
Abstract
Objectives:
A randomized controlled trial (RCT) and an extension trial of qigong (Chaoyi Fanhuan qigong [CFQ]) in patients with fibromyalgia were recently completed. In the present study, a qualitative analysis of comments from the RCT was undertaken using motivation and amount of practice to determine whether initial experiences provided information relevant to outcomes.
Intervention:
Participants in the RCT received instruction in qigong (level 1 CFQ), practiced 45 min/day for 8 weeks and continued practice to 6 months; open-ended qualitative comments on experiences were invited at 8 weeks and 4 and 6 months. Extension trial participants received further instruction (level 2 CFQ) and practiced regularly for 8 weeks–6 months. Comments from the original RCT were considered as narratives for the extension trial subgroup (n=20) and thematically, according to amount of practice, for all participants who completed the RCT (n=73).
Results:
Narrative comments from the RCT for those who completed the extension trial (n=13) and those who withdrew from that trial (n=7) were considered separately. Participants reporting benefits within the first 8 weeks were more likely to maintain practice and report continued benefits at 4–6 months than those who withdrew from the trial. Thematic comments for all who completed the RCT (n=73) were considered in relation to amount of practice (per protocol, intermediate, minimal). Participants who practiced per protocol during the initial 8 weeks (≥5 hours/wk) were more likely to maintain practice over 4–6 months and to report beneficial health effects from qigong.
Conclusions:
This retrospective qualitative analysis of information collected in an RCT of qigong for fibromyalgia indicates that favorable initial experiences with the practice over 8 weeks predispose to continued practice and more health effects. Future individual trials and meta-analyses of qigong will need to attend to the amount, and potentially quality, of practice undertaken in considering trial outcomes.
Introduction
Q
There are now several reports of sustained benefits (4–6 months) of regular qigong practice (over 6–12 weeks) in fibromyalgia, a chronic pain condition associated with sleep disturbances, fatigue, and decreased quality of life. 10 –13 In Halifax, Nova Scotia, Canada, the authors have completed several trials of a single form of qigong (Chaoyi Fanhuan qigong [CFQ]) 14 —a pilot trial, 15 a randomized controlled trial (RCT), 12 and an extension trial involving a subset of RCT participants 16 —and this body of investigation allows for more detailed exploration of issues related to the health potential of qigong practice. The RCT reported quantitative measures for pain, impact, sleep, and physical and mental function, and there were significant improvements in all scores that were maintained to 6 months. 12 The extension trial undertook a quantitative and qualitative analysis, and the juxtaposition of the two approaches provides valuable insight into long-term effects of qigong practice for fibromyalgia. 16 In both trials, there was a relationship between extent of practice and outcomes, with more favorable results occurring in patients who practiced diligently (45–60 min/day for 8 weeks). Both trials required considerable dedication on behalf of participants, and completion rates were 73% (RCT) and 65% (extension) at 6 months. It is recognized that this practice will not be for everyone, for many reasons, so it is important to attend to factors that predispose to successful outcomes.
The current study entailed a retrospective subgroup analysis of qualitative comments of participants in the RCT, 12 with clustering around motivational factors (those who entered the extension phase) and extent of practice (self-reported practice times). The general hypothesis being considered is that benefit is related to amount of practice. These comments provide valuable supplementary information to the quantitative data already reported and insight into patient experiences with an emerging practice that holds promise for improving health outcomes in a challenging chronic pain condition.
Materials and Methods
The RCT was conducted between September 2009 and July 2011 at the Pain Management Unit, Queen Elizabeth II Health Sciences Centre, Halifax, and was approved by the Research Ethics Board. 12 Participants (n=100) were randomly assigned to an immediate qigong training group or to a wait list control group (usual care) and then received qigong training at the end of the wait time. Participants received training in level 1 CFQ, 14 a form of qigong that is available locally, over 3 half-days, attended weekly practice sessions (where instruction was refined), and were expected to practice 45 min/day for 8 weeks; they were then encouraged to continue regular practice to 6 months. Training consisted of instruction in 7 movements that are loose and gentle and performed with attention to body feeling; a set consists of 10 repetitions of movements 1–5 and 5 repetitions of movements 6–7 and takes 10–12 minutes to complete. Quantitative data for pain (numeric rating scale), impact (Fibromyalgia Impact Questionnaire), sleep (Pittsburgh Sleep Quality Index), and physical and mental function (Medical Outcomes Study Short-Form Health Survey) were collected at baseline, 8 weeks, 4 months, and 6 months. Quantitative data were analyzed separately for the immediate and delayed practice groups compared with the wait list group and as a combined qigong group compared with the wait list group. 12
The extension trial was conducted between March and September 2012, wherein 20 participants received additional level 2 CFQ instruction (sitting, standing, and lying meditation) and practiced 45–60 min/day for 8 weeks and beyond to determine whether additional benefit could be derived from further instruction and practice. Quantitative and qualitative results from the extension trial were reported recently. 16
Qualitative comments in the RCT were recorded by using a questionnaire that invited open-ended comments on experiences at baseline (first training session), 8 weeks (final practice session), and 4–6 months (returned by mail). (At 8 weeks: “Describe changes in your health over the past 8 weeks that you attribute to qigong practice.” At 4–6 months: “Describe changes in your health since entering the study that you attribute to qigong practice.”) Qigong practice times were self-reported on these questionnaires. (“On average, how many hours per week have you practiced qigong since entering the study?”) Qualitative comments were considered as subgroups according to (1) motivation (those entering the extension trial were considered highly motivated; this is a presumption, and other factors could contribute) and (2) practice time (quantitative outcomes were related to extent of practice in the RCT and extension trial).
Two types of analyses were undertaken. Thus, comments were considered as narratives in which experiences over time were reported for extension trial participants (n=20; completers and noncompleters), as well as in themes of pain, sleep, and quality of life for participants who completed the RCT (n=73; stratified according to practice times). Comments were abbreviated but retain original phrasing used by participants. Following compilation, an independent reviewer checked extracted information against original comments to ensure that these accurately reflected information recorded by trial participants.
Practice times for the per protocol, intermediate, and minimal practice groups were compared using analysis of variance with Dunn post hoc comparison (Sigma Plot 11.0, Systat Software, Inc., San Jose, CA).
Results
The RCT involved 100 participants (96% female) with a mean age of 52 years and fibromyalgia duration of 9.6 years; 73 (73%) completed the trial to 6 months. The extension trial involved 20 participants (100% female) with a mean age of 53 years and fibromyalgia duration of 11.5 years; 13 (65%) completed this trial to 6 months. Quantitative measures for pain, sleep, impact, and physical function were significantly improved in both trials. 12,16 Figure 1 indicates the disposition into subgroups of the 73 sets of qualitative comments from the RCT. Table 1 indicates self-reported practice times for subgroups. The per protocol group refers to those who practiced 45 min/day for 8 weeks (≥5 h/wk); other divisions are arbitrary but are intended to identify minimal practice (≤3 h/wk) and intermediate groups (>3–<5 h/wk).
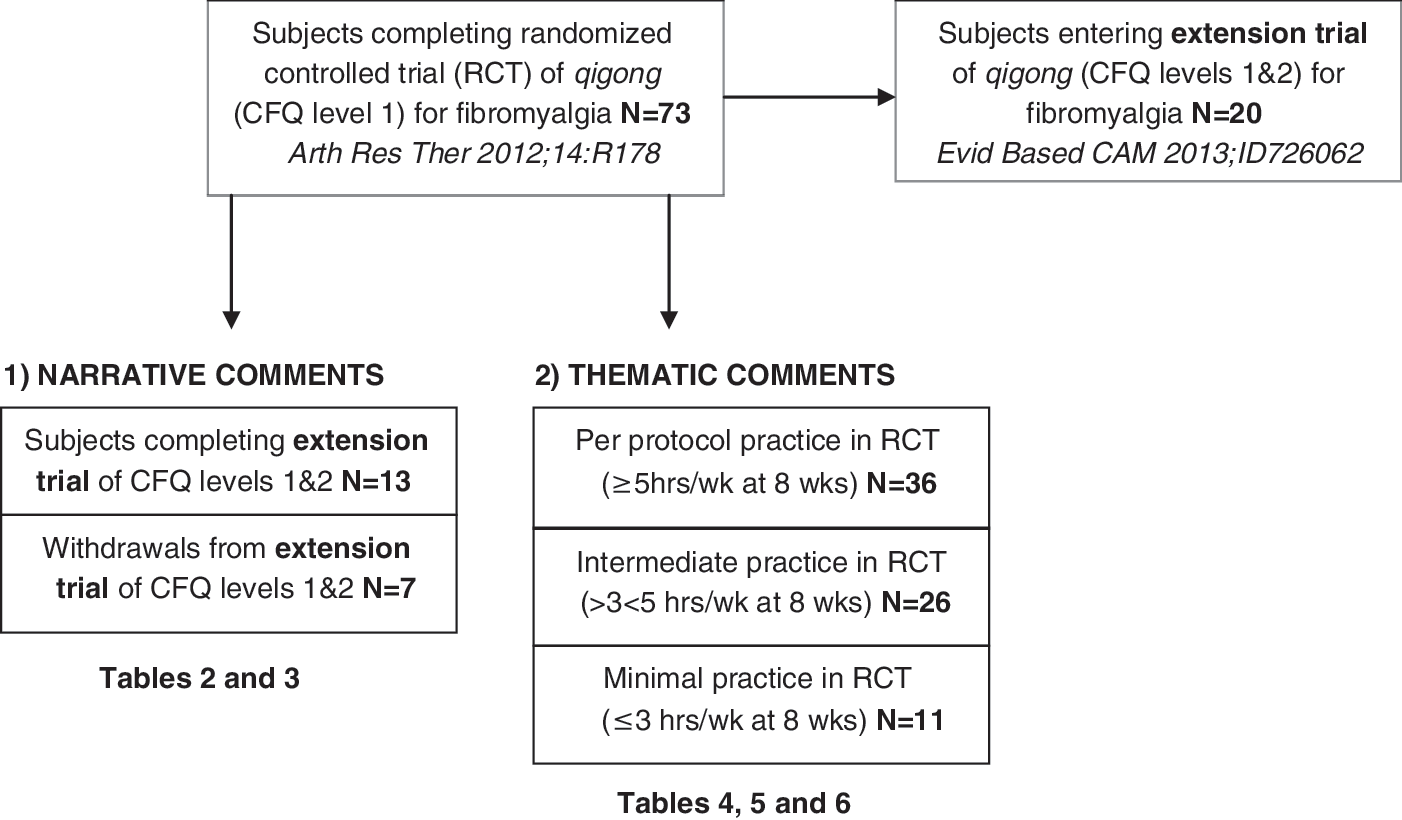
Subgroups of those completing a randomized controlled (RCT) trial of qigong for fibromyalgia in which qualitative comments are considered as narratives or themes. CFQ, Chaoyi Fanhuan qigong.
Values are expressed as mean±standard deviation.
p<0.05 compared to per protocol group.
p<0.01 compared to per protocol group.
RCT, randomized controlled trial.
Narrative qualitative comments
Narrative comments for the subset of participants completing the extension trial (n=13) are presented in Table 2. These refer to benefits in quantitative scores reported previously and include comments on pain (007, 019, 029, 042, 043, 075, 087, 091, 098), sleep/fatigue/energy (006, 007, 019, 029, 042, 043, 075, 087, 091, 098), and relaxation/reduced stress/improved mood (006, 007, 029, 042, 019, 043, 044, 048, 075, 087, 098). Additional benefits include improvements in allergies (006, 007, 098), better chemical tolerance (006,098), reduction in pain medication (019), improvements in symptoms of muscular dystrophy (048), and improvement in blood pressure (075). Some mention increased pain (006, 019, 036, 042, 091). One participant reported an incident of pain “returning with a vengeance” for an interval and then dissipating (019), while another suggested that qigong uncovered health issues (042).
CFQ, Chaoyi Fanhuan qigong; FM, fibromyalgia; TMJ, temporomandibular joint.
Narrative comments by those who withdrew from the extension trial (n=7) are presented in Table 3. There are some favorable comments about pain (004, 005, 060), sleep/fatigue/energy (004, 005, 025, 060, 082), and relaxation/reduced stress/improved mood (025, 082, 089). Some comments mention continued pain (004, 089). Additional benefits attributed to practice included gastrointestinal effects (004, 060) and improved breathing (025). Comments were more moderate in tone than comments by participants who completed the extension trial. Those who withdrew from the extension trial had similar, but somewhat lower, practice times compared with those who completed the extension trial in the earlier RCT (Table 1).
Thematic qualitative comments
Thematic qualitative comments for all who completed the original RCT are presented in Tables 4 –6. Comments are clustered around themes of pain, sleep, and impact/quality of life/other, and are stratified according to practice times of per protocol (≥5 h/wk at 8 weeks, continued practice of 2–4 h/wk for 4–6 months) (Table 4), intermediate practice (>3–<5 h/wk at 8 weeks, some practice over 4–6 months) (Table 5), and minimal practice (≤3 h/wk at 8 weeks, variable practice over 4–6 months) (Table 6). Self-reported practice times for these subgroups are presented in Table 1; practice times significantly differed between groups.
CNS, central nervous system.
Quantitative outcomes for participants who practiced per protocol were statistically better than for those who practiced minimally. 12 Perusal of comments in Table 4 and Table 6 generally reflects these differences. For those who practiced per protocol, reports on pain experiences were richer than can be conveyed by a single numeric score and contain temporal sequences that are part of the experience of chronic pain (Table 4). Participants who practiced minimally report some positive effects on pain, but there is a clear difference in the tone of comments (Table 6). With respect to sleep, there are many favorable comments in the per protocol group (Table 4) but little sense of benefit in the minimal practice group (Table 6). Impact/quality of life and other comments reveal marked changes in health for the per protocol group (Table 4) and little impact in these areas with minimal practice (Table 6).
Quantitative results for the subgroup that practiced an intermediate amount of time were not previously considered separately, 12 recognizing potential imprecision of self-reporting and the arbitrariness of categories. In the present clustering, qualitative comments for this subgroup indicate there are positive effects perceived to result from qigong practice (Table 5), but there is a more moderate tone to these comments than in the per protocol group (Table 4).
Discussion
Underlying principles of qualitative analysis
This study undertook a retrospective analysis of qualitative comments from a RCT in which 73 participants with fibromyalgia undertook regular qigong practice for 8 weeks, continued practice and completed the trial to 6 months, and reported significant health gains in core domains for fibromyalgia. 12 Qualitative content analysis can take different forms, and the approach used will reflect theoretical perspectives on the issue of study. 17 The present retrospective viewpoint was structured around two features: motivation and practice time. (1) Motivation: A subgroup of those who completed the original trial went on to enter an extension trial in which instruction was added (level 2 CFQ) and further diligent practice was engaged (60 min/day for 8 weeks, practice encouraged for 6 months). 16 (2) Practice time: In both the RCT and the extension trial, outcomes were related to extent of practice, whereby more favourable outcomes were associated with more practice. 12,16 An underlying principle for the current analysis was the recognition that qigong practice requires diligence and that it may not be suitable for all individuals, for many reasons. The current analysis sought to determine whether information in this set of qualitative responses might be helpful for predicting favorable outcomes and for advising patients in terms of self-care practices that might assist in managing fibromyalgia. This is a difficult condition to treat 18 and is a challenge both for patients who experience it and physicians who treat it. 19 Complementary therapies need to be explored. 20 –22
Motivation and extent of practice
A subset of those who completed the RCT went on to enter the extension trial (n=20), which required further diligent qigong practice, and those who completed the extension trial (n=13) reported prominent and sustained health benefits. 16 Within that group was a further subgroup who had voluntarily undertaken additional CFQ training following completion of the RCT and before entering the extension phase (n=5). That group had the most improvement in fibromyalgia symptoms and reported benefits in other areas (asthma, food allergies, respiratory allergies, chemical sensitivities, improved eyesight, improved mood). Because of the way in which the two trials unfolded (the extension trial was undertaken because it was known that further health benefits were occurring), these participants had practiced qigong for 2–3 years. The prominent health benefits with long-term practice of qigong reported in the extension trial are similar to health gains described in some who undertake extensive community-based practice. 23
In the current qualitative analysis, the 13 extension trial completers differ in their initial experiences within the RCT from the 7 who withdrew from the extension trial in terms of more positive outcomes (Table 2 vs Table 3). Those who withdrew from the extension trial self-reported only somewhat lower practice times than those who completed the trial during the initial RCT (Table 1), raising the issue of fidelity/effectiveness of practice or limits of self-reporting methods (see next section). Those who entered the extension trial included 10 (50%) per protocol, 9 (45%) intermediate practice, and 1 (5%) minimal practice participants from the original RCT; most of those who completed the extension trial (9 of 13 [69%]) had practiced per protocol in the original RCT. It appears that experiences within the first 8 weeks of exposure to qigong are important, with more favorable experiences during this initial time predisposing to continued practice and benefit. In future studies, it will be important to prospectively assess motivational and other factors that predispose to more favorable outcomes with qigong practice.
Within the initial RCT, experiences are also clearly related to extent of practice. This was demonstrated statistically in quantitative scores in core domains for fibromyalgia 12 and is also reflected in qualitative comments when comparing per protocol and minimal practice groups (Table 4 vs Table 6). The intermediate group was not analyzed statistically with respect to quantitative scores previously, but qualitative comments indicate many positive experiences related to core domains in fibromyalgia that are attributed to qigong practice (Table 5). There are however, more qualifications offered and more equivocal presentations of experiences. The intermediate group practiced significantly less than did the per protocol group, especially during the 4- to 6-month follow-up time (Table 1). Although the method of self-reporting practice time has limits, this post hoc distinction does reveal associations between outcomes and amount of practice.
Implications for research
Qigong is currently considered to be mindful exercise or meditative movement, 1,9 and there is growing interest in exploring the health potential of the practice. There are challenges inherent in conducting research into qigong and related practices, 9,24 –26 and several observations in the present study are relevant to methodology. With respect to “dosing,” how much practice is needed, and for how long, protocols of 6–12 weeks with variable practice times are generally used. Whether the protocol is sufficient or optimal also is not clear; protocols are often based on pilot studies or prior trials, but few studies have explored the issue of the most efficacious regimen. There is the further issue of adherence; group practice time can be regulated, but individual home practice relies on motivational/adherence factors. Another issue is “fidelity of practice” or “bioavailability”—that is, whether all time devoted to practice is effective time. The current analysis provides information relating to amount of practice (see above) and potentially additional insight. Thus, differences in qualitative reports in the RCT between participants who completed or withdrew from the extension trial were noticeable despite similar self-reports of practice times. This suggests that there are indeed differences in effectiveness between groups (assuming self-reported times are somewhat accurate). With mindful or meditative practices, monitoring effective engagement of the practice has been attempted by developing specific tools (e.g., meditative movement inventory 27 ), but this approach is not validated or widely used. In view of the relation between practice time and outcomes observed in the present analysis, it is recommended that future studies of qigong consider issues of “dosing” and “fidelity/bioavailability” in relation to design and interpretation of outcomes.
Meta-analysis and systematic analysis of larger data sets also need to attend to the issue of practice time. For example, recent meta-analyses of qigong for fibromyalgia came to cautious conclusions on its merit. 28 –30 These analyses clustered studies in which qigong was part of weekly group sessions for 8–12 weeks 31 –33 with those in which it was practiced daily for 6–8 weeks 10 –12 but made little distinction between such studies. Qigong practiced daily for 12 weeks also leads to improvements in chronic fatigue syndrome, 34 which is a condition related to fibromyalgia. 35 Collective analysis of qigong in all research areas will need to address amount of practice.
Summary and conclusions
Both quantitative and qualitative approaches indicate that qigong is a promising self-care practice for management of fibromyalgia, especially when practiced diligently over time (daily for 8–12 weeks, regular practice for 6–12 months). Furthermore, in view of health benefits in other areas reported in qualitative assessments, exploration of the benefits of qigong practice in other conditions is encouraged. Benefits do appear related to amount of practice, and it will be particularly important to determine which factors predispose to (e.g., locus of control, attitudes toward complementary practices, psychological characteristics) or hinder (nature of qigong instruction, unclear optimal protocols, matching protocols to particular needs) qigong practice.
Footnotes
Acknowledgments
This study was funded by a Pfizer Neuropathic Pain Research Award. The authors thank Chok Hiew and Dana Marcon for qigong instruction in the original RCT of qigong for fibromyalgia. They also thank Allison Reid for editorial assistance and for independently checking abbreviated comments against original comments.
Author Disclosure Statement
No competing financial interests exist.