (5) Consults a psychologist/psychiatrist at least once a week; and (6) Taken a recreational drug in the past 15 days.
Sample size
The sample size was based on an expected mean difference in quality of life (AQoL) of 0.1 utility points between the TM and WLC groups. Assuming a standard deviation of 12.5% and 10% attrition, a sample size of 18 patients will be required in each arm. A total of 36 participants will have 80% power for a two-way repeated-measures analysis of variance (RM-ANOVA) to detect a statistically significant difference in quality of life with a two-tailed αlevel set at 0.05. This sample will be sufficient to test the feasibility of the study, and to generate the necessary data to estimate the sample size for a larger clinical trial.
Setting
TRANSCENDENT will be administered by the University of South Australia, and implemented through the positive aging center (Woodside, South Australia), and the Maharishi Invincibility Centre (Parkside, South Australia).
Recruitment
Nonprofessional, community-dwelling carers will be informed of the study through notices mailed to them by the Adelaide Hills Council and multiple carer respite agencies throughout Central Adelaide. In addition, study flyers will be posted on the noticeboards of community health centers, Adelaide Hills Council offices, and general practices within the Adelaide Hills Council and Central Adelaide area. A media release will also be disseminated to local newspapers, radio stations, and television networks. Carers expressing interest in participating in the project will be asked to contact the research assistant (by phone) for further information and screening. Carers eligible to participate in the study will be posted/e-mailed a copy of the participant information sheet and consent form to read and discuss with family/friends in order to make an informed decision. One week after dispatching the study information, participants will be contacted by phone to gauge their “capacity to give consent” (i.e., the ability to provide a brief description of the study purpose, and outline what their involvement in the study might entail). Participants able to provide a satisfactory response to these questions will be invited to sign the written consent form and return it to the research assistant using the attached reply-paid envelope. Participant recruitment is expected to commence in April 2013 and be completed by May 2013. The planned end date for the trial is December 2013.
Randomization
Enrolled participants will be randomly assigned to TM or WLC at a ratio of 1:1 (Fig. 1). To approximate equality of sample sizes in each study group, block randomization will be used with computer-generated randomly permuted blocks of four; this will be performed prior to participant recruitment, and by a researcher not involved in the implementation of treatment assignment. Randomization codes will be held in sequentially numbered opaque sealed envelopes. Each envelope will be selected by the research assistant (who will be unaware of the allocation sequence) in consecutive order at the time of participant enrolment.
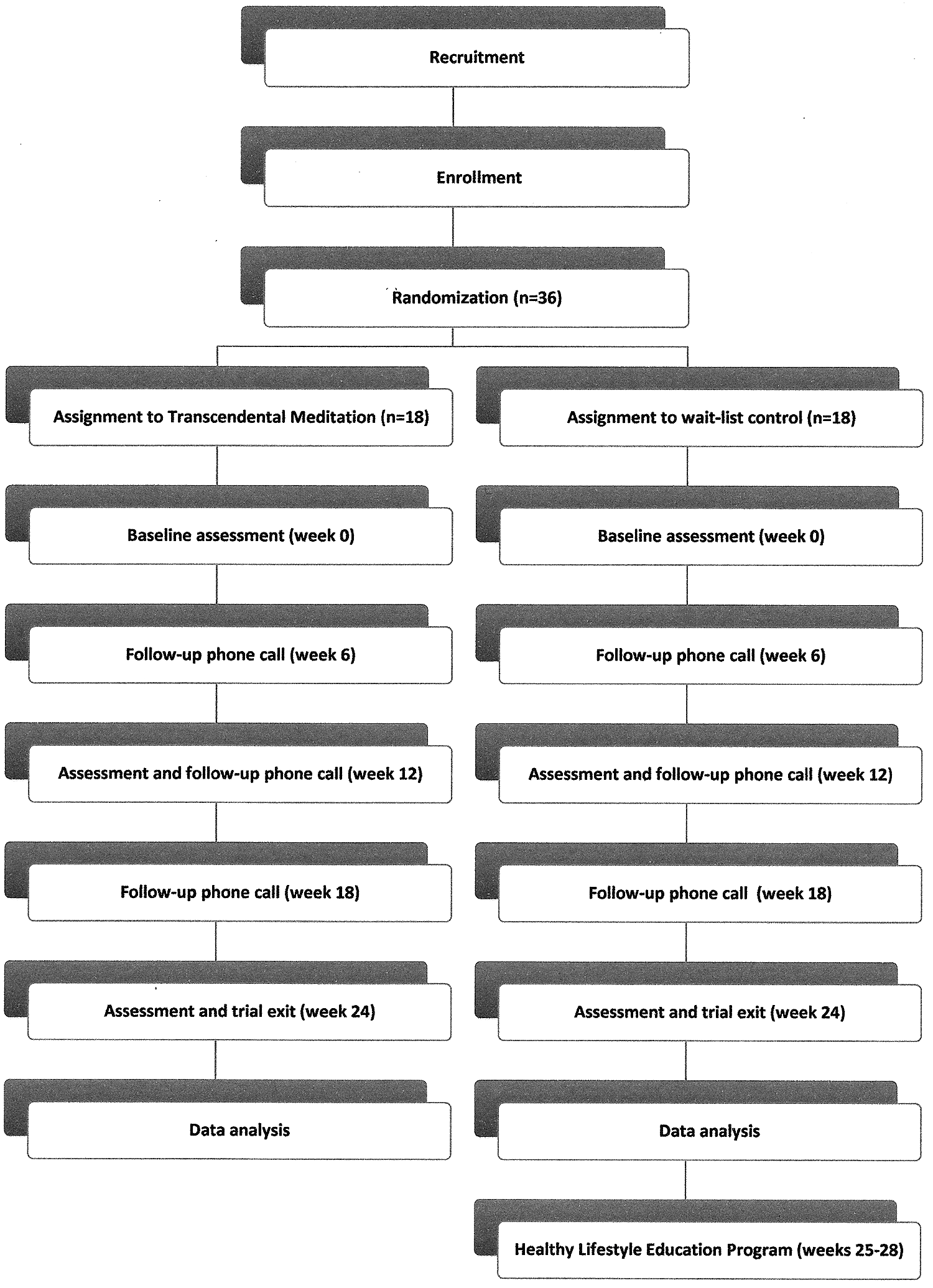
Flowchart of Transcendental Meditation for carers of dementia sufferers trial (TRANSCENDENT).
Outcomes
The primary and secondary endpoints of TRANSCENDENT are conceptualized and operationally defined as follows:
Primary outcomes
Health-related quality of life (HR-QoL) refers to an individual's sense of well-being and an ability to enjoy normal life activities. Given that carers of persons with dementia demonstrate a significant decline in quality of life, 5,6 it is important to recognize the participant's perception of change in response to each treatment in order to capture any patient-centered benefits resulting from each intervention. HR-QoL index scores will be measured using the Assessment of Quality of Life 8-dimension (AQoL-8D) instrument. This instrument, which takes less than 10 minutes to complete, will be self-administered by participants at baseline (week 0), postintervention (week 12), and follow-up (week 24).
Stress is a physiological and psychological response to an intrinsic or extrinsic event or situation. Carers of people with dementia report high levels of stress, 5,6 which can contribute toward impairments in cognitive performance, sleep disturbance, depression, and other comorbidities. 4 –6 Caregiver stress can also contribute to poor outcomes in dementia sufferers. 10,11,21 Stress is a particularly important outcome as it has notable consequences for the health and well-being of the carer, as well as those under their care. Mean stress score will be measured using the WebNeuro test battery (a self-administered, validated, neurocognitive assessment measure). The test battery will take participants between 50 and 60 minutes to complete, and will be performed at baseline, postintervention, and follow-up.
Secondary outcomes
Affect is the expression of feelings or emotions. A number of systematic reviews report a higher prevalence of affective disorders (such as depression and anxiety) in dementia caregivers when compared with noncaregivers. 7 This is likely to impact on the caregivers' capacity to self-care and to care for the person with dementia. Affect, specifically (1) emotional resilience, (2) feelings of depression, and (3) feelings of anxiety, will be measured using the WebNeuro test battery.
Cognitive performance is the ability to process information, apply previously acquired knowledge, build understanding, and initiate responses. Carers of people with dementia report high levels of stress, 5,6 and stress has been shown to impair cognitive performance. 4 Importantly, reduced cognitive performance in caregivers predicts poor physical function and ability to care. 8 Cognitive performance, specifically (1) psychomotor response speed, (2) impulsivity, (3) attention and concentration, (4) information processing efficiency, (5) working memory, and (6) executive function, will be measured using the WebNeuro test battery.
Cost-effectiveness will be determined using cost-utility analysis; this will examine the cost and effectiveness of each intervention using the quality-adjusted life year (QALY) as its unit of effectiveness. The AQoL-8D will be used to derive quality-of-life utility scores and to measure any change over the trial period. Results for each group will be compared to identify any differential change in quality of life that can be multiplied by time to generate quality-adjusted life year (QALY) gain or loss for each intervention group. The cost of each intervention will be derived from trial cost data. This will be combined with QALYs to estimate cost per QALY gain, with the assumption that TM is more expensive than WLC but delivers greater quality of life. This outcome will be assessed on completion of the study.
Feasibility, in the context of this study, refers to the ease and practicality of reproducing the study on a larger scale, that is, as a larger randomized controlled trial. Feasibility will be determined by (1) measuring rates of participant recruitment, retention, and response, (2) reporting the efficiency of each recruitment strategy, (3) recording participant experiences of the study (via the trial exit survey) and semi-structured participant interviews, and (4) evaluating the logistics of the trial methodology and procedures. This outcome will be assessed on completion of the study.
Interventions
Participants will be randomly assigned to one of two groups: TM or WLC. The 12-week (13-hour) TM training program comprises a 1-hour introductory session, 30-minute personal instruction, three 1.5-hour training sessions (over the first week), followed by three weekly 1-hour classes and four 2-weekly 1-hour classes, under the guidance of experienced TM instructors. The initial sessions will comprise content on the health effects of stress, the theory of TM, training of the TM technique, and assessment and refining of the technique. The weekly and 2-weekly sessions will focus on assessing, refining, and mastering the TM technique.
Participants assigned to wait-list control will receive 24 weeks of no intervention, followed by a 4-week healthy lifestyle education (HLE) program. (Due to resource constraints, it is not feasible to offer TM to the WLC group; hence, participant information will clearly identify HLE as the comparative intervention). The wait-list arm is a critical component of the study design as it will control for nonspecific effects and bias. The HLE program comprises 4 weekly 90-minute sessions. These sessions will be facilitated by an experienced TM instructor. Sessions will focus on developing skills and knowledge that foster a healthy diet and lifestyle, including yoga, preparation of healthy meals, and stress management. All treatment and control sessions will be delivered face-to-face, in groups, during business hours at the positive aging center (Woodside, South Australia) and the Maharishi Invincibility Centre (Parkside, South Australia). Subjects in both groups also will be contacted by telephone every 6 weeks to monitor retention and participant experience.
Statistical analysis
Data from all completed outcome measures will be entered onto SPSS (v. 20), and analyzed by intention-to-treat. Measures of central tendency and variability will be used for descriptive data where values are normally distributed. Medians and the interquartile range will be used to describe data that are not normally distributed. For categorical variables, frequency distributions and percentages will be used to describe categorical data. Differences between the two groups at baseline will be examined using the t-test for independent groups. Outcome differences between groups, differences over time, and any differential treatment effect at different points in time will be examined using RM-ANOVA. RM-ANOVA was specifically chosen because outcomes will be assessed at three different points in time. The cost-effectiveness of each treatment will be determined using cost-utility analysis (as previously described). The primary outcome of the cost-utility analysis will be the incremental cost-effectiveness ratio; this is the difference in the expected costs of each intervention, divided by the difference in expected QALYs between each intervention.
Results
Data collection is expected to commence in April 2013. Results are anticipated for early 2014.
Discussion
Caregivers are often referred to as the silent victims of dementia. Not only can the enduring stress and burden of the caregiver role take its toll on the carer financially, but also socially, physically, and mentally. Each of these corollaries, which are potentially preventable, can further distress the caregiver and person with dementia, and further encumber the community and health care system. This suggests that there are potentially considerable health, social, and economic implications for reducing caregiver stress and burden.
We hypothesize that TM will safely and effectively reduce caregiver stress and burden, and in so doing, bring about immediate improvements in the quality of life, cognitive performance, and affect of dementia caregivers. The potential downstream effects of this are numerous, including an increased capacity for caregivers to care for the person with dementia and engage in paid employment; delays in the placement of dementia sufferers into nursing homes; and reduced caregiver demand for health services.
While there is an initial cost of TM training, there are no ongoing costs to the user in maintaining this therapy. This, together with the potential benefits of TM alluded to previously, suggest that considerable health care costs attributed to caregiver stress could be averted through effective caregiver training in TM.
Conclusions
Caring for a person with dementia can be a relentless and onerous task, one that is often detrimental to the caregiver's health and well-being. With more than 24.3 million people across the globe suffering from dementia, and numbers forecast to increase as the population ages, any initiatives that contribute to caregiver health and well-being are important and valuable. If this research demonstrates that TM is effective, it could indicate a simple, cost-effective, and easily implemented strategy (that could complement and perhaps reduce the need for other forms of intervention) to assist many of the growing numbers of caregivers to cope with the demanding and often difficult caregiver role.
Footnotes
Acknowledgment
The conduct of this trial would not be possible without the tremendous support provided by Vladimir Lorenzon and Heather Lorenzon (Maharishi Invincibility Centre, Parkside), Dr. Richard Clarke (Brain Health Clinics, Adelaide) and the Adelaide Hills Council (particularly Ann Jackson, Anne Ellis, and Rebecca Shepherd). TRANSCENDENT is primarily funded by an Alzheimer's Australia Dementia Research Foundation grant, with additional funding provided by the West Torrens City Council and the School of Nursing & Midwifery, University of South Australia.
Ethics approval for the conduct of this trial was granted by the Human Research Ethics Committee of the University of South Australia.
Disclosure Statement
No competing financial interests exist.