
Abstract
Objective:
To investigate the effects of Thai traditional massage (TTM) on pressure pain threshold (PPT) and headache intensity in patients with chronic tension-type and migraine headaches.
Design:
Randomized controlled trial of TTM compared with the sham ultrasound (nine sessions each) during a 3-week period.
Participants:
Seventy-two participants who had had a headache diagnosis for at least 3 months before the experiment was recruited.
Results:
After the treatment and at 3 and 9 weeks of follow-up, the TTM group showed a significant increase in PPT (p<0.01) compared with the sham ultrasound group. PPT values at baseline, after 3 weeks of treatment, and at 3- and 9-week follow-up for the TTM group were 2.71±1.22, 3.57±1.41, 3.72±1.46, and 3.42±1.46 pounds/cm2, respectively; values in the sham ultrasound group were 2.85±1.20, 2.62±1.07, 2.58±1.05 and 2.63±0.94 pounds/cm2. In both groups, headache intensity decreased significantly (p<0.05) at every end point of the outcome measures, and there were no differences between the groups (p>0.05).
Conclusions:
TTM could increase PPT and reduce headache intensity, suggesting that this is a possible alternative treatment for chronic headaches.
Introduction
C
Treatments for CTTH and migraines can be divided into pharmacologic and nonpharmacologic. Pharmacologic treatments are most commonly used for chronic headaches. Many patients with these headaches tend to increase the dose of analgesic drugs, which may lead to an increased headache frequency. Overuse of these medications can lead to chronic headaches. Therefore, reduction of the frequency of analgesic drugs is a very important guideline for prevention of chronic headaches. 5 On the other hand, nonpharmacologic treatments for CTTH and migraines, including acupuncture, physical training, and relaxation training, can decrease the excitability of the neurons and desensitize the central pain receptors in the central nervous system and lead to a decreased pain sensitivity or an increased pain threshold. 6 Because having a prevention strategy of CTTH and migraines is encouraged, many patients have been seeking nonpharmacologic treatments and alternative therapies.
Massage is one of these nonpharmacologic treatments and the most commonly used in alternative therapy, with relatively minor adverse effects. 7,8 Walach and colleagues reported the effects of classic massage in patients with chronic headaches. 9 Recently, Thai traditional massage (TTM) showed analgesic effects in patients with back pain. 10,11 TTM is a form of deep massage with brief sustained pressure (5–10 seconds per point) in specific myofascial trigger points (MTrPs) and in a surrounding area of these points in the whole muscle. Thus, it is more likely to provide better results in overall relaxation of the patient compared with other forms of deep massage, which focus only on the trigger point. The benefits of TTM are also known to reduce salivary pain substances, 12 increase blood circulation, decrease heart rate, reduce pain, improve the efficacy of breathing, and promote relaxation. 13 One study showed that one session of massage can reduce headaches and improve other physiologic parameters. 14 No study, however, has investigated the short-term treatment and post-treatment effects of TTM on headache in head, neck, and shoulder regions by using subjective and objective measurement techniques: the pressure pain threshold (PPT) and headache intensity (as measured on a visual analogue scale [VAS]). PPT using pressure algometry is the objective measurement technique of pain and shows high levels of reliability. 15,16 To determine the effects of TTM on headaches, trials with strong methods, including appropriate sample sizes and evaluation of the long-term effects, are needed. Therefore, the current study aimed to investigate the therapeutic effectiveness of TTM on PPT and headache intensity after 3 weeks of treatment and subsequent follow-up at 3 and 9 weeks after treatment among patients with CTTH and migraines.
Materials and Methods
Study design
This 3-month prospective, parallel-group, randomized, controlled clinical trial was conducted cooperatively by a research group that consisted of physical therapists, a traditional Thai massage therapist, a neurologist, and a research methodologist/statistician. The Ethics Committee of Khon Kaen University approved the research protocol. Written informed consent was obtained from all participants at the start of the study. This study was conducted in the Division of Physical Therapy, Faculty of Associated Medical Sciences, Khon Kaen University, Thailand. Patients who met the inclusion criteria were randomly allocated to the treatment (TTM) or sham ultrasound (US; control) group, using stratified block randomized allocation with block sizes of 2, 4, and 6. The age group (group 1, age 20–35 years; group 2, age 36–50 years) and type of headache (CTTH or migraines) were also chosen as the stratification variables to achieve an approximate balance of age and type of headache. A pregenerated random assignment scheme was done by using Stata software, version 10.0 (Stata Corp., College Station, Texas). Assignments were enclosed in envelopes by a research assistant who was not involved in treatment and outcome assessment. Figure 1 summarizes patient recruitment, participation, attrition, and reasons for exclusion from the study.
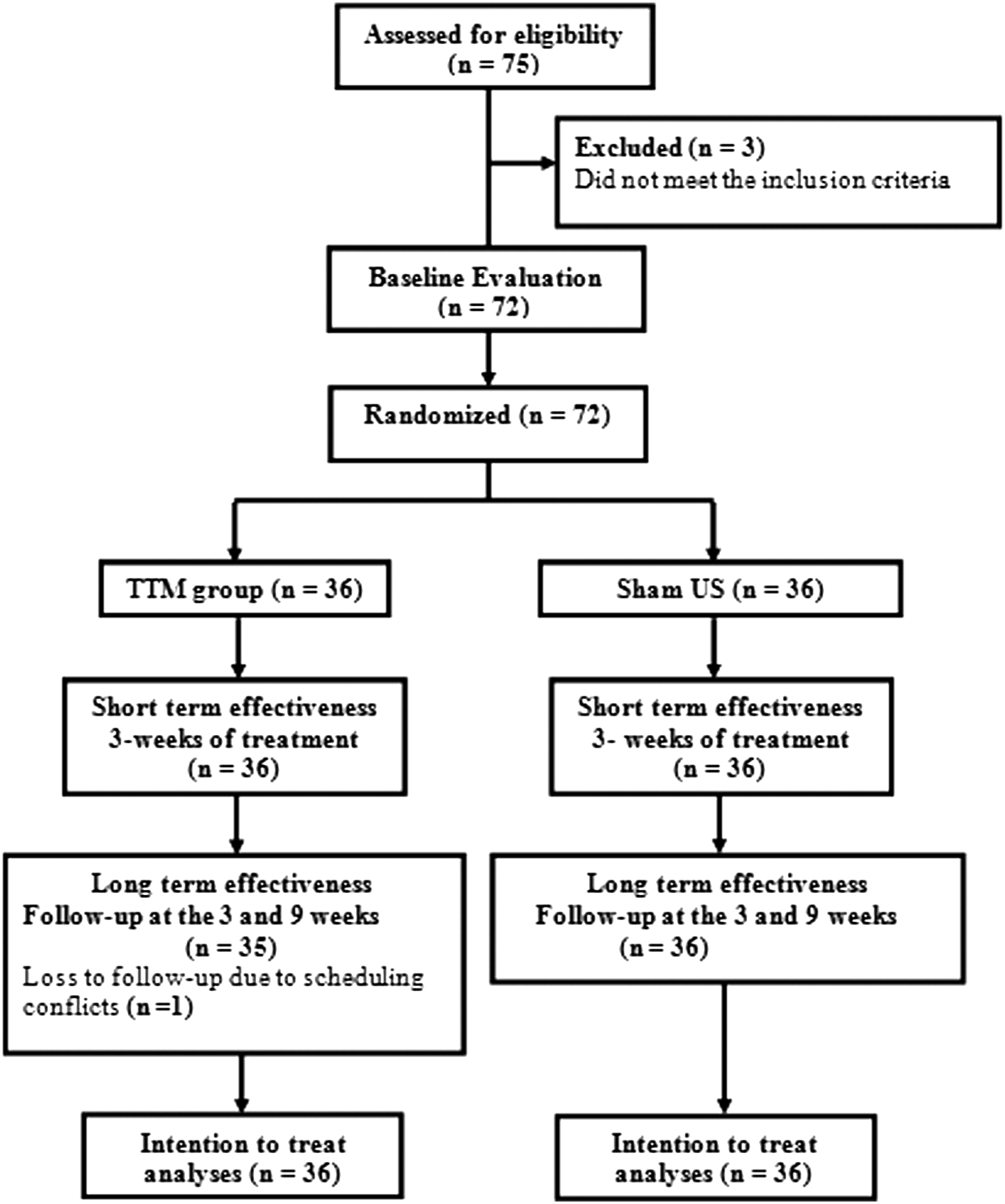
Number of participants throughout the study and reasons for dropout. TTM, Thai traditional massage; US, Sham ultrasound.
Participants
Participants with CTTH and migraines were recruited from the general community using bulletin boards and verbal requests for participants who lived in Khon Kaen during a 12-week period. Potential participants age 20–50 years were recruited. Participants who responded to the announcements were interviewed on subjective examination criteria by the first physical therapist. They underwent physical examination and were diagnosed by the neurologist.
Patients with CTTH or migraine were diagnosed according to the criteria of the International Headache Society. 17 The additional following criteria were also included: having a headache diagnosis for at least 3 months before study, having headaches present for 15 days/month at a frequency of at least two times/week, and having a score for headache intensity on a VAS of 4 or greater.
Patients with any of the following conditions were excluded: headache caused by cervical disorders, such as cervical spondylosis; spondylolysis; spondylolisthesis; or herniated disc with neurologic deficits. Other exclusion criteria were skin disease; hemiplegia/paresis; hypertension (blood pressure >170/90 mmHg); taking an antiplatelet drugs, such as aspirin, clopidogrel, prasugrel, ticlopidine, or cilostazol; inability to follow instructions; poor communication skills; and receipt of massage therapy in the last 1 month.
Treatment protocol
TTM group
The protocol in this study combined massage for 25 minutes and stretching for 5 minutes according to the pattern of royal Thai massage. The massage points included in this method are three lines on the head, upper neck, and upper back (Fig. 2). The line of massage was that followed by Sen sib, that is, the meridian line according to the TTM theory (along the lines of In-ta, Ping ka-la, and Gan-la-ta-ree), 18 which covered the muscle area of the temporalis, suboccipitals, posterior neck extensor group, upper trapezius, and levator scapulae. The massage was performed while the participants were in the supine and side lying positions. For the thumb pressing used in TTM, the massage therapist applied gentle and gradually increasing pressure along the meridian lines. Each thumb pressure was applied until the participant started to feel some pressure discomfort (subpain threshold) and was held for 5–10 seconds at each massage point. This sequence was repeated three to five times for each meridian line. 10 Passive stretching was applied thereafter. 19 The TTM recipients were treated by a massage therapist who had 5 years of experience in TTM. This massage therapist was validated on the massage technique at least 2 months before the study by a licensed physical therapist with 20 years of experience in TTM.
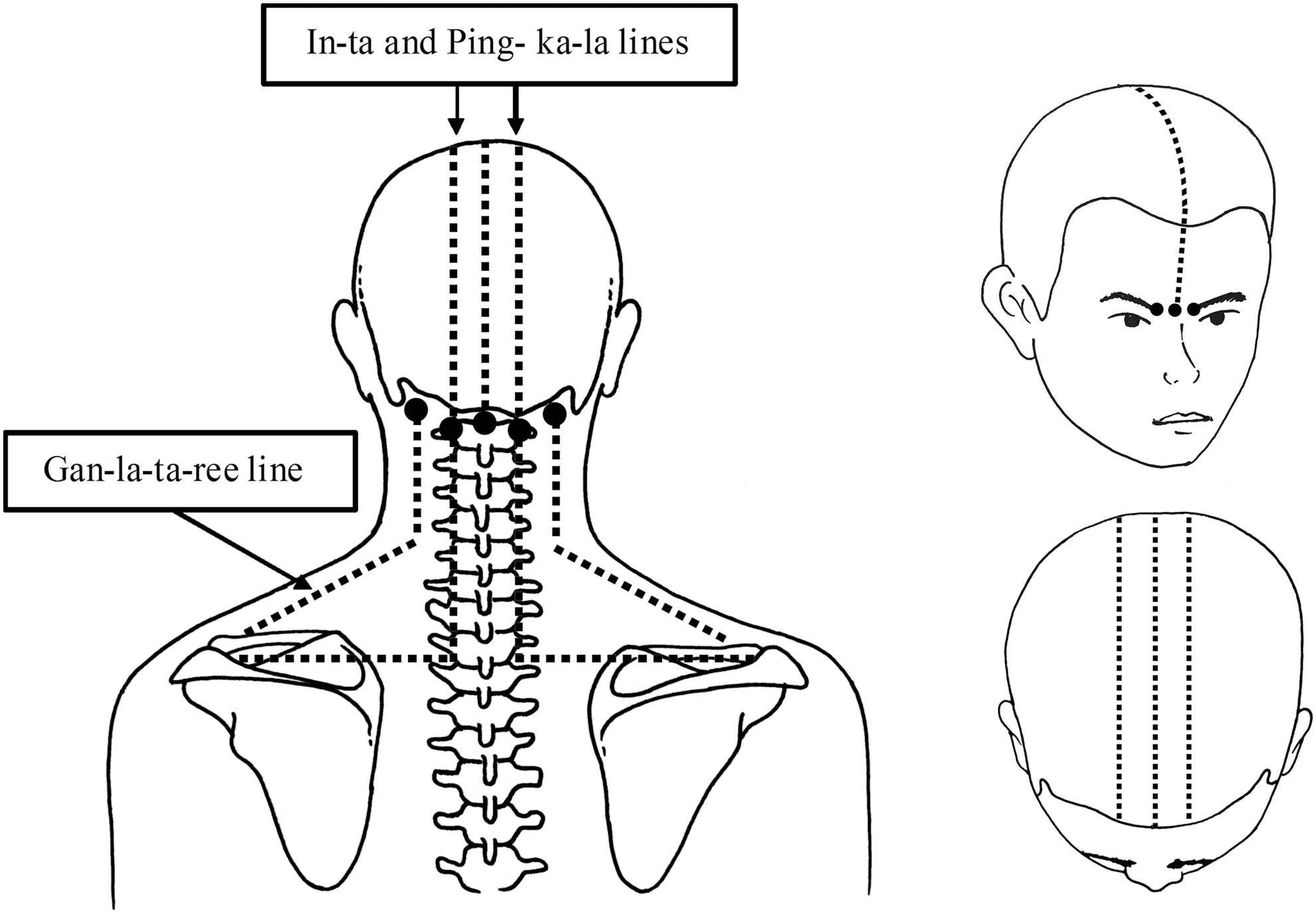
Massage points and lines for Thai traditional massage.
Sham US group
The participants in the control group received sham US application of a detuned US device with circular kneading on the upper neck or upper back in the supine and side-lying positions by the physical therapist. This group received treatments at a different time and in a different room from the TTM group to make sure that they did not know which treatment group they were in by observing the other group. The sham US was used as the comparable regimen because US was generally recommended to be used as the standard treatment for muscle pain and CTTH. The high-frequency sound waves of US are likely to stimulate tissue heating and healing effects. The conventional US technique with continuous-wave mode was used. In this technique, the applicator is usually applied with an Aquasonic® (Parker Laboratories, Fairfield, New Jersey) gel to the skin, which creates a friction-free surface. The US probe is moved in smooth overlapping sweeps or circular motions for several minutes. 20 These motions imitate manual massage and may provide some massage effects. After the study period ended and all data were collected, the participants could request an additional massage treatment by a physical therapist if they wished.
Both treatment groups received nine 30-minute sessions during a period of 3 weeks. In addition, all participants were allowed to take the medication that was already prescribed for them; this was monitored every day of treatment.
Assessment
Each participant's demographic characteristics and history of headache were recorded. The clinical outcomes were grouped as primary and secondary outcome measures. The primary outcome measure was the PPT. The secondary outcome measures or other parameters related to headaches included the 24-hour VAS, pain frequency (times/week), pain duration (hours by average/time), suboccipital and neck range of motion (degrees), the Headache Disability Index (HDI) score, and adverse effects. All outcome measures were assessed by the second physical therapist, who had 5 years of experience and was blinded to the treatment group of each participant. The reliability tests of all outcome measures were done with 10 participants with episodic CTTH before the main study. The assessment time was before and after 3 weeks of treatment and at follow-up at 3 and 9 weeks after the last treatment.
Additional secondary outcome measures were asked, such as satisfaction with the assigned treatment, adverse effects, and presence or absence of signs and symptoms (e.g., soreness, fever, or more pain) after each treatment session.
PPT
The Commander™ Algometer and DigiTrack (JTECH Medical, Salt Lake City, Utah) was used to measure PPT levels. This algometer consists of a 1-cm2 rubber-tipped plunger applied to each trigger point. PPT was defined as the minimal amount of pressure required from the initial sense of pressure to the first sense of pain. 21 The most painful MTrPs were selected for recording. According to Simons and colleagues (1999), these MTrPs should be active, cause a clinical symptom, and refer to patient-recognized pain on compression. 22 These MTrPs are always found related to specific muscles of the posterior neck and upper back muscles. The muscles with the most painful trigger points were recorded. The participants were asked to indicate the sensation of pressure to the first change to pain three times. The average (pound/cm2) PPT was used for the main data analysis.
Headache intensity on VAS
The participants were asked about the average intensity of pain that they had experienced during the past 24 hours by using a VAS with a 10-cm line ranging from 0 to 10. The participants were asked to mark the point on the line. Zero indicated no pain, and 10 indicated the most pain ever experienced. Response on the scale was evaluated before each treatment for detailed monitoring.
Pain frequency and duration
Participants were asked to indicate the pain frequency expressing in times/week, before treatment at the first treatment each week, after 3 weeks, and at the follow-up points of 3 and 9 weeks. Pain frequency was expressed as times/week.
Suboccipital and neck range of motion
Suboccipital movements were measured in flexion and extension. Neck or cervical spine movements in flexion, extension, lateral flexion, and rotation were assessed before and after the first treatment, after 3 weeks, and at subsequent 3- and 9-week follow-up. A cervical range of motion was applied for this assessment. This device has high reliability (intraclass correlation coefficient [ICC] range, 0.96–0.99). 23
HDI Questionnaire
The HDI questionnaire consists of 25 items answered with one of three responses: yes (4 points), sometimes (2 points), or no (0 points). A total score change of at least 29 points was necessary for effects to be considered clinically significant. The HDI has good internal consistency (0.89), robust long-term test–retest reliability (ICC, 0.83), and good construct validity. 24
Data analysis
The third physical therapist, who had MSc and PhD degrees in epidemiology and biostatistics, analyzed the data and was completely blinded to the patients' group assignments. All analyses were performed on the basis of the intention-to-treat principle. Imputation of outcomes by carrying the last known outcome status forward was used to minimize the bias introduced by loss to follow-up. 25
The major outcome measures were presented as mean±standard deviation (SD). This study aimed to analyze each outcome separately at different points of time during the treatment period to detect the short-term (after 3 weeks of treatment) and long-term (at 3 and 9 weeks after last treatment) therapeutic effectiveness. To compare continuous outcome variables between baseline with post-test data of outcome measures after 3 weeks of treatment and at 3 and 9 weeks of follow-up, one-way repeated-measures analysis of variance was performed. The randomization method did not assure that baseline characteristics would be the same between groups. An analysis of covariance was performed to compare differences in outcome measures between the two treatment groups. Outcome measures taken before the first treatment were used as covariates. The adjusted mean differences and the 95% confidence intervals for each outcome measure of each evaluation time point were estimated to compare differences in all outcome measures between the two treatment groups. To achieve statistical significance, 80% power and overall two-sided 5% significance were used. In addition, the effect size (Cohen d) was calculated to examine the average effect of PPT and headache intensity between both treatment groups. 26
Results
Table 1 shows the demographic characteristics of the two groups. These variables did not significantly differ between the groups (p>0.05). Figure 3 shows the PPT at initial baseline, after 3 weeks of treatment, and at 3 and 9 weeks of follow-up. These values were 2.71±1.22 pounds/cm2, 3.57±1.41 pounds/cm2, 3.72±1.46 pounds/cm2, and 3.42±1.46 pounds/cm2, respectively, in the TTM group and 2.85±1.20 pounds/cm2, 2.62±1.07 pounds/cm2, 2.58±1.05 pounds/cm2, and 2.63±0.94 pounds/cm2 for the sham US group. PPT significantly improved after treatment and at 3 weeks of follow-up (F=6.22; p=0.006), while values in the sham US group did not change. PPT in the TTM group was better than in the sham US group, with a mean difference of 1.03 pound/cm2 (95% confidence interval [CI], 0.54–1.53 pound/cm2), 1.21 (95% CI, 0.69–1.74 pound/cm2), and 0.84 (95% CI, 0.28–1.39 pound/cm2) at each assessment time (Table 2). The effect sizes of PPT at the three occasions of follow-up were 0.70, 0.83, and 0.58. Compared with the sham US group, the TTM group also revealed a better result, with effect sizes of 0.76, 0.90, and 0.64 at each assessment time. These effect sizes reflected medium to large effects. The method of measuring PPT in this study showed a high reliability (ICC, 0.96 [95% CI, 0.90–0.99]).
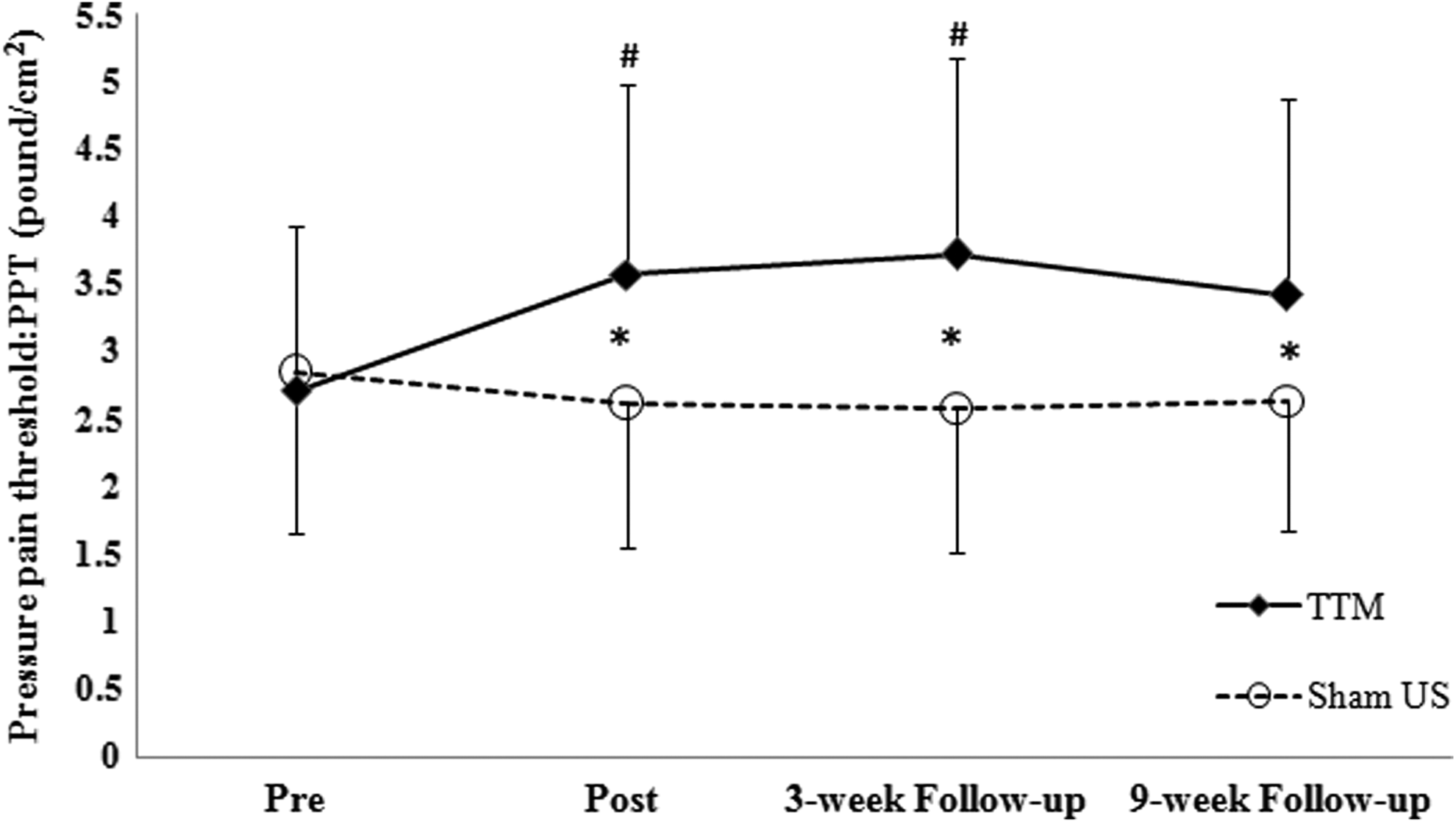
Pressure pain threshold (PPT) at baseline (Pre), after 3-week of treatment (Post) and at 3- and 9-week follow-up for TTM and Sham US. Values are means±standard deviation (SD). Error bars indicate SD. “#” denotes statistically different (p<0.05) from baseline in TTM and “*” indicates statistically different (p<0.05) between treatment groups.
Values expressed with a plus/minus sign are the mean±standard deviation.
TTM, Thai traditional massage; US, ultrasound; CTTH, chronic-tension type headache
Statistically significant difference between treatment groups (defined as p<.05).
CI, confidence interval; VAS, visual analogue scale.
Headache intensity showed a significant decrease at all assessment times in both groups (Fig. 4). The mean change at follow-up from baseline data was about 40%–50%; the pain was reduced by 2 points on the VAS (effect size ≥0.80). In addition, this finding was maintained at 3 and 9 weeks of follow-up (F=24.45 and 13.50; p<0.001). The VAS score did not significantly differ between the two groups at any assessment (Table 2).
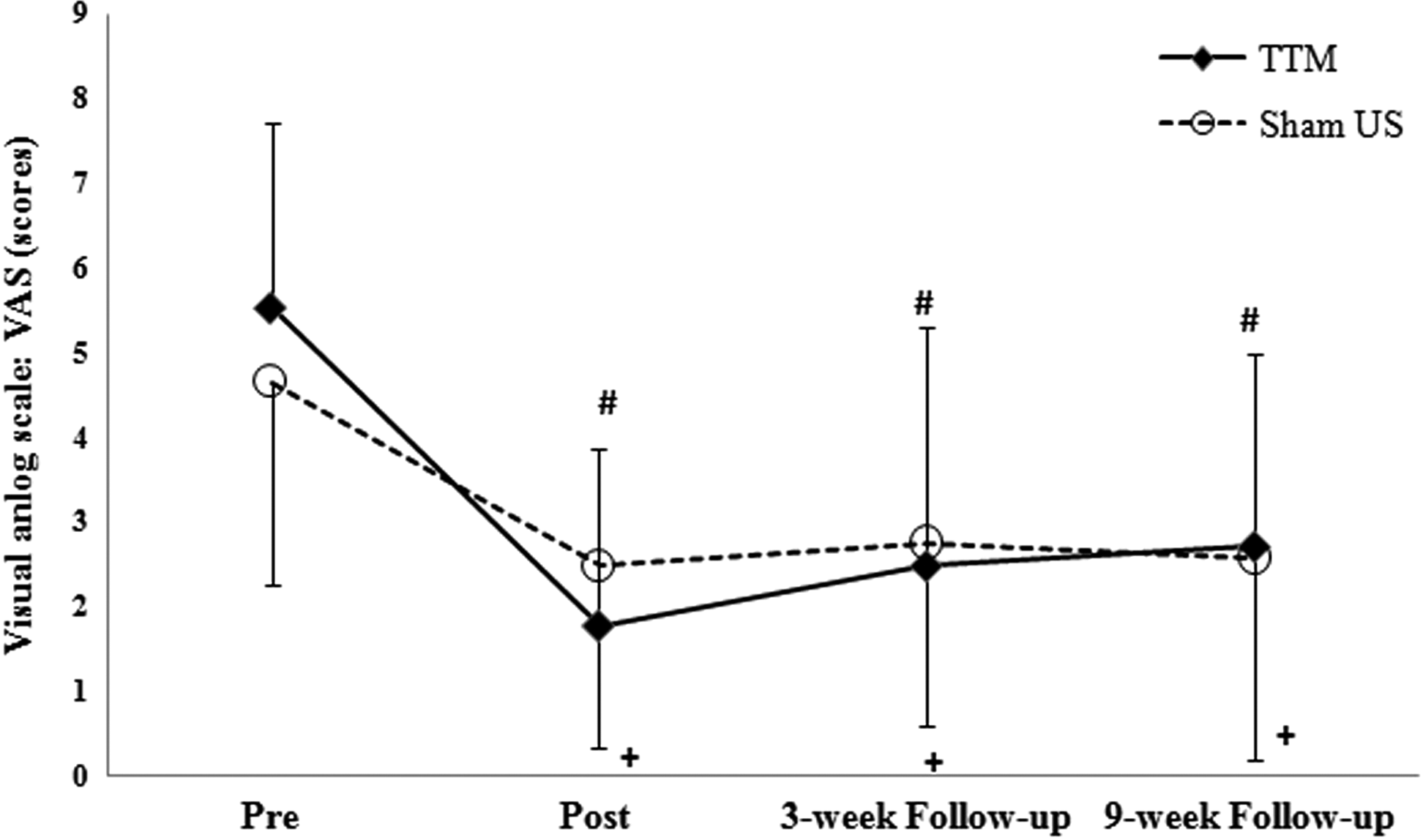
Visual analog scale (VAS) at baseline (Pre), after 3-week of treatment (Post) and at 3- and 9-week follow-up for TTM and Sham US. Values are means±SD. Error bars indicate SD. “#” and “+” denote statistically different (p<0.05) from baseline in TTM and Sham US, respectively.
The other parameters related to headache showed that the TTM group improved with regard to headache frequency, headache duration, and HDI score at all post-treatment assessment times. For suboccipital and neck range of motion, only some parameters—suboccipital flexion/extension, left/right cervical lateral flexion, and right cervical rotation—were significantly higher in the TTM group than the sham US group at the 3-week follow-up (p<0.05). When the study was complete, 97% of the participants from the TTM group and 78% of those from the sham US group reported that they were satisfied with their assigned treatment. This study showed a high reliability with this device (ICC range, 0.94–0.99).
During the treatment period, 6 patients from the TTM group and 5 from the sham US group, reported having a mild fever, mild soreness, and other discomfort; however, they all recovered from adverse effects after 15–60 minutes without using any medication. Both groups reported decreasing use of analgesic medication, from 25 (69.4%) to 10 (27.8%) in the TTM group and from 25 (66.7%) to 9 (25.0%) in the sham US group.
Discussion
The main findings of this study were that 3 weeks of TTM increased PPT and decreased headache intensity in patients with CTTH and migraine headaches. This effect was evaluated 3 and 9 weeks after treatment, with effect sizes reflecting a medium to large effect. The percentage improvements of PPT after the treatment and at 3 and 9 weeks of follow-up for TTM were 31.7%, 37.3%, and 26.2% of the baseline values, respectively. When compared with the sham US group, PPT values after the treatment and at the 3 and 9 weeks of follow-up for the TTM group had improved by 26.6%, 30.7%, and 23.2%, respectively. Previous studies showed that TTM resulted in a significantly higher PPT than Swedish massage or physical therapy for patients with back pain 10 and the scapulocostal syndrome 27 after 3 week of treatments. The immediate effect of TTM on PPT was also found after one treatment in patients with episodic tension-type headache. 28 These studies show that TTM may reduce pain from stimulating MTrPs. It has been known that treatment of MTrPs using dry needling relieves muscle pain and headaches. 29 Other reports suggest that TTM has similar effects as dry needling while being a noninvasive and safe technique. 7,8 These findings indicate that TTM can be used as an alternative treatment for patients with headache and other pain related with neuromuscular disorders.
TTM, which uses deeper pressure followed by passive stretching, was applied along the massage area, which covers all muscles with MTrPs. This massage may break down any MTrP adhesions. The activation of MTrPs as both local and referred pain may have reproduced the headache patterns. 22,30,31 Fernández-de-Las-Peñas and colleagues found the most frequent site of MTrPs was in the upper trapezius muscle (95.83%). 30 According to Simons and colleagues, referred pain evoked by MTrPs in the upper trapezius muscle may spread ipsilaterally from the posterior-lateral region of neck (behind the ear) to the temporal region. 22 Toro-Velasco and colleagues 32 reported a non–statistically significant difference in PPT with use of only one session of head and neck massage for patients with CTTH. It is possible that most of the patients in this study had headaches associated with MTrPs in the upper trapezius muscle region. In addition, massage may reduce ischemia and increase blood flow to allow decreased MTrP sensitivity. 33,34
By all of these mechanisms, deep pressure along the meridian lines and passive stretching on muscles having MTrPs in TTM may be responsible for the pain relief in CTTH and migraine headaches in the current study. It seems that MTrPs may be the major source of pain among patients with CTTH and migraine. Therefore, further study should focus on massage for management of specific MTrPs.
Reduction of headache intensity after the treatment may be explained by a few theories. First, (1) Because MTrPs, which constitute an important source of chemical mediators (bradykinin, calcitonin gene–related peptide, serotonin, and substance P may be present in active MTrPs), 35 massage that reduces muscle tension and improves blood flow may wash out pain metabolites (e.g., substance P and lactic acid) and lead to reduced pain and muscle tension. 12 Second, TTM provides deep pressure, which may stimulate proprioceptors, such as spindle cells and the Golgi tendon organ, in the target muscles. Reducing muscle spasm and adhesion in tissues will reduce pain. 10,11 Previous randomized 28 and single-group 14 studies found similar results on reduction of headache intensity resulting from TTM. These results were also in line with various forms of Western massage, in which the effect of massage on pain relief was seen when the massage focused on the muscles with MTrPs in CTTH and migraines. 36 –39 In the current study, headache intensity, as assessed on a VAS, improved in both the TTM and sham US groups, but no significant differences were seen between the two groups. This could be explained by the effect of kneading massage by the sound head of the sham US.
This study had some limitations. The findings may not be extrapolated to the overall population because most participants were students (67%), their ages ranged from 20 to 35 years (84%), and most were women (77%). These characteristics may affect the results of the study because young people are generally quicker to recover from their fatigue or high tension status than middle-aged and elderly individuals. In addition, the duration of treatments may not have been long enough to obtain the maximum effects for patients with chronic symptoms. Therefore, future studies should include other age groups, especially middle-aged and elderly individuals, and use a longer duration of treatment.
In conclusion, these results indicate that TTM can improve both PPT and headache intensity during both the short-term of treatment and during the relatively long-term of post-treatment. TTM could be promoted as an alternative treatments for patients with CTTH and migraines.
Footnotes
Acknowledgments
The authors gratefully acknowledge the Faculty of Associated Medical Sciences Khon Kaen University, Thailand, for supporting the research setting. The Under Incubation Researcher Project, Back, Neck and Other Joint Pain Research Group, Neuroscience Research and Development Group, Khon Kaen University, Thailand, provided valuable research funding. The authors thank Professor James A. Will for editorial assistance. Finally, the authors express sincere gratitude and appreciation to all participants for their generosity and willingness to participate in this study.
Disclosure Statement
No competing financial interests exist.