
Abstract
Objective:
This meta-analysis was conducted to evaluate the efficacy of acupuncture on cognitive impairment (function) after a stroke.
Design:
Randomized controlled trials (RCTs) comparing acupuncture with no acupuncture in addition to medicine or rehabilitation were identified from databases (PubMed, Cochrane Central Register of Controlled Trials, Chinese National Knowledge Infrastructure, VIP Chinese Periodical Database, Wangfang Chinese Periodical Database, Chinese Bio-medicine Database, Cochrane Library, and Chinese medical literature databases) and two relevant journals (Chinese Acupuncture and Moxibustion and the Journal of Shanghai Acupuncture and Moxibustion). Meta-analyses were conducted for the eligible RCTs.
Results:
Twenty-one trials with a total of 1421 patients met inclusion criteria. Pooled random-effects estimates of the change in the Mini-Mental State Examination were calculated for the comparison of acupuncture with no acupuncture in addition to medicine or rehabilitation. Following 4 weeks and 8 weeks of intervention with acupuncture, the merged mean difference was 3.14 (95% confidence interval [CI], 2.06–4.21; p<.00001) and 2.03 (95% CI, 0.26–3.80; p=0.02), respectively. For the comparison of 3–4 weeks of acupuncture with no acupuncture in addition to medicine or rehabilitation groups, the merged MD in Neurobehavioral Cognitive State Examination total scores was 5.63 (95% CI, 3.95–7.31; p<.00001). For the comparison of 8–12 weeks of acupuncture with no acupuncture in addition to medicine or rehabilitation groups, the P300 latency merged MD was −12.80 (95% CI, −21.08 to −4.51; p<.00001), while the P300 amplitude merged MD was 1.38 (95% CI, 0.93–1.82; p<.00001). Overall, the study quality was rated as moderate on the basis of the Cochrane Handbook for Systematic Reviews of Interventions (part 2: 8.5).
Conclusions:
This meta-analysis suggests that acupuncture had positive effects on cognitive function after stroke and supports the need for additional research on the potential benefits of this therapeutic approach.
Introduction
S
To date, the definition and classification of cognitive impairment vary across studies. Cognition typically includes domains such as attention and concentration, memory, and executive function; 4 some researchers also include visual-spatial perception and apraxia as cognitive impairments. 5 Including patients who remain cognitively intact after an index stroke, hospital-based and population-based studies 6,7 have revealed a significant risk of developing delayed dementia. However, physical handicaps often produce more profound symptoms compared with cognitive deficits following a stroke, and individuals who display slight cognitive deficits generally do not receive treatment. Considering that 40% of survivors are not able to take care of themselves, these cognitive deficits not only bring pain to the patients but also burden their family and society.
Stroke rehabilitation techniques develop rapidly. The World Health Organization 8 reported that active rehabilitative therapy may help up to 60% of all surviving stroke victims to resume daily living activities without assistance; approximately 30% of working-age stroke survivors can return to work within 1 year after a stroke. In Western countries, treatments aimed at stroke rehabilitation typically include physiotherapy, occupational therapy, and speech therapy, in addition to the skilled medical and nursing care classified as conventional stroke rehabilitation. Considerable research efforts have focused on improving the many treatment technologies. However, no single rehabilitation intervention has been identified as unequivocally beneficial to recovery. This has led to more recent research on the use of other treatment approaches for stroke rehabilitation, such as acupuncture and Chinese herbal medicine.
Acupuncture is one of the most important treatments of Traditional Chinese Medicine and can be traced back more than 2000 years in China. 9 A relatively simple, cheap, and safe treatment compared with other conventional interventions, acupuncture has been accepted by Chinese patients and is widely used to improve the neurologic functions of patients who have had a stroke, including motor function, sensation, and speech. As a therapeutic intervention, acupuncture has also become more frequently used among Western countries. 10,11 The utility of acupuncture treatment remains under investigation, even with many lines of evidence supporting its use across diseases. Numerous studies 12 –15 support the clinical efficacy of acupuncture in stroke rehabilitation, especially in China; nevertheless, some conflicting evidence exists. 16 Systematic reviews of trials of acupuncture in stroke rehabilitation have been conducted, 13,17 –21 including trials on stroke patients in acute, subacute, or chronic stages. One recent systematic review conducted by a Chinese research group indicated that acupuncture appeared to be safe but did not provide any additional benefit to patients with acute stroke. 22
As a traditional therapeutic method, acupuncture therapy is a widely recognized alternative measure in current clinical practices. For decades, numerous clinical studies have evaluated the efficacy and safety of acupuncture in patients with cognitive impairment, more specifically with vascular dementia and cognitive impairment after stroke. Researchers designed randomized controlled trials (RCTs) to assess the efficacy of acupuncture on patients with cognitive impairment after stroke, but the results were inconsistent. Several review articles 23,24 have summarized the use of acupuncture in patients who have had a stroke. Most of these reviews have highlighted the potential role of acupuncture as a promising treatment for patients with cognitive impairment after stroke, but no conclusions regarding its efficiency were drawn.
No systematic reviews have specifically examined the efficacy and safety of acupuncture on patients with cognitive impairment after stroke. To evaluate the effectiveness and safety of acupuncture therapy for impairment after stroke, a systematic review and meta-analysis were performed. This review used a standardized classification of cognitive impairment in high-quality RCTs of the effects of acupuncture on cognitive impairment after stroke. The purpose of this review was to systematically analyze all RCTs of acupuncture for cognitive impairment after stroke, with the goal of providing evidence-based treatment for clinical practice and assisting with future research.
Materials and Methods
Inclusion and exclusion criteria
Included in this review were original reports published in Chinese or English that described acupuncture as an intervention and provided sufficient methodologic details and specific data on cognitive function. The inclusion criteria for this meta-analysis were as follows: (1) RCT, 2) comparison of acupuncture of any kind with no acupuncture, (3) stroke diagnosis confirmed by computed tomography or magnetic resonance imaging; and (4) cognitive impairment and disability measures that are internationally recognized or nationally approved by an academic body in China. If studies contained three experimental groups with only one group receiving acupuncture, the acupuncture group and one additional treatment group consistent with interventions from other studies were chosen. If there were three experimental groups with two acupuncture groups, a routine acupuncture group was chosen as the intervention group and the nonacupuncture treatment group was chosen as the control group.
Trials were excluded if they met any of the following criteria: (1) no control group included in the original article; (2) acupuncture used in both the treatment group and the control group; (3) standardized indices of curative effect or detailed results of treatment not included; and (4) comparison of the intervention group with the control group in addition to treatment methods other than acupuncture, such as drugs or other forms of Traditional Chinese Medicine.
Search strategy
Electronic literature searches were performed in eight databases from their inception to February 2012 (PubMed, Cochrane Central Register of Controlled Trials, Foreign Medical Journal Service, Foreign Evidence-based Medicine, Vip Chinese Periodical Database, Chinese National Knowledge Infrastructure, Wangfang Chinese Periodical Database, and Chinese Bio-medicine Database) and two relevant journals (Chinese Acupuncture and Moxibustion and the Journal of Shanghai Acupuncture and Moxibustion). The search featured a wide coverage of reports and prospective studies within the field in order to provide sufficient data for analysis.
The search terms used were “acupuncture/electroacupuncture/auricular acupuncture, cognitive” AND “stroke/CVA/cerebrovascular accident/cerebral infarction/intracerebral hemorrhage/cerebral embolism (acupuncture OR acu*), cognitive” AND “(stroke OR apoplexy OR CVA OR cerebrovascular attack OR cerebrovascular accident OR cerebrovascular* OR cerebral infarction OR cerebral hemorrhage OR cerebral*).” One reviewer also manually searched Chinese Acupuncture and Moxibustion (2008–December 2012) and Journal of Shanghai Acupuncture and Moxibustion (2008–December 2012), which referenced trials and review articles, as well as acupuncture conference proceedings in China.
To include as many reports as possible on cognitive impairment, the publication date range was not limited and included all years for each individual database.
Study eligibility
Information on patients, methods, interventions, outcomes, and results were extracted independently by two reviewers using a self-developed data extraction form. Disagreements were resolved by a third member or through discussion between reviewers. One researcher picked out duplications of these reports via NoteExpress and scanned the title and abstract of the citation retrieved by the selection search engine (first scanning). Another researcher then viewed the full text of all potentially eligible reports obtained, after which similar reports were marked as “suspicious duplications” and compared. If the similarity rate of these articles appeared at or above 80%, the report containing the most detailed information was included while the other articles were omitted. Disagreements between the two reviewers were resolved by the research team (Fig. 1).
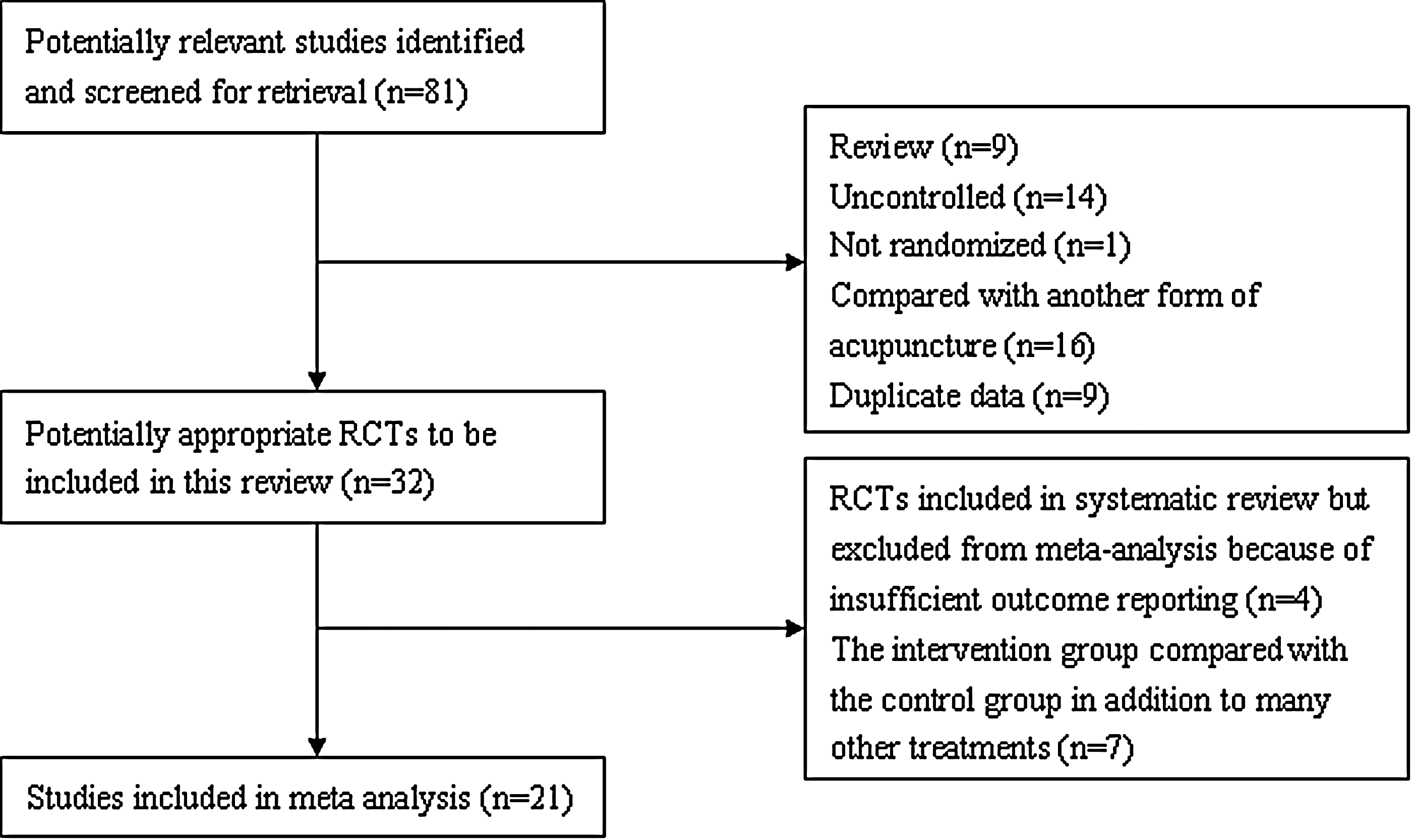
Study flow diagram of selection of randomized, controlled trials (RCTs).
Data extraction
Two researchers compiled a table listing the general information of the final included reports. The table listed the report title, journal name, year of publication, type of control, number of participants, and country of publication. Any missing information was coded as “not reported,” and disagreements were resolved by consulting related references before the table was finalized. Two reviewers scanned the full text of all 21 reports and compiled the relevant data (Table 1).
FNACCVD, Fourth National Academic Conference of Cerebral Vascular Diseases; CT, computed tomography; MRI, magnetic resonance imaging; CECS, Chinese expert consensus standards, proposed in 2005 for the prevention and treatment of cognitive dysfunction; MMSE, Mini-Mental State Examination; HDS-R, Revised Hasegawa's Dementia Scale; MoCA, Montreal Cognitive Assessment; FCA, Functional Comprehensive Assessment; LOTCA, Loewenstein Occupational Therapy Cognitive Assessment; FIM, Functional Independence Measure; NIHSS, National Institutes of Health Stroke Scale; SECF, Scale of Elderly Cognitive Function; CDT, Clock Drawing Task; WMS, Wechsler Memory Scale; NCSE, Neurobehavioral Cognitive State Examination.
Recorded data contained study characteristics, patient characteristics, and outcomes. An internationally recognized examination of cognitive impairment is generally composed of the following assessments: the Mini-Mental State Examination (MMSE), the Neurobehavioral Cognitive State Examination (NCSE), the Wechsler Memory Scale (WMS), the Functional Comprehensive Assessment (FCA), the National Institutes of Health Stroke Scale (NIHSS), the Functional Independence Measure (FIM), the Scale of Elderly Cognitive Function (SECF), the Montreal Cognitive Assessment (MoCA), the Loewenstein Occupational Therapy Cognitive Assessment (LOTCA), the Revised Hasegawa's Dementia Scale (HDS-R), the Clock Drawing Task (CDT), and the cognitive potential P300. Among these methods listed, P300 is the late component of an event-related potential (ERP) in the cerebral cortex and reflects the functioning of the neurochemical systems involved in cognitive processes. 25
Statistical analysis
RevMan 5.02 (Cochrane Collaboration, Oxford, United Kingdom) was used to perform the meta-analysis. An odds ratio was used for enumeration data, and the weighted mean difference was used for continuous variables. For continuous data, two types of estimates were calculated. The measure of the treatment difference for any outcome was calculated as (1) the mean difference (MD) when the pooled trials used the same rating scale or test or (2) the standardized MD when the trials used a different rating scale or test. Both parameters were expressed with 95% confidence intervals (CIs). Heterogenous test results were expressed by using the random-effects model, and homogeneous test results were expressed with the fixed-effects model. Heterogeneous test results were analyzed with sensitivity and subgroup exploration. Homogeneity of weighted MD across studies was assessed by using the Cochrane Q statistic and the I 2 statistic. A significant Q statistic (p<0.10) or I 2 >50% indicated heterogeneity across studies. The Begg rank correlation test and Egger linear regression test with p<0.10 indicated statistical significance.
Methodologic quality
The quality of clinical research articles was assessed via reference to the Cochrane Handbook for Systematic Reviews of Interventions, part 2: 8.5 (Table 2). The tool book consists of seven specific domains: sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, and “other issues,” such as early termination of the study and group differences at baseline that would impede data analysis. Each domain was evaluated as having low risk of bias high risk of bias, or unclear risk of bias in accordance with the judgment criteria. For each entry, a “yes” answer indicated a low risk of bias, “no” indicated a high risk of bias, and “unclear” indicated an unclear or unknown risk of bias. All test data were merged with the terminal index to obtain a positive result.
Based on Cochrane Handbook for Systematic Reviews of Interventions, Part 2: 8.5.
Results
Characteristics of included trials
The 21 included trials 22,26 –30,45 –59 were conducted in China and included a total of 1421 patients ranging in age from 18 to 80 years. More male than female participants were included in 15 trials, while four trials did not describe the sex of the patients. 26–27,46,50 The treatment period ranged from 2 to 24 weeks. Treatment sessions varied from 28 to 120 sessions, and the frequency of the sessions ranged from five sessions per week to two sessions per day. The acupuncture interventions varied significantly across the 21 trials. Nine trials were conducted by manual stimulation only, and 12 trials were conducted by electrical stimulation only. Acupuncture point prescriptions were also not consistent. Five trials 24,28,47 –49 involved only scalp acupoints, one trial 29 contained only body acupoints, and the other trials contained both body and scalp acupoints. Moreover, in all included trials, the number of points varied considerably and the needle retention time ranged from 15 to 30 minutes.
The time interval between stroke onset and treatment varied. In 10 trials the time interval ranged from 48 hours to 1 month, and in nine trials, the time interval was 3 to 36 months. In two trials the time interval was unclear. 50,51
The internationally recognized examination of cognitive impairment consisted of the MMSE, NCSE, WMS, FCA, NIHSS, FIM, SECF, MoCA, LOTCA, HDS-R, CDT, and cognitive potential P300.
Summary of meta-analysis
MMSE
Four trials with a total of 116 patients 30,46,50,51 measured improved MMSE total scores after 4-week acupuncture treatment. Heterogeneous tests were performed on the four referred trials. For the comparison of 4-week acupuncture with no acupuncture in addition to medicine or rehabilitation group, the MMSE total scores (chi-square=4.69; p=.20; I 2 =36%) indicated that the included studies were of clinical and statistical heterogeneity. The fixed-effects model was adopted in the meta-analysis; the merged MD value was 3.14 (95% CI, 2.06–4.21). The tests for overall effect (Z=5.71; p<.00001) revealed a statistically significant difference between the test and control groups on the MMSE after 4 weeks of treatment (Fig. 2).
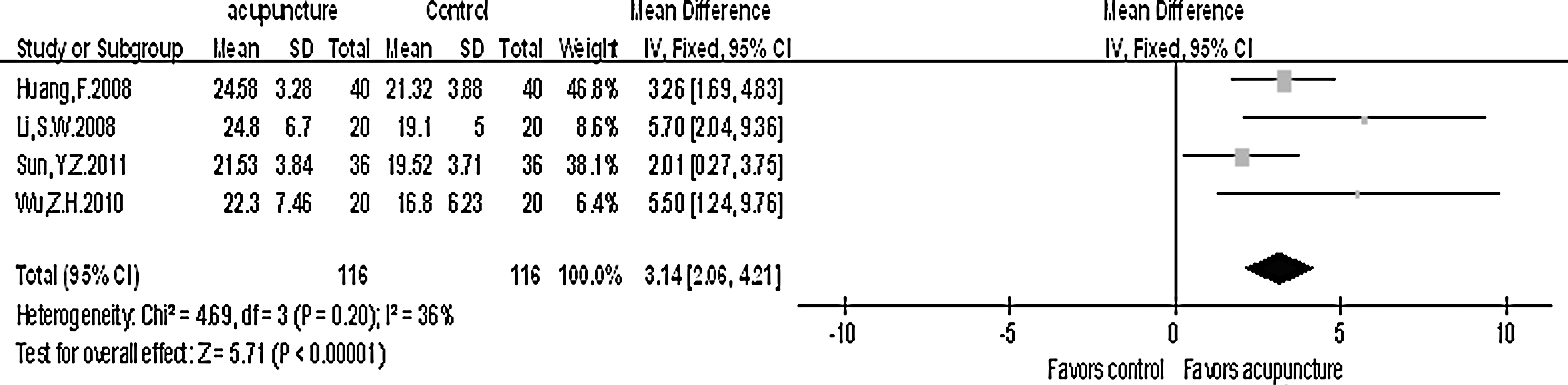
Mini-Mental State Examination total scores after 4 weeks of treatment. CI, confidence interval; SD, standard deviation.
Three trials with a total of 64 patients 47 –49 measured improved MMSE total scores after an 8-week acupuncture treatment. For the comparison of 8-week acupuncture with no acupuncture in addition to medicine or rehabilitation group, the MMSE total scores (chi-square=7.19; p=0.03; I 2 =72%) indicated that included studies were of clinical and statistical heterogeneity. The random-effects model was adopted in the meta-analysis; the merged MD value was 2.03 (95% CI, 0.26–3.80). The tests for overall effect (Z=2.25; p=0.02) revealed a statistically significant difference between the test and control groups on the MMSE after 8 weeks of treatment (Fig. 3).
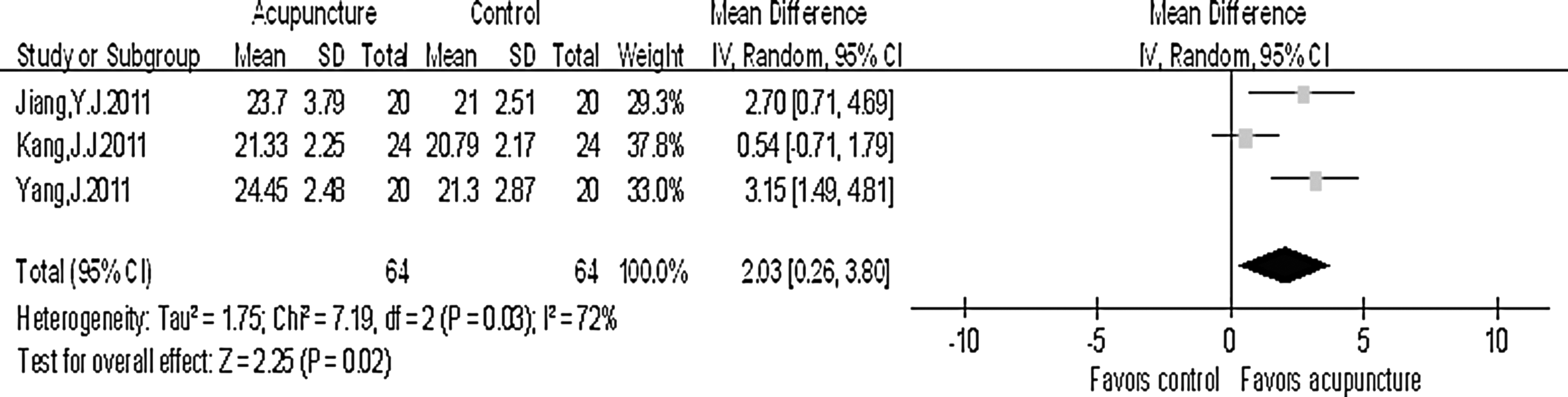
Mini-Mental State Examination total scores after 8 weeks of treatment.
NCSE
Two trials with a total of 61 patients 22,31 measured improved NCSE total scores after 3–4 weeks of acupuncture treatment. For the comparison of 3–4 weeks acupuncture with no acupuncture in addition to medicine or rehabilitation group, the NCSE total scores were compared (chi-square=0.35; p=0.56; I 2 =0%). The fixed-effects model was adopted in the meta-analysis; the merged odds ratio was 5.63 (95% CI, 3.95–7.31). The tests for overall effect (Z=6.58; p<.00001) revealed a statistically significant difference between the test and control groups on the NCSE after 3–4 weeks of treatment (Fig. 4).

Neurobehavioral Cognitive State Examination total scores after 3–4 weeks of treatment.
P300
Four trials with a total of 98 patients 27,47 –49 measured an improved P300 after acupuncture treatment. The P300 was measured by the key point electromyography/evoked potential instrument with auditory oddball paradigm. The main index consisted of latency and amplitude. For the comparison of 8–12 weeks of acupuncture with no acupuncture in addition to medicine or rehabilitation group, the P300 latency (chi-square=40.29; p<.00001; I 2 =93%) indicated that included studies were of clinical and statistical heterogeneity. The fixed-effects model was adopted in the meta-analysis; the merged MD value was −12.80 (95% CI, −21.08 to 4.51). The tests for overall effect (Z=3.03; p=.002) revealed a statistically significant difference between the test and control groups in latency (Fig. 5).
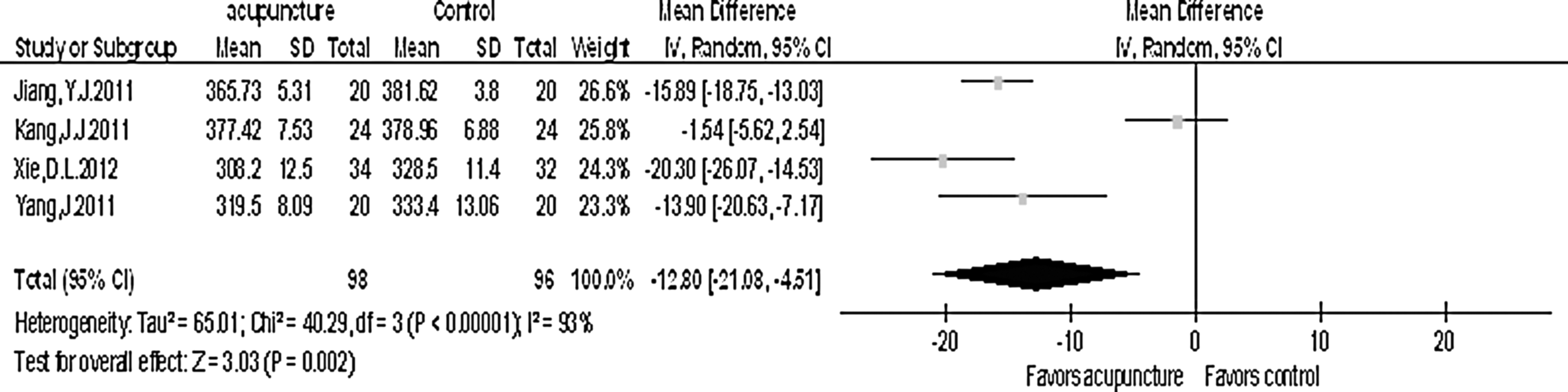
P300 latency after 8–12 weeks of treatment.
For the comparison of 8–12 weeks of acupuncture with no acupuncture in addition to medicine or rehabilitation group, the P300 amplitude was compared (chi-square=2.10; p=.55; I 2 =0%). The fixed-effects model was adopted in the meta-analysis; the merged MD value was 1.38 (95% CI, 0.93–1.82). The tests for overall effect (Z=6.11; p<.00001) indicated a statistically significant difference in amplitude between the test and control groups in amplitude (Fig. 6).
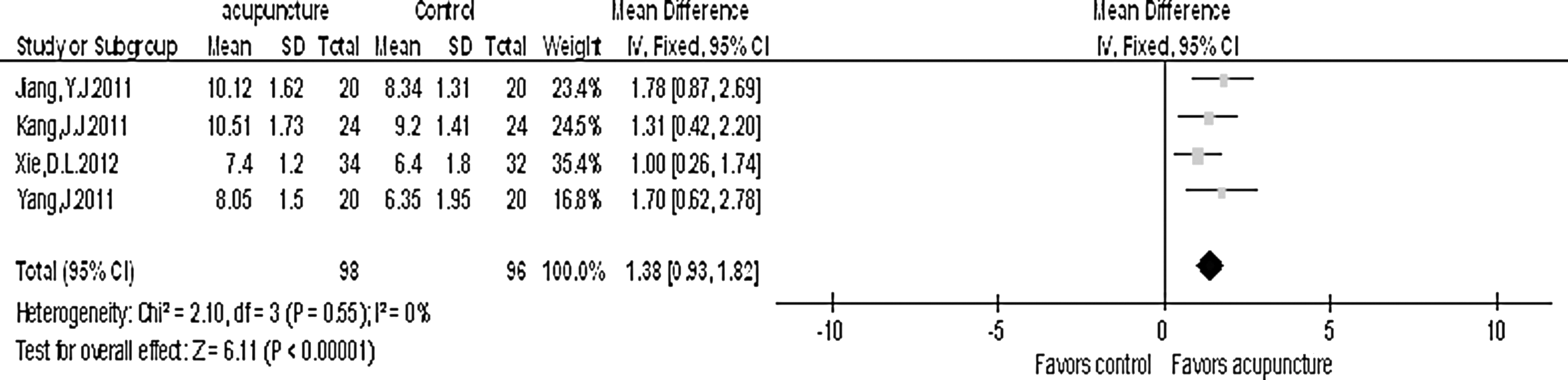
P300 amplitude after 8–12 weeks of treatment. CI=confidence interval; SD=standard deviation.
The other trials measured improved cognitive impairment after various acupuncture treatments for which the time interval was different; thus, the index was not merged.
Discussion
The conclusion drawn from the present data is that acupuncture may improve cognitive impairment after stroke. Numerous papers have discussed the effects of acupuncture on impaired cognitive function and have proposed the possible mechanisms of acupuncture that may lead to improved cognitive function after stroke. Litscher and colleagues 32 reported that acupuncture may increase mean values of regional cerebral oxygen saturation and significantly increase mean blood flow velocity of the right middle cerebral artery. Lee and coworkers 33 investigated the correlation between acupuncture and neuroimaging using single-photon emission computed tomography in patients with stroke. The results of their study suggested that postacupuncture images showed multiple activation sites in the periphery of the ischemic area or in the hypoperfused zone in the affected vascular territory.
The correlation between cognition and cerebral blood flow may partly explain the cognitive-enhancing effect of acupuncture. 34 Dos Santos and colleagues 35 suggested that electroacupuncture may prevent atrophy of some limbic structures, and thus improve cognitive deficits in pilocarpine-epileptic rats. The authors of that study postulated that this effect may depend on the serotonergic system. 35 Wang and associates 36 suggested that electroacupuncture may modulate the production and clearance of free radicals, as well as improve memory and the ability to learn in a rat model of vascular dementia. Furthermore, evidence from functional magnetic resonance imaging indicated that different acupoints on the same meridian may activate certain similar areas of the brain. 26
The late component of the ERPs, the P300, is a marker for cognitive brain function. The hippocampus, thalamus, and frontal cortex are considered potential locations of the P300 generators, 37 and these structures are important for learning and memory. P300 has been widely used to assess cognitive decline in various diseases affecting the central nervous system, especially in dementia-related disorders. 38 –41 P300 latency increases as dementia symptoms increase. It is considered a consequence of the attention process, speed of the reaction, and immediate memory. Shorter P300 latencies indicate a superior mental performance relative to longer latencies. 42 Sufficient evidence suggests that the latency and amplitude of the P300 are altered in Alzheimer's disease. Furthermore, evidence indicates that the characteristics of the P300 wave are also compromised in individuals with mild cognitive impairment. Recent studies suggest that the latency and amplitude of the P300 wave might serve as a marker for monitoring the process through which mild cognitive impairment progresses to AD. Thus, the main indexes of P300 (1atency and amplitude) reflect complicated emotional activities, such as cognition, memory, and cognitive impairment. Evidence suggests that ERP is an objective, sensitive, and specific indicator in evaluating cognitive impairment, and P300 can be used to measure the severity of the impairment. 37,38
Four trials with a total of 98 patients showed that acupuncture had a positive effect on restoring cognitive function after stroke. These findings suggest that the deleterious effects of cerebral infarction may improve with Traditional Chinese Medicine. Tang 43 argued that scalp acupuncture should be the first choice in treating ischemic stroke. Scalp acupuncture activates the cerebral collateral circulation, increases blood volume in the brain, improves the velocity of blood flow, and repairs the ischemic condition in the affected area of the brain; 27,44 thus, it provide a potential mechanism for the therapeutic effects of this approach. Therefore, P300 can be used as one of the objective indicators for evaluating the therapeutic effect of scalp acupuncture.
Two trials 45,46 demonstrated that acupuncture did not improve cognitive impairment after stroke. Potential explanations for these discrepant findings include the short length of the intervention period, the differential placement of acupuncture points, the different methods of evaluation, and small sample size.
The outcome of this meta-analysis needs to be confirmed in future, prospective studies that include larger sample sizes. Limitations of this study that may have affected the results include small sample sizes, different criteria for evaluating cognitive function across studies, and the high risk of bias of the included studies. Furthermore, these analyses focused on comparing the overall effectiveness of combined treatment with acupuncture, without specifically analyzing the effects of acupuncture alone or the potential adverse incidents. It is difficult to comprehensively evaluate the differential effects of acupuncture from nonacupuncture interventions on cognitive impairment after stroke. In reference to the included trials, several different methods were selected for the assessment of cognitive impairment after stroke, and the intervention period varied across studies. Questions regarding how to achieve sensitive assessment methods and how long the treatment effects may last need to be resolved in future studies. Moreover, this study focused solely on cognitive function, and therefore future research is necessary to determine whether acupuncture can actively restore other functions of patients with stroke. Finally, the search was confined to reports written in Chinese or English because most journals on acupuncture are published in these languages. It is possible that additional reports may be included in non-Chinese databases or in other languages, which may have limited the results of our study.
The growing popularity of acupuncture, which is largely based on positive outcomes that are associated with less severe adverse effects and lower costs, clearly warrants additional research. Large-scale sham- or placebo-controlled trials are needed to confirm or refute the available evidence for acupuncture as an efficacious treatment for patients who have had a stroke. Future studies should clearly define the modality of acupuncture, use evidence-based acupuncture techniques and rigorous methods, adopt standard measures of assessment, and validate the outcomes. Future studies should also be reported according to the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) criteria in conjunction with the Consolidated Standards of Reporting Trials (CONSORT) criteria.
In conclusion, evidence from this meta-analysis suggests that acupuncture may improve cognitive function after stroke and supports the need for future research.
Footnotes
Acknowledgments
This study was supported by the Fujian University of Traditional Chinese Medicine. The authors are particularly indebted to Mr. Jing-Yu Tan for his review of the Chinese literature. They also thank Ms. Xue-Ping Lin for grammatical review of the manuscript.
Author Disclosure Statement
No competing financial interests exist.