
Abstract
Objectives:
The objectives of this study were to determine the effects of the novel Buddhism-based walking meditation (BWM) and the traditional walking exercise (TWE) on depression, functional fitness, and vascular reactivity.
Design:
This was a randomized exercise intervention study.
Settings/location:
The study was conducted in a university hospital setting.
Subjects:
Forty-five elderly participants aged 60–90 years with mild-to-moderate depressive symptoms were randomly allocated to the sedentary control, TWE, and BWM groups.
Interventions:
The BWM program was based on aerobic walking exercise incorporating the Buddhist meditations performed 3 times/week for 12 weeks.
Outcome measures:
Depression score, functional fitness, and endothelium-dependent vasodilation as measured by the flow-mediated dilation (FMD) were the outcome measures used.
Results:
Muscle strength, flexibility, agility, dynamic balance, and cardiorespiratory endurance increased in both exercise groups (p<0.05). Depression score decreased (p<0.05) only in the BWM group. FMD improved (p<0.05) in both exercise groups. Significant reduction in plasma cholesterol, triglyceride, high-density lipoprotein cholesterol, and C-reactive protein were found in both exercise groups, whereas low-density lipoprotein cholesterol, cortisol, and interleukin-6 concentrations decreased only in the BWM group.
Conclusions:
Buddhist walking meditation was effective in reducing depression, improving functional fitness and vascular reactivity, and appears to confer greater overall improvements than the traditional walking program.
Introduction
D
Most depressed patients have a sedentary lifestyle due, in part, to low motivation and energy. 10 This is unfortunate because habitual exercise has been shown to decrease the risk of CHD, diabetes, and stroke in aging populations 11,12 and is a nonpharmacologic method that has been used for the treatment of depression. 13 Developing effective preventive and treatment programs that not only act on both depression and vascular disease but also are suitable for the elderly populations will be of paramount importance. Many countries, including Thailand, choose a holistic concept in health promotion and use the mind–body approach that combines physical activities and mental exercises. Mind–body exercise modalities such as yoga 14 and t'ai chi 15 are examples of this strategy. There is also an increasing recognition that changes in mind can modulate alteration in vascular health. For example, mirthful laughter induces beneficial effects on vascular compliance. 16
Walking meditation or mindful walking is a widely performed form of Buddhist practices that focus on mind–body interactions. It incorporates the basic principles of traditional meditation performed in the sitting position, including breathing, awareness, concentration, and relaxation, with rhythmic exercise of walking. In the present study, the customized walking meditation exercise was created to incorporate the spiritual movements of the arm swing while praying Budd–Dha during walking. In this practice, each step is taken after each breath, being aware of the alternating intervals of contraction and relaxation involved with walking exercises. This form of exercise is amenable to a modern lifestyle and can be practiced easily by the elderly who have a number of limitations.
Accordingly, the primary aim of the present investigation was to determine the effects of the Buddhist walking meditation (BWM) on depression, functional fitness, and endothelium-dependent vasodilation compared with the sedentary controls in the elderly with mild-to-moderate depression. In order to assess the relative efficacy of this spiritual exercise, the results were compared with those obtained with the traditional walking exercises (TWE). Moreover, it was determined whether the changes in depression were accompanied by corresponding changes in inflammatory markers and endothelium dysfunction that are characteristics of depression.
Materials and Methods
Subjects
A total of 45 female elderly with mild-to-moderate depression aged 60–90 years were recruited from the two welfare centers in Bangkok, Thailand. These centers are funded by the Thai government and provide meals and accommodations for people in Thailand. The inclusion criteria included mild-to-moderate depression as defined by Geriatric Depression Scale scores of 13–24, 17 normal mobility and independent self-care, no cardiovascular disease, no hypertension, and no diabetes mellitus; adequate communication ability, no history of psychiatric illness, and no current psychiatric medications. Only subjects whose electrocardiogram showed no significant abnormality were admitted to the study. An informed consent was obtained from all subjects. The study was approved by the Ethical Review Committee for Research Involving Human Research Subjects at Chulalongkorn University.
The eligible subjects were stratified based on age and depression levels (mild-to-moderate depression) and then were randomly allocated into three groups using the random number table generated by the computer: the sedentary control group (CON; n=15), the traditional walking exercise training (TWE; n=15), and the Buddhism walking meditation (BWM; n=15). Subjects were excluded if they completed less than 80% of the training sessions. A total of 5 subjects dropped out by the end of the study. The reasons for withdrawal included: loss of follow-up, physical discomfort, and a lack of compliance. Those remaining were 13 subjects in the CON group, 13 subjects in the TWE group, and 14 subjects in the BWM group. All of the subjects were instructed not to alter their physical activity, dietary, and lifestyle habits throughout the intervention period.
Exercise training program
Both TWE and BWM exercise programs were divided into two phases. In phase 1 (weeks 1–6), TWE and BWM training programs were conducted at mild intensity (20%–39% individually determined heart rate reserve) performed for 20 minutes, 3 times a week. In phase 2 (weeks 7–12), the training intensity was increased to moderate intensity (40%–50% heart rate reserve) performed for 30 minutes, 3 times a week. Both exercise programs were closely supervised by one of the investigators. Adherence to the prescribed exercise intensity was confirmed using heart rate monitors (Polar Team 2 Pro, USA). Both TWE and BWM programs also included 11 common stretching exercises performed during warm-up and cool-down stages. All of the exercise training involved walking on the 50-m oval-shaped indoor track.
The BWM program created and customized for the present study was based on aerobic walking exercise incorporating Buddhist meditations. The subjects performed walking exercises while rhythmically swinging both arms while voicing “Budd” with arm swing up and “Dha” with arm swing down and were instructed to practice mindfulness while walking. In phase 2 of the exercise training, the training workload was increased by subjects holding a 500-mL water bottle in each hand. This practice was necessary in order to increase the exercising heart rate (or exercise intensity) without increasing step rates, which must be maintained for proper meditations.
Measurements
Depression score
The Geriatric Depression Scale (long form) questionnaire developed by Yasavage 17 was translated into the Thai language for the Thai Geriatric Depression Scale (TGDS). 18 The scale consists of 30-item questions with “yes” or “no” answers and has a score range of 0–30, with the scores 0–12 indicating no depression, 13–18 mild depression, 19–24 moderate depression, and 25 or more severe depression. In this study, the subjects with mild-to-moderate depression (i.e., TGDS scores 13–24) were recruited.
Functional fitness measures
Prior to the testing, subjects were familiarized with each physical fitness testing measure. Body composition was measured using the Innerscan Body Composition Monitor (BC 533, Tanita Corporation of America, USA). Heart rate was measured with the heart rate monitor (Polar Team 2 Pro, USA). Cardiovascular endurance was assessed with the 6-minute walk test and expressed as the meters that the subjects walked in 6 minutes around a 50-yard course. Upper and lower muscle strengths were measured with the 30-second arm curl test (number of biceps curls completed while holding a hand weight of 2.27 kg for women and 3.63 kg for men) and the 30-second chair-stand test. The back scratch flexibility test (how close the hands can be brought together behind the back) and the chair sit-and-reach test were used to measures upper and lower limb flexibility, respectively. The timed up-and-go test was used as a measure of agility and dynamic balance.
Endothelium-dependent vasodilation
Brachial artery characteristics were assessed with ultrasound equipment (CX50, Philips, USA), using the arterial occlusion technique on the right forearm. All subjects rested in the supine position for 20 minutes. The brachial artery was imaged above the antecubital fossa in the longitudinal plane. Baseline data were monitored for 1 minute and then the cuff placed around the right forearm was inflated rapidly to 50 mm Hg above systolic blood pressure for 5 minutes and deflated for 5 minutes of recovery. 19,20 Mean blood velocity was sampled by using the pulsed-wave Doppler mode. In order to eliminate investigator bias in image analyses, arterial distension was measured using a computer software program (Brachial Analyzer, Medical imaging applications, USA). Shear rate was calculated by blood velocity/vascular diameter. Flow-mediated dilation (FMD) was calculated using the formula FMD=(D2-D1) x 100/D1, where D1 is the brachial artery diameter at baseline, and D2 is the maximal postocclusion brachial artery diameter. 19
Blood analyses
After 8 hours of overnight fasting, the venous blood sample was collected from the antecubital vein. Blood samples were then centrifuged at 3500 rpm for 10 minutes at 4°C for separation of erythrocyte and plasma. Nitric oxide (NO) concentration, as estimated by total nitrate plus nitrite concentrations, was measured in plasma samples with the commercial assay kit (colorimetric NO assay kit, PromoKine, Germany). IL-6 was measured in plasma samples with enzyme-linked immunosorbent assay kits (eBioscience, Vienna, Austria). Plasma cortisol, C-reactive protein (CRP) and lipoprotein concentrations were measured with standard procedures at the certified clinical laboratory (BRIA Lab, Bangkok, Thailand).
Statistical analyses. All the data were first checked for normality and were transformed to a normal distribution if it was found to be violated. Two-way (group×time) analyses of variance (ANOVA), followed by Bonferroni multiple comparisons were used to determine the significant differences among group means. In an attempt to compare the magnitudes of changes among groups, percent change scores were created and compared using one-way ANOVA. A statistical level of p<0.05 was considered a priori to be a statistically significant difference. The data were expressed as means±standard error of the mean unless indicated otherwise.
Results
Body mass and body–mass index (BMI) decreased (p<0.05) in the TWE and the BWM groups (Table 1). A significant decrease in body fat percentage was only observed in the BWM group. Both systolic and diastolic blood pressure decreased in both exercise training groups (all p<0.05). No significant changes were observed in the sedentary control group except that there were small but significant increases in body mass and BMI.
Data are mean±standard error of the mean.
p<0.05 vs. Pre, † p<0.05 vs. Sedentary control using analysis of variance.
BMI, body–mass index; BP, blood pressure.
The depression score decreased (p<0.05) in the BWM group (16.8±0.9 vs. 8.6±0.6 U), and the magnitude of reductions in depression was significantly greater in the BWM than in the TWE group. No significant changes in depression scores were obtained in the TWE (17.3±1.0 vs. 15.5±0.9 U) and sedentary control group (17.9±0.7 vs. 18.6±0.6 U) (Fig. 1).
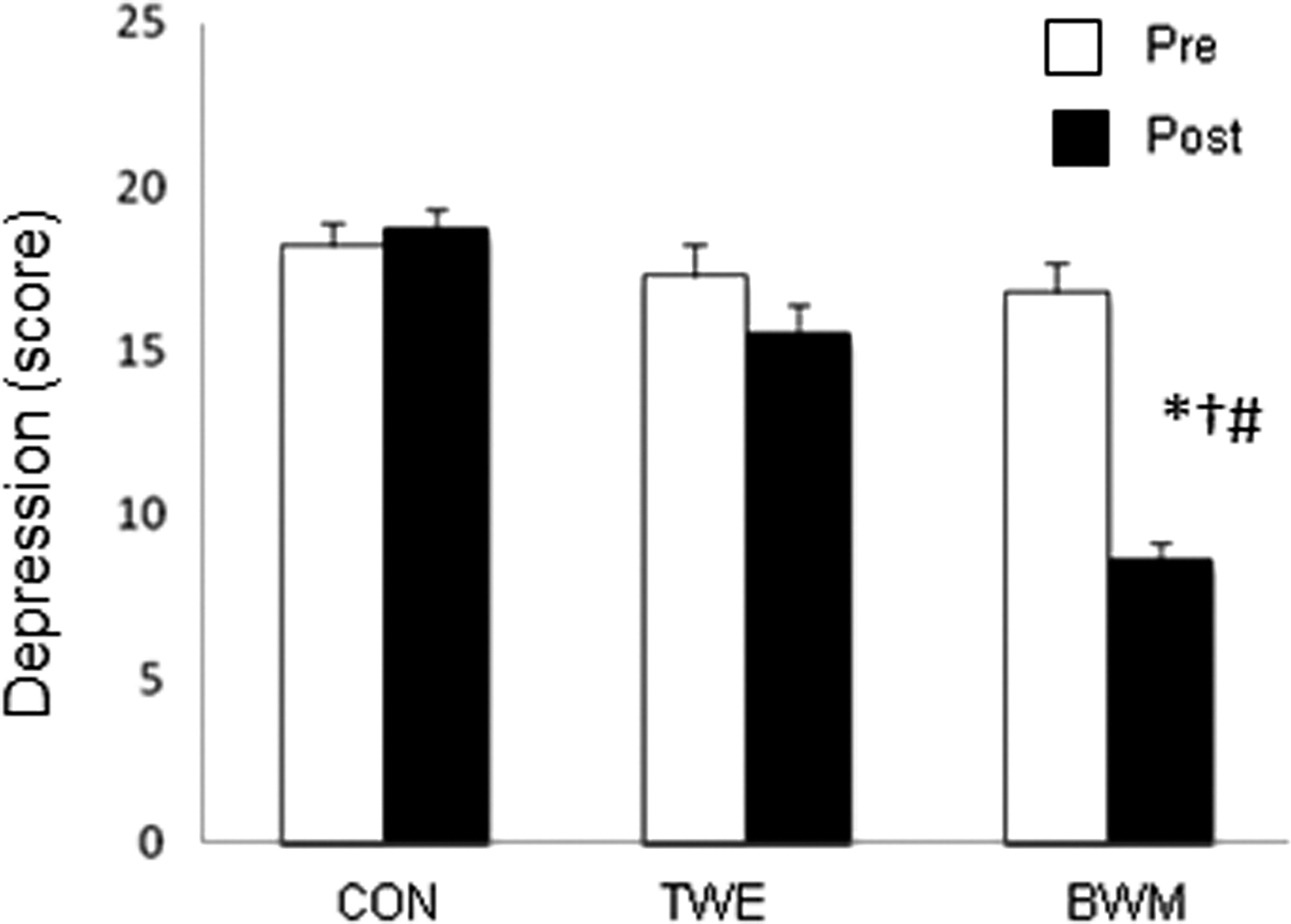
The comparative depression scores between baseline (Pre) and after 12 weeks (Post) among 3 groups of subjects: sedentary control group (CON), traditional walking exercise group (TWE), and Buddhism walking meditation group (BWM). Data are mean ± standard error of the mean. *p<0.05 vs. Pre, † p<0.05 vs. Sedentary control, # p<0.05 vs. traditional walking using analysis of variance.
Measures of functional fitness, including muscle strength as measured by arm curl and chair stand, flexibility as assessed by back scratch and chair sit-and-reach, agility and dynamic balance on timed up-and-go, and 6-minute walk test all increased (p<0.05) in both exercise groups (Table 2). The improvement in 6-minute walk test was significantly greater in the BWM than in the TWE group. No significant changes were observed in the sedentary control group.
Data are mean±standard error of the mean.
p<0.05 vs. Pre, † p<0.05 vs. sedentary control using analysis of variance.
As shown in Table 3, endothelium-dependent vasodilation as assessed by FMD improved (p<0.05) in both the BWM and TWE groups. At baseline, the depression score was significantly and inversely related to FMD (r=−0.38, p<0.05).
Data are mean±standard error of the mean.
p<0.05 vs. Pre, † p<0.01 vs. sedentary control, # p<0.01 vs. traditional walking using analysis of variance.
Plasma concentrations of total cholesterol, triglycerides, and CRP decreased in both the TWE and BWM groups (Table 4). Significant reductions in plasma cortisol, low-density lipoprotein cholesterol and IL-6 concentrations were only observed in the BWM group. Nitric oxide concentration increased significantly in both the BWM and TWE groups.
Data are mean±standard error of the mean.
p<0.05 vs. Pre, † p<0.05 vs. sedentary control using analysis of variance.
Discussion
The salient finding of the present study is that Buddhism-based walking meditation produced improvements in depression score, functional fitness, and vascular function in elderly female patients with mild-to-moderate depression. The magnitude of improvements in vascular function and functional fitness was equivalent to those induced by TWE. More notably, only the walking meditation resulted in a reduction in depression scores and plasma concentrations in cortisol and IL-6. The present results suggest that Buddhism-based physical exercise that incorporated the mind and body interactions were effective in reducing depression and cardiovascular disease risk factors and in improving functional fitness and vascular function in elderly with depressive symptoms. To the best of our knowledge, this is the first study to report beneficial effects of Buddhism-based walking meditation on a variety of cardiovascular and functional indices that are relevant to older populations.
There has been growing attention and interest in spiritual or religious matters in the management of overall health and quality of life. In the same vein, regular physical activity is a relatively well-established strategy for maintaining and enhancing health and quality of life. In the present study, Buddhism-based walking meditation was incorporated into the arm-swing physical exercises. This particular form of mind and body exercises that could yield a dual effect was effective in eliciting improvements in a variety of cardiovascular and functional fitness measures. The current study is consistent with previous studies that reported beneficial effects of other mind and body exercises, including t'ai chi, yoga, 21 kouk-sun-do, 22 and Turkish folklore dance. 23 More importantly, a decrease in depression scores was observed only in the spiritual exercise group. It is well known that compliance and adherence to the exercise program are very low and rather disappointing. On the other hand, the practice in religions is a life-long commitment. It remains to be seen whether the inclusion of religious matter in the exercise program can lead to greater compliance and adherence in the long term. In the present study, 2 subjects dropped out from the TWE group but none in the BWM group.
Endothelium-dependent vasodilation as measured by FMD is impaired in depressed, compared with nondepressed, individuals. 6 The present data showed that both exercise programs increased FMD in elderly subjects with depression. The increase in the “functional” measure of endothelium-dependent vasodilation was accompanied by the increase in the “biochemical” measure of plasma NO level. These results indicate that walking exercises have beneficial effects on endothelial function via increased blood flow and shear stress resulting in increased NO production and consequent vasodilation. 24,25 It was also found that FMD was increased by 88% in the BWM group, while the TWE group increased it by 72%, indicating that BWM might have superior improvements in endothelial-dependent vasodilatation compared with TWE.
It should be noted that the inclusion of the traditional walking program was not intended to perform a direct head-to-head comparison with the BWM but to gauge the efficacy of the walking meditation relative to the familiar physical exercise mode. In addition to the meditation component, the BWM was different from the TWE in that the subjects performed arm swinging by holding weights in each hand to increase upper limb workloads. In the traditional walking program, the subjects were able to increase walking speed as they got fitter. This was not possible for the subjects in the walking meditation because the faster cadence (step rate) interfered with the proper timing/duration of Buddhist meditations. In an attempt to match both exercise programs for exercise intensity, we added arm swinging by holding water bottles in each hand for the BWM group. The BWM program produced more widespread effects than the TWE program. A previous study demonstrated that exercise training using a flexible stick—an exercise program that simultaneously combines aerobic and resistance exercise components—showed superior improvements in health-related physical fitness and cutaneous microcirculatory responsiveness compared with t'ai chi in older women. 26 Consistent with this, Maeda et al. 27 demonstrated that resistance training increased endothelial function without inducing arterial stiffening in older adults. Thus, the greater effects of the BWM on cardiovascular function could be attributed to the additional upper body resistance load applied to aerobic exercise in the BWM group.
One of the consistent physiologic abnormalities reported in major depression is cortisol hypersecretion. 28 In this study, only the BWM group showed a decrease in depression score accompanied by decreased cortisol level. There is accumulating evidence to suggest that hypothalamic–pituitary–adrenal (HPA) axis alteration is involved in the etiology and pathogenesis of depression. 29 Dysregulated HPA can produce hypersecretion of cortisol into the bloodstream and is associated with elevated concentrations of CRP and IL-6 that could lead to impaired endothelial function. 30 –33 It is possible that the reason walking meditation exercise causes greater improvement than TWE in depressed elderly individuals is due to its greater efficacy in alleviating depression as a result of its attenuation of cortisol, leading to a reduced inflammatory process.
There are several limitations in the present study. First, the number of subjects studied is relatively small. As such, this study may be considered a pilot study and needs to be verified by a larger clinical trial. Second, the duration of the exercise intervention was relatively short. A longer-term intervention study is warranted.
Conclusions
Similar to the TWE, the Buddhism-based walking meditation intervention that incorporated arm-swing exercises was effective in improving impaired functional fitness and vascular dysfunction, which are characteristics of the depressed elderly. The walking meditation was also able to decrease depression, plasma concentrations of cortisol, and inflammatory markers that the TWE failed to modify. Collectively, these results indicate that the spiritually oriented walking meditation exercise may be the novel therapeutic modality that may be suitable for improving physical and psychologic functions in elderly with mild and moderate depression symptoms.
Footnotes
Acknowledgments
This study was supported by the 90th anniversary of the Chulalongkorn University fund (Ratchadaphiseksomphot endowment fund) and the Faculty of Sports Science fund at Chulalongkorn University. The authors are very grateful to all participants in this study. We also would like to thank Dr. Supranee Buranapraditkun for her technical assistance.
Disclosure Statement
No competing financial interests exist.