
Abstract
Background and purpose:
Unilateral forced nostril breathing (UFNB), a yogic pranayama technique, improves verbal and spatial cognition in healthy adults. The use of UFNB as an adjunct in aphasia recovery has not been explored. The current study investigated the use and potential benefit of combining UFNB with conventional speech-language therapy.
Methods:
A multiple baseline single-subject AB design was conducted across three participants with stroke and aphasia. All participants practiced 40 minutes of UFNB daily at home, after instruction, and received conventional aphasia therapy. Speech and language skills were assessed before and after intervention, with individualized assessments throughout the period. Assessments included the Western Aphasia Battery-R (WAB-R) and the Communication Abilities of Daily Living-2 (CADL-2), as well as the Apraxia Battery for Adults if a diagnosis of apraxia was present. The Color Trails Test was performed and language samples collected for Correct Information Unit (CIU) and word productivity analyses.
Results:
For the pre- and postassessments, visual inspection revealed an increase in CADL-2 scores for participants A2 and A3. In addition, A1 and A3 had a slight trend of increasing WAB-R aphasia quotients. Some change was observed for total number of CIUs and word productivity in two of the three participants. Attention did not markedly improve from baseline to treatment phase.
Conclusion:
This study suggests that UFNB combined with speech-language therapy may benefit overall language production and functional communication. Further investigation on use of UFNB treatment alongside traditional speech-language therapy is warranted.
Introduction
T
The use of altered breathing patterns in pranayama to change cognition and language in those living with aphasia is understudied. 4 Aphasia is a communication disorder characterized by linguistic and attention impairments. 5 –11 If yogic breathing techniques prove to be beneficial for reducing aphasic impairments, the approach would offer adults with aphasia a no-cost intervention with considerable flexibility (i.e., used at any place and at any time).
Among the several types of yogic breathing, unilateral forced nostril breathing (UFNB) may hold the most promise for the treatment of aphasia. UFNB alters electroencephalographic (EEG) amplitudes in the brain's hemispheres. 12 –14 There are naturally occurring cycles of nasal dominance, and EEG activity is greater in the hemisphere contralateral to the dominant nostril (for a review, see Shannahoff‐Khalsa 13,14 ). 13 –15 This naturally occurring dominance is related to verbal or spatial abilities, with unobstructed nasal dominance linked to cognitive performance in the contralateral hemisphere. 16 Further research supports EEG activity and hemispheric dominance shift contralaterally with a change in nasal dominance, 15 and changes in hemispheric dominance can be induced when an individual engages in UFNB. 12 –14,17 Previous research has also demonstrated increased verbal abilities for women who complete right nostril breathing and enhanced spatial abilities in those who complete left nostril breathing. 18 Others support increased cognitive function in the contralateral hemisphere (e.g., spatial memory) in non–brain-damaged individuals, 12,17,19 as well as changes in hemispheric dominance, 12 cognitive abilities, 16,18 and increased oxygen consumption. 20 If hemispheric dominance is altered through UFNB, 15 this particular pranayama practice may help strengthen the function of the damaged hemisphere following stroke.
Because UFNB may be a novel adjunct to traditional speech-language treatment, the current study sought to explore whether adults with aphasia could be taught the technique; whether the technique could then be simultaneously practiced as traditional speech-language therapy occurred; and, finally, how a combined traditional therapy and UFNB would affect the language and attention skills of adults with aphasia. The prediction is that using UFNB by adults with aphasia will result in positive outcomes of traditional speech-language treatment because it will address the underlying attention deficits in aphasia. By measuring the recovery of linguistic and attention skills of adults with aphasia following stroke, the results of this study may provide more insight into the effect of combining complementary and alternative medicine with traditional aphasia treatments.
Case Studies
Design
To control for possible threats to internal validity, a multiple baseline single-subject AB design was conducted across three participants. 21 –23 Each participant had a different length of baseline (phase A), resulting in introduction of treatment phase (phase B) at different times. A withdrawal phase (A2) was not introduced because of the potentially long-lasting effect of UFNB. 24
Materials and Methods
The participants were given pre- and postassessments, which included the Western Aphasia Battery-R (WAB-R) 25 and the Communication Abilities of Daily Living-2 (CADL-2). 26 A third assessment, Apraxia Battery for Adults (ABA-2), 27 was also given to A1 and A2 because of their accompanying diagnosis of apraxia of speech (AOS). The assessments were administered before the first baseline and after the last treatment data were obtained.
Three primary assessments were administered to track the combined influence of UFNB and traditional speech and language therapy on language and cognition. A fourth assessment, diadochokinetics, was administered if the participant had an accompanying diagnosis of AOS (as was the case with A1 and A2). The three primary assessments were as follows: (1) the Color Trails Test (CTT) to measure attention; (2) three 5-minute language samples composed of a scenario description task using the kite picture from the Minnesota Test for Differential Diagnosis of Aphasia, 28 the fireman picture from Nicholas and Brookshire (1993), 29 and the participants' description of an imaginary 2-week vacation to New York City; 30 and (3) a participant-specific assessment individualized according to specific treatment. A1's participant-specific assessment was orally reading 10 single-syllable functional words. Total words correct per session and percentage phonemic errors were calculated to track performance. A2's participant-specific assessment was saying 10 single-syllable words while completing step 4 and step 5 of Rosenbeck's eight-step continuum. 31 Lastly, A3's participant-specific assessment was a confrontational naming task of trained and untrained visual picture stimuli.
For each language sample, the following data were obtained: total Correct Information Unit (CIU) percentage, total number of CIUs, percentage word productivity, and total number of words. 32 All four of these variables were recorded to track the progress on each discourse in addition to the language sample as a whole. Specifically, these variables were recorded for the descriptions of the kite picture (Minnesota Test for Differential Diagnosis of Aphasia), 28 fireman picture, 32 and an imaginary vacation trip to New York City, as well as the summation of these three discourses.
CIU refers to the number of content words (words that are intelligible and relevant to the picture being described or topic being discussed) in a particular language sample. 32 Total word counts were also obtained so that in addition to having a number of CIUs, a variable of percentage of CIUs was available. Word productivity was defined as the proportion of productive words to total number of words. 33,34
Procedure
Preassessment
After providing consent, participants were assessed with the WAB-R, CADL-2, and ABA-2 (participants A1 and A2). No treatment was given at this time.
Phase A baseline
Repeated assessments (CTT, discourse/speech sample, and individualized participant-specific assessment) were administered during this phase as is typically performed for single-subject designs. After the percentage CIUs variable stabilized, participant A1 began the treatment phase. Additional baselines were obtained before the other participants were introduced to the intervention/treatment phase of the study.
Phase B treatment
At the beginning of the treatment phase, participants were instructed in the use of UFNB, using the nostril contralateral to the damaged hemisphere based on previous research. 12,16,18,19 A1 and A2 had left hemisphere strokes, so the left nostril was occluded (right UFNB or surya anuloma viloma pranayama). 35,36 A3 had a right hemisphere stroke; therefore, the right nostril was occluded (left UFNB or chandra anuloma viloma pranayama). 36 UFNB treatment began with an introduction to three-part breathing, or diaphragmatic breathing (deergha swasam pranayama). 37,38 With three-part breathing the participants were asked to be aware of sequential movement beginning with the expansion of the abdomen expanding, then the chest, and finally a slight rise in the collarbones. Expiration was a reversal (collarbones relax, chest lowers, and then abdomen pulls toward the spine). Deergha swasam is deep, slow breath that is thought to still the mind and has been used in individuals with anxiety. 37,39,40
Following this phase, the facilitator moved to instruction of the UFNB breathing technique. For UFNB, the participant was asked to use the nostril contralateral to the damaged hemisphere (i.e., close the nostril on the affected side), using whichever hand was unaffected by the stroke or was more comfortable. Participants were encouraged to work toward extending the exhalation to twice as long as the inhalation, with a ratio of 1:2. All participants were judged to be able to complete the UFNB practice during the initial training sessions, with no limb apraxia observed. Handouts outlining the practice and CDs with different lengths of guided UFNB were provided, and participants were supported with adequate time for questions and answers with a trained instructor. Further, participants were instructed to sit in a quiet place, with spine straight and eyes closed or soft and unfocused in front of them. The protocol also required the participant to complete UFNB treatment for a predetermined length of time every day.
Participants had twice-a-week sessions with researchers and were asked to continue practicing at home for the other days of the week. Each week, the amount of time required was increased, beginning with 5–10 minutes and subsequently increased by 5 minutes until the participant reached 40 minutes of UFNB a day for 6 days a week. 20 This increase took approximately 4 weeks to achieve. A 40-minute UFNB session was used because of the nature of brain injury and because most studies of UFNB have been done in the healthy population. Additionally, if the participants found the session to be too long to do all at once, shorter sessions were allowed, as long as the total minutes of UFNB reached the daily goal. All participants reported adherence with UFNB practice during the study.
Postassessment
After the treatment phase, participants were again assessed with the WAB-R and CADL-2, as well as the ABA-2 if a diagnosis of AOS was present.
Participants
Participants in this study included three individuals diagnosed with left or right hemisphere brain damage and aphasia (see Table 1). Two of the participants also had a diagnosis of AOS. A fourth individual began the study; however, he discontinued participation because of a broken hip. The participants were recruited through speech and hearing clinics at the University of Georgia and Georgia State University. All individuals had a diagnosis of mild to severe aphasia; had a high school education or more; had corrected or uncorrected visual acuity of at least 20/40; and passed an audiometric screening, aided or unaided, at 500, 1000, 2000, and 4000 Hz at 45 dB hearing loss in at least one ear. The three participants are described below:
WAB-R, Western Aphasia Battery-R.
A1
A 49-year-old woman who had a left hemisphere stroke 22 months earlier was diagnosed with Broca's aphasia according to the WAB-R. She also was diagnosed with moderate AOS according to the ABA-2. Scores at the initial assessment were as follows: WAB-R aphasia quotient (AQ) of 34.2 (severe deficits), a CADL-2 score of 70, and an ABA score of 2 (moderate severity). WAB-R scores revealed the lowest scores to be in the naming subtest (1.2 of 10), spontaneous speech (6 of 20), and auditory verbal comprehension (5 of 10). Performance on the CADL-2 placed her in the 40th percentile, which denotes a moderate-low level of functional communication abilities.
A2
A 51-year-old woman who had a left hemisphere stroke 21 months earlier was diagnosed with severe Broca's aphasia (WAB-R AQ score of 28.4) and moderate AOS (ABA-2 severity score of 2). WAB-R scores revealed the lowest scores to be in spontaneous speech (3 of 20), repetition (0.8 of 10), and naming (1.3 of 10). Performance on the CADL-2 placed her in the 22nd percentile, which denotes a low level of functional communication.
A3
A 74-year-old man who had a right hemisphere stroke 12 months earlier was diagnosed with global aphasia. Scores at the initial assessment were as follows: WAB-R AQ of 52.4 (moderate severity) and CADL-2 score of 61. Performance on the WAB-R revealed the lowest scores to be in naming (2.1 of 10), spontaneous speech (12 of 20), and repetition (3.9 of 10). Performance on the CADL-2 placed him in the 24th percentile, which denotes a low level of functional communication.
Analysis
The following variables were recorded each session and graphed: (1) CIUs, (2) word productivity, and (3) Color Trails 1 and 2. Participant performance was determined through visual inspection for some assessment measures. In addition, similar to Boyle (2004), 41 a numeric analysis was also completed to analyze results of the collected language samples. Average CIUs per minute 41 and average productive words per minute 33 were calculated to numerically compare baseline and treatment results from the collected language samples.
Case Results
For the pre- and postassessments (WAB-R and CADL-2, as well as ABA if a diagnosis of apraxia was present), visual inspection revealed an increase in CADL-2 scores for participants A2 and A3 (Fig. 1). In addition, A1 and A2 had a slight trend increasing WAB-R AQ (Fig. 2). For the two participants with an accompanying diagnosis of AOS who were given the ABA (A1 and A2), the ABA scores did not clearly improve. A1 demonstrated an improvement and the other, A2, showed no change (Fig. 3).

Communication Abilities of Daily Living-2 (CADL-2) scores for all three participants.
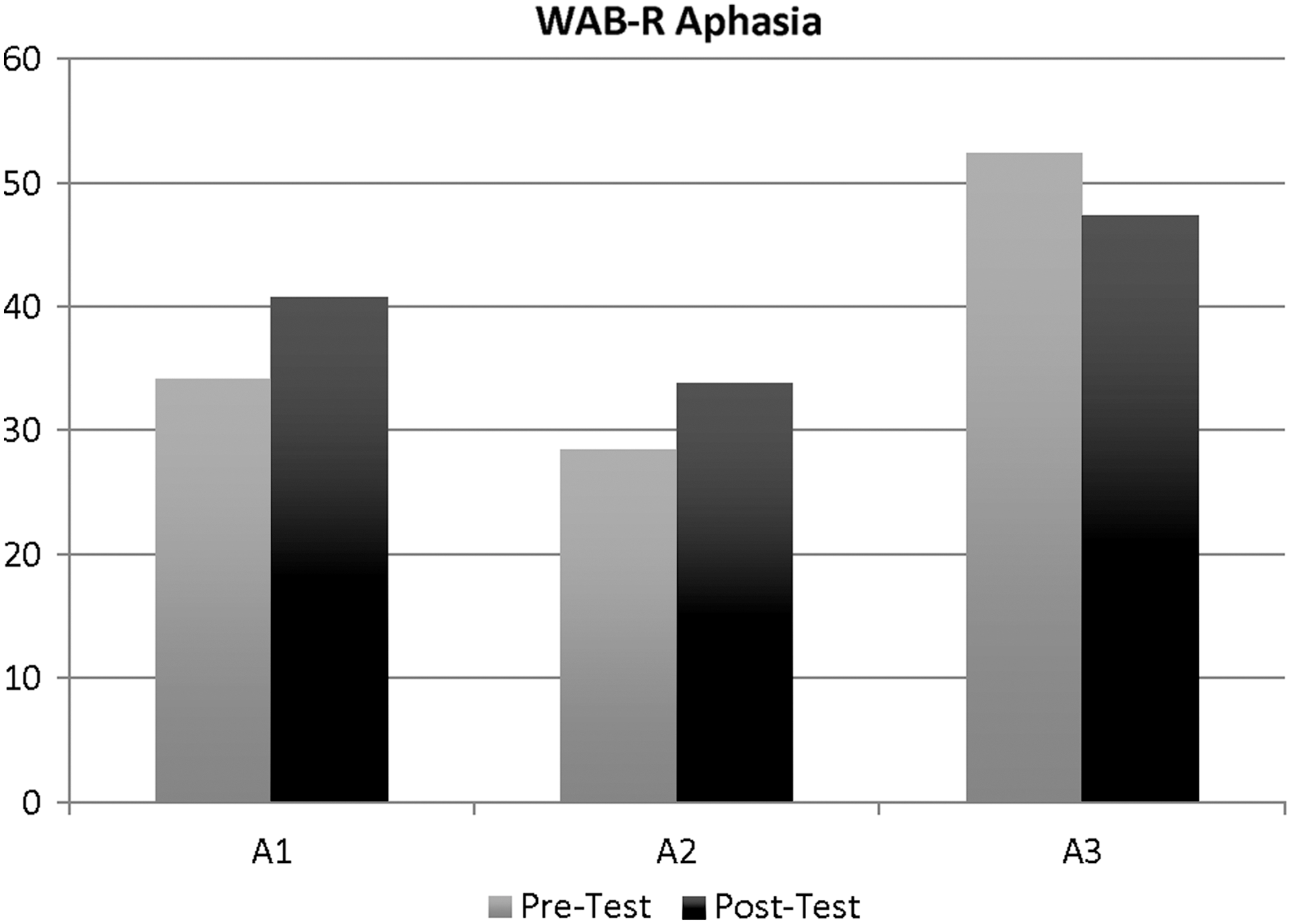
Western Aphasia Battery-R (WAB-R) aphasia quotients for all three participants.
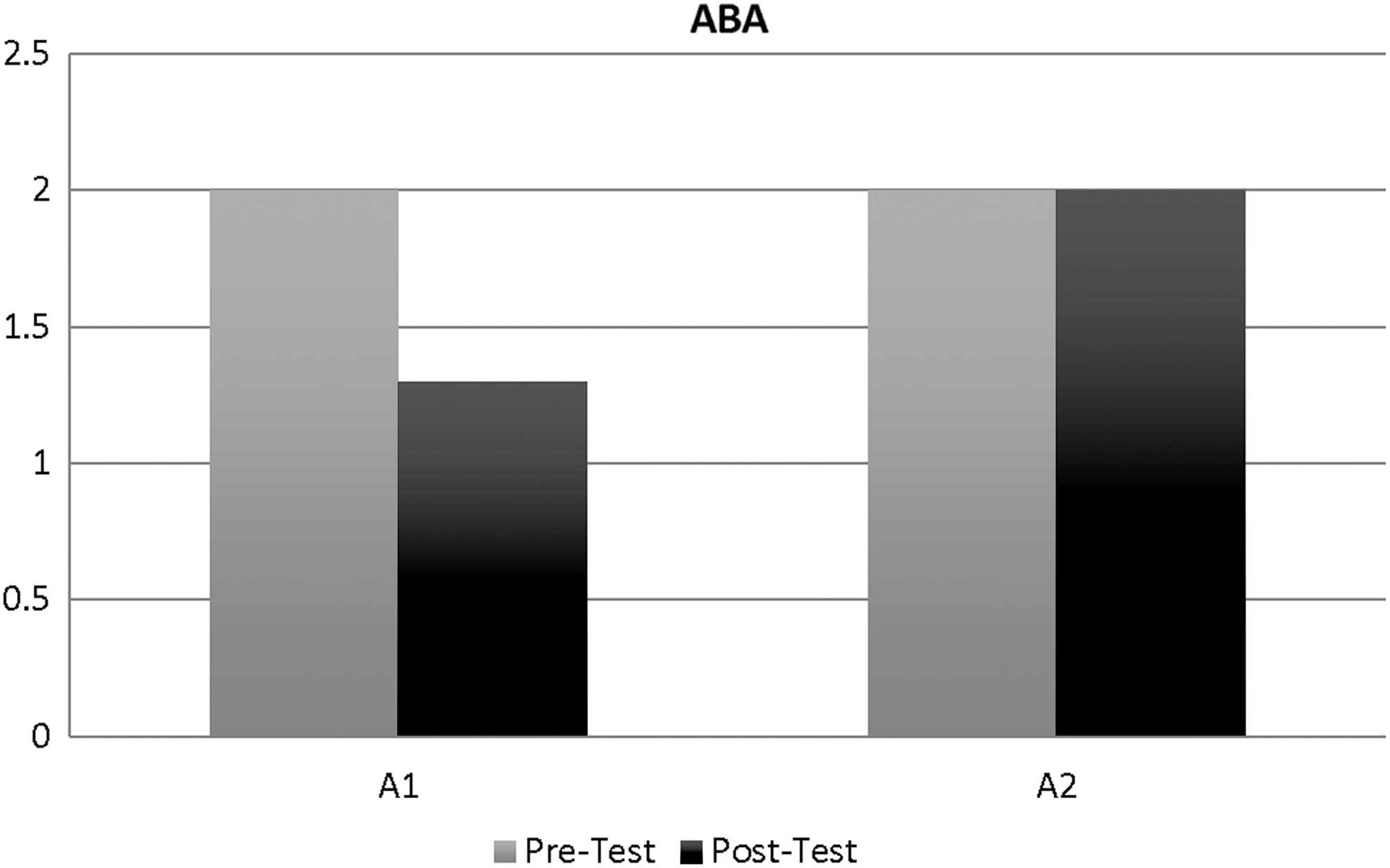
Apraxia Battery for Adults (ABA) scores for all three participants.
All dependent variables were recorded and graphed for each session. Movement between phases depended on relative observable stability of at least three data points. Overall, some change was observed for total number of CIUs and word productivity for two of the three participants. The attention measure (CTT) suggested that there was no marked improvement from baseline to treatment phase.
The individual results for the participants are as follows:
A1
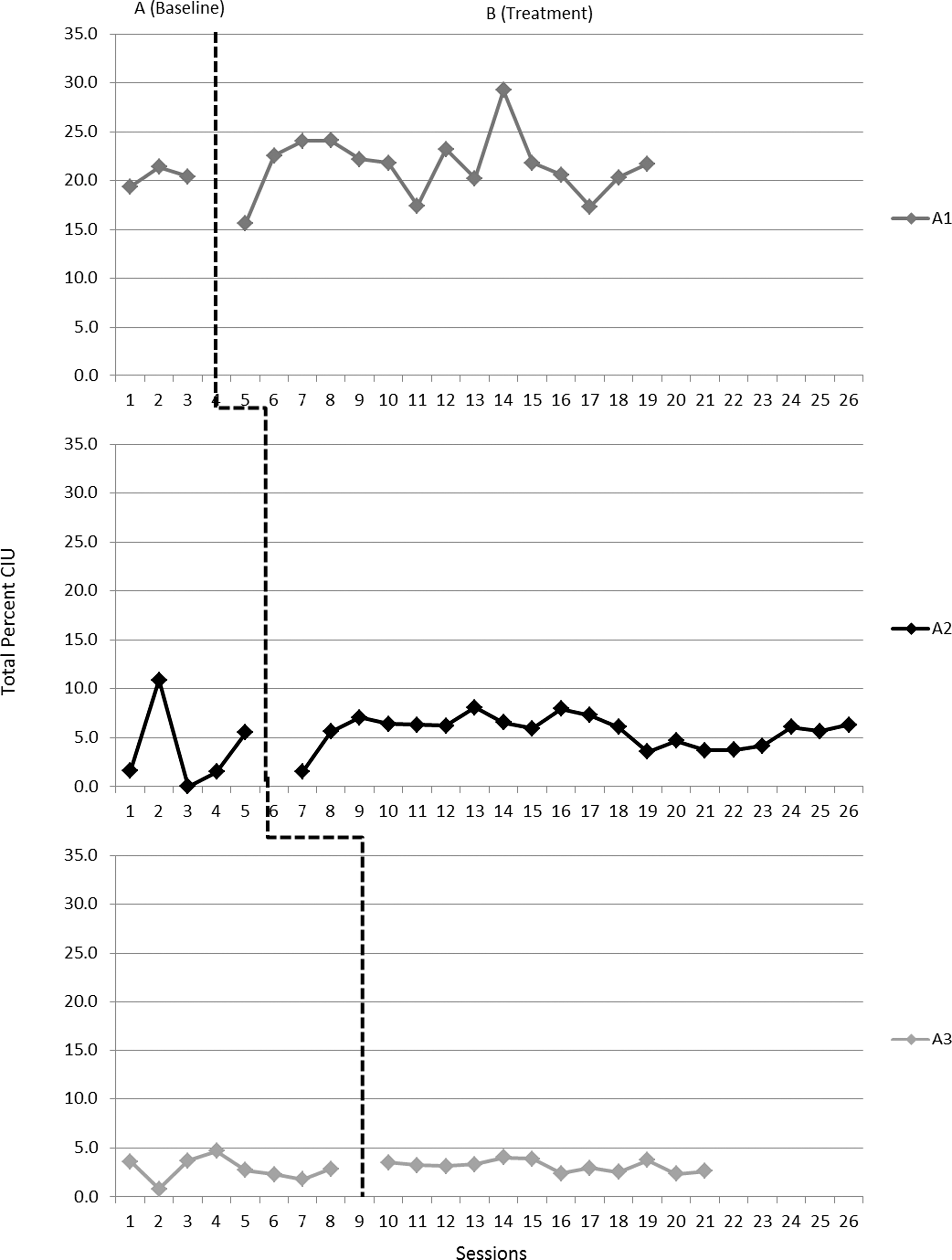
A1 participated in a total of 18 sessions (3 baseline, 15 treatment) over the course of 13 weeks. Descriptive comparison between pre- and post-test results showed that the WAB-AQ score improved slightly from 34.2 to 40.8 (Fig. 2) and apraxia severity decreased from moderate to mild-moderate as determined by the ABA-2 (Fig. 3). CADL-2 scores changed slightly, from 70 to 71 (Fig. 1). However, the participant's diadochokinetic rate improved from a maximum of 2 during the baseline phase to a maximum of 9 during the treatment phase (Fig. 4). With regard to the language and attention assessments, no improvements were noted. The participant produced an average of 3.24 CIU/min during the baseline phase and 3.42 CIU/min over the last four treatment sessions (Fig. 5). The number of productive words was calculated to be an average of 6.98 per minute during baseline and 4.02 per minute during the last four treatment sessions (Fig. 6). Percentage CIUs, percentage word productivity, and CTT scores showed no change via visual inspection (Fig. 7). For A1's participant-specific assessment, she was asked to read 10 words randomly chosen from a bank of 50 words. Whole words correct and percentage of phonemes correct were scored. Neither showed improvement.

Diadochokinetic rates for participants A1 and A2 across phases and sessions.
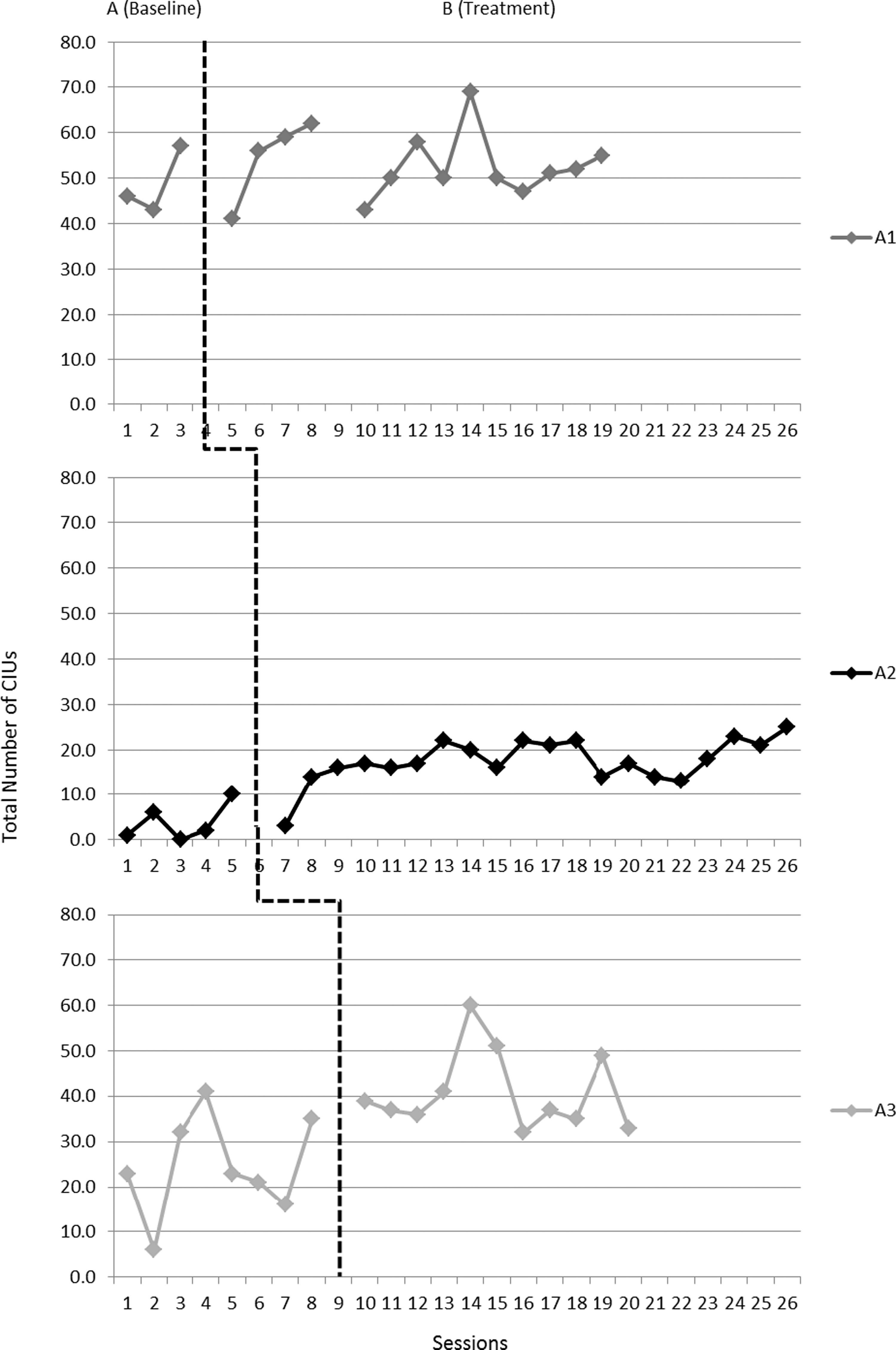
Total number of Correct Information Units (CIUs) for participants across phases and sessions.
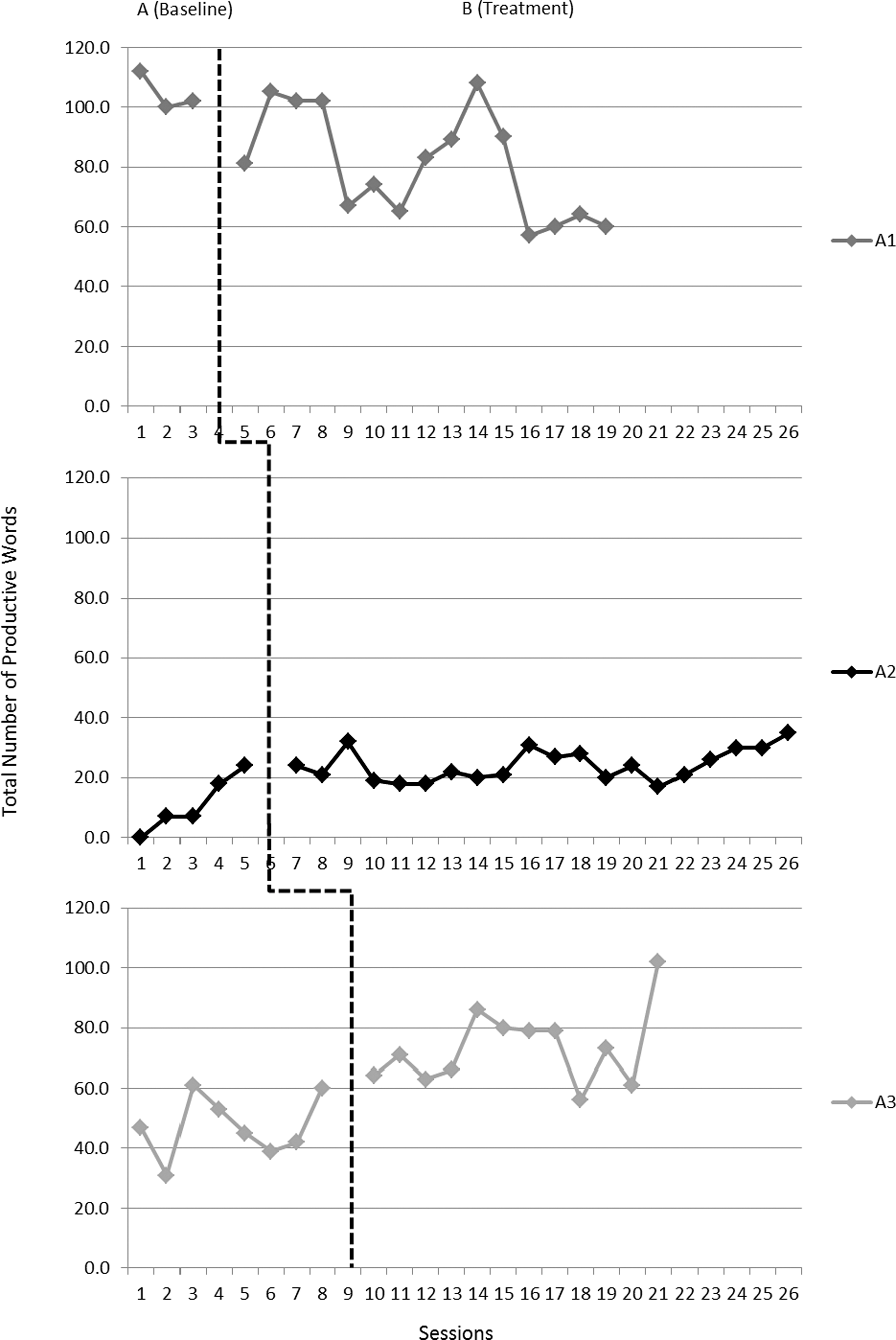
Number of productive words for all participants across sessions and phases.
Percentage Correct Information Units (CIUs) for all participants across sessions and phases.
A2
A2 participated in a total of 25 sessions (5 baseline, 20 treatment) over 14 weeks. Descriptive comparison between pre- and post-test results showed an improvement in functional communication skills, as measured by CADL-2 scores of 59 to 70 (Fig. 1), as well as a slight improvement in WAB-AQ scores of 28.4 to 33.8 (Fig. 2). Severity of apraxia did not change, as shown by the ABA scores (Fig. 3), while diadochokinetic rates improved as the rate steadily increased throughout the study (Fig. 4). Finally, visual inspection revealed an increase in the total number of CIUs (Fig. 5) and total number of productive words (Fig. 6) with treatment. The participant produced an average of 0.25 CIU/min during the baseline phase and 1.45 CIU/min over the last four treatment sessions. Word productivity was calculated to be an average of 0.75 productive words per minute during baseline and 2.02 productive words per minute during the last four treatment sessions. However, percentage CIUs (Fig. 7), percentage productive words, and CTT scores did not improve. A2's participant-specific assessments consisted of completing steps 4 and 5 of Rosenbeck's 8-Step Continuum. 31 No improvement was identified through visual inspection.
A3
A3 participated in a total of 20 sessions (8 baseline, 12 treatment) during 15 weeks. Descriptive comparison between pre- and post-test results showed a slight improvement in functional communication skills, as measured by CADL-2 scores increasing from 61 to 65 (Fig. 1); however, WAB-AQ showed an increase in severity from moderate to severe with scores of 52.4 and 47.3 (Fig. 2). With regard to the language measures, visual inspection revealed an increase in the total number of CIUs (Fig. 5) and total number of productive words (Fig. 6) after combined therapy techniques were introduced. The participant produced an average of 1.64 CIU/min during the baseline phase and 2.62 CIU/min over the last four treatment sessions. Word productivity was calculated to be an average of 3.15 productive words per minute during baseline and 4.87 productive words per minute during the last four treatment sessions. Percentage CIUs (Fig. 7), percentage word productivity, and attention assessments did not improve. A3's participant-specific assessments consisted of confrontational naming of 20 total items. Items included both trained (targeted during conventional treatment) and untrained (not targeted during conventional treatment) items. The participant showed no consistent increased performance from baseline to treatment phase for either trained or untrained items.
Discussion
This study sought to determine whether adults with aphasia could be taught UFNB, whether UFNB could be used along with simultaneous traditional speech-language therapy, and what the combined therapy outcome would be. Additionally, because two of the participants had apraxia of speech, this study explored the effect of this combined approach on motor speech skills. Findings suggest that adults with aphasia can learn UFNB and use it successfully while participating in traditional therapy. Furthermore, functional communication scores for two of the three participants increased (Fig. 1), as did the diadochokinetic rate in participants A1 and A2. These changes are clinically significant for individuals with aphasia. Unfortunately, no consistent improvement of aphasia severity or attention skills was found in the three participants. In the language samples, both A2 and A3 demonstrated an increase in total number of CIUs and total productive words.
The most encouraging findings from this study involve the improvement of functional communication, discourse, and diadochokinetic rates. Regarding diadochokinetic rates, no previous literature suggests that motor skills improve with the use of UFNB. Of note, no interventions received by the participants with AOS targeted diadochokinetic rates. Because UFNB arguably increases blood flow in the contralateral hemisphere, damaged areas associated with apraxia of speech may benefit from this technique. Further, the relaxing effects of UFNB may counteract the muscle tension that can accompany AOS, which could lead to better performance on speech motor tasks, such as diadochokinesis. Additionally, combined UFNB and speech-language pathology treatment appears to benefit functional and discourse-level communication. Such a finding suggests that this inexpensive technique may hold promise for some aspects of language production and comprehension, although further research is needed.
Attention skills did not improve as predicted, which revealed some potential for change with attention and UFNB after stroke. 4,42 The current study used the standard attention test (CTT) to capture change in attention. However, previous studies used the Connors Continuous Performance Test (CPT-II). A test emphasizing more discrete aspects of attention might reveal changes, such as those used in studies of nonclinical populations. 18
Limitations of the current study include the fact that one participant had chronic global aphasia. This participant showed no improvement on many aspects of language. Language skills associated with certain types or severities of aphasia may be more amenable to UFNB. Furthermore, because of the single-subject design, the individuals may be demonstrating practice effects, which could be influencing the results of the study. Future research could use a controlled waitlist design to determine whether statistically significant effects exist between a group receiving only speech-language treatment and those receiving both UFNB and speech-language treatment. Further, it would allow a more detailed analysis of the amount of UFNB completed and the potential changes observed.
Conclusion
Research and clinical implications for this study suggest that UFNB is teachable to patients with aphasia. Furthermore, UFNB appears to have resulted in clinically significant changes and benefitted overall language production and functional communication when it was paired with traditional therapy. Overall, UFNB holds promise for individuals with aphasia (and potentially adults with apraxia of speech) and should be evaluated further because of its low cost and flexibility. Although certain areas improved for these three participants, more research is needed to better understand the potential benefits of yogic breathing tasks and how they may be applied to individuals with aphasia.
Footnotes
Acknowledgment
Thanks to all of the participants who gave generously of their time and the anonymous reviewers who gave their helpful suggestions.
Author Disclosure Statement
No competing financial relationships exist.