
Abstract
Objectives:
To assess the efficacy of aromatic essential oils on neck pain.
Design:
Sixty participants with a history of neck pain and Neck Disability Index (NDI) score >10% were selected and randomly divided into control and experimental groups.
Setting:
Motion analysis laboratory at Hungkuang University.
Intervention:
For the experimental group, the intervention included 3% concentration cream composed of four essential oils: marjoram, black pepper, lavender, and peppermint. For the control group, only an unscented cream was provided. For 4 weeks, all patients applied 2 g cream directly to the affected area daily after showering or bathing.
Outcome measures:
Assessment was performed by using a visual analogue scale (VAS), NDI, pressure pain threshold (PPT) evaluated with a pressure meter, and neck-joint range evaluated with Motion Analysis System (MAS).
Results:
A t-test statistical analysis by SPSS statistical software indicated that VAS scores improved significantly for both groups (p<0.05). In addition, the experimental group had improved pain tolerance in the left upper trapezius (mean±standard deviation, 2.96±2.54) and right upper trapezius (2.88±2.90) as measured by the PPT. According to the NDI, the experimental group also showed significant improvement (p=0.02). Comparison of MAS values before and after the intervention showed significant improvement in the 10 motion areas in the experimental group. This finding suggests that the experimental group had better results than the control group.
Conclusion:
The essential oil cream developed in this study can be used to improve neck pain. This study appears to be the first to quantify this by using PPT and MAS.
Introduction
N
One of the most common nonmedical therapies for muscle pain and stiffness is massage. Lewis and Johnson (2006) reviewed several massage methods that used or did not use creams to treat musculoskeletal pain. The foundation of massage is the manipulation of the layers of muscle and connective tissue to enhance function, aid the healing process, reduce muscle reflex activity, and promote relaxation. 13
Aromatherapy has been accepted as a component of nursing care in certain countries, where nurses are permitted to apply essential oils to patients in approved hospitals 14,15 in order to provide nonpharmacologic pain relief. 16,17 Massage with aromatic essential oils reduced the severity of menstrual pain in outpatients with primary dysmenorrhea. 18 Aromatherapy assessments typically involve using subjective questionnaires, such as numerical rating scale (NRS), visual analogue scale (VAS), Western Ontario and McMaster Universities Arthritis Index (WOMAC), Short Form-36 General Health Questionnaire (SF-36), and other scales. 19 –21 Previous studies have evaluated the effectiveness of aromatic therapies by measuring blood pressure, heart beat, respiratory rate, and blood oxygen levels. 8,20,22 –24
In aromatherapy, essential oils derived from plants are added to a base massage oil or unscented lotion. The essential oils are claimed to exhibit a wide range of medicinal properties and to affect wound healing, infection, and blood circulation. 25 The benefits of essential oils for aromatherapy include ease of application and rapid relaxing effects. Neck pain is typically related to sustained neck muscle contractions caused by working posture. No previous study appears to have described how aromatherapy affects neck pain and range of motion. Therefore, this study was conducted to evaluate how aromatherapy affects neck pain and range of motion by using scientific assessment methods. The null hypothesis was that the aromatherapy intervention is associated with nonsignificant changes in neck pain and range of motion.
Materials and Methods
Participants
This randomized controlled trial was approved by the institutional review board of Hungkuang University (project number 99-13-002). According to G*Power software, version 3.1.7 (Heinrich-Heine-Universität Düsseldorf, Germany), a study sample of 44 can detect a medium effect size (d=0.5) with a power of 90% at α=0.05 regarding the parameters of outcome measures. Recruitment advertisements that provided the purpose of research, major inclusion and exclusion criteria, time commitment for participation, and study principles were posted in community and university bulletin boards in Central Taiwan. A preliminary interview was then conducted for participants who scored >10% on the Neck Disability Index (NDI). All volunteers fulfilling the inclusion criteria were invited for a medical consultation to confirm their suitability, exclude other serious illness, explain the experimental procedures of the study and the allergy risks of essential oils, and obtain informed consent. The inclusion criteria were (1) age 20–65 years; (2) score >10% in the NDI; and (3) no acupuncture, massage, physical therapy, or medication during the previous month. The exclusion criteria were (1) allergy to essential oils, (2) spinal deformities or herniated discs, (3) cervical neural defects or spinal cord lesions, (4) neck surgery or cervical spine fracture during the previous 6 months, and (5) infections or fractures caused by osteoporosis. 5 Sixty participants were enrolled in the study and randomly assigned to the control (n=30) or experimental (n=30) groups. All 60 enrolled participants completed the study.
Materials
The essential oils and creams used in this study were manufactured by Arte Verde Co. (Röthis, Austria) and purchased from Fung Cheng International, Inc,, Taiwan. The commercial supplier was recommended by our aromatherapy expert for authenticity and purity of materials. Gas chromatography–mass spectrometry analysis revealed that the oils contained the following constituents: marjoram(-)-4-terpineol (10.53%), sabinene hydrate trans (7.29%), α-terpineol (5.57%), black pepper (caryophyllene, 16.75%), D-limonene (15.00%), L-β-pinene (9.94%), lavender (linalyl acetate [28.86%], linalyl alcohol [25.22%], lavandulol acetate [6.04%]), peppermint (menthol, 34.78%), p-menthone (17.88%), and menthyl acetate (9.62%). The four essential oils—marjoram, black pepper, lavender, and peppermint—were mixed in a ratio of 2:2:1:1 and then mixed with an unscented cream at a final concentration of 3%. Many plant extracts or essential oils may be poisonous; therefore, exceptionally low doses are used. Essential oils are concentrated and intensely energetic in their effects, so very little is needed for successful treatment in general use. Almost all aromatherapy reference books suggest a safe use concentration in the range of 0.05%–3%. 26,27 The control group applied an unscented cream that contained no essential oils. After randomized grouping, a 24-hour closed patch test was performed using the essential oil cream or unscented cream and medical Scotch tape. The creams were applied to the skin behind the ear to determine whether they triggered an allergic response in the study participants. 28 Safety and allergy were evaluated through the physical examination and participant self-reporting. No adverse effects were reported.
Procedure
Figure 1 shows the aromatherapy intervention protocol design. None of the participants fulfilled the criterion for an allergic reaction (red rash, itchy, burning skin, blisters, or wheals). Each day after showering or bathing, all participants were instructed to apply 2 teaspoons (approximately 2 g) of the cream to the neck and upper trapezius muscles until fully absorbed. To improve adherence to the intervention protocol, a research team member followed up with the participants twice a week by telephone. The duration of the aromatherapy intervention was 4 weeks.

Study flow.
Outcome measures
The pretest measures were performed 1 day before initiation of the intervention; posttest measures were performed after completion of the 4-week intervention. The NDI contains 10 items for assessing how neck pain affects the ability of participants to perform their daily activities. The scale comprised the items pain intensity, personal care (e.g., washing, dressing), lifting, reading, headaches, concentration, working, driving, sleeping, and recreation. These items indicated the levels of discomfort in the head, neck, and upper limbs caused by cervical pain symptoms. 29,30 The NDI score is calculated by summarizing the responses for each item and multiplying that by 2 to obtain a disability percentage. The maximum total score is 100. A score >10% indicates some disability in the neck. The higher the NDI value, the more serious the neck disability of the participant. 31,32 In this study, NDI scoring was examined by a senior orthopedic physical therapist who had more than 15 years of clinical experience.
The visual analogue scale (VAS) is a subjective pain assessment on which participants their response on a horizontal straight line 10 mm in length. The left end (score 0) represents no pain, and the right end (score 10) represents severe pain. This scale enables participants to quantitatively express the severity of the pain experienced. 33
The pressure pain threshold (PPT) is defined as the minimum force applied that induces pain on an affected area. A high PPT value indicates a correspondingly high pain tolerance. The pressure test was performed on the upper trapezius muscle, in the midpoint between the seventh cervical vertebra and the acromion connection. The upper trapezius arises from the external occipital protuberance, the medial third of the superior nuchal line of the occipital bone, and the ligamentum nuchae. It is a large superficial cervical muscle that plays a crucial role in maintaining neck posture. The average minimum pain thresholds of the left and right upper trapezius muscles were recorded. 34
The Motion Analysis System (MAS) was equipped with five infrared cameras to capture the dynamic movement trajectories of markers on the neck and shoulder. The dynamic range of motion of the neck of each participant was recorded. Twelve surface markers, 10 mm in diameter, were attached to landmarks that represented four neck levels: occiput level, C2 level, C7 level, and shoulder level (Table 1 and Fig. 2). 35 The occiput level comprised the bilateral mastoid processes and base of the occiput, the C2 level comprised the transverse and spinous processes of the second cervical vertebrae, the C7 level comprised the transverse and spinous processes of the seventh cervical vertebrae, and the shoulder level comprised the bilateral acromions and second thoracic spinous process. The participants performed the following six neck movements: extension, flexion, left bending, right bending, left rotation, and right rotation. They rested for 5 seconds between each movement and completed three successful trials for each movement. The neck marker sets were captured and identified using EVaRT4.6 software. 36 These neck motion data were digitized three times, and the mean values of the three measurements were used in subsequent analyses.

Motion Analysis System: 12 surface markers.
Data analysis
The characteristics of the two groups were compared using independent t tests for pretest and posttest measurements. Paired t tests were conducted to examine the statistical differences between the results collected preintervention and postintervention within each patient group. The level of significance was .05 in all tests. All analyses were performed by using SPSS software, version 12.0 (SPSS Inc., Chicago, IL).
Results
Patient characteristics
Table 2 lists the patient characteristics: sex, age, history of trauma, exercise habits, pain duration, pain frequency, and extent of pain disturbance. This table shows no significant differences in sex and medical conditions between two groups. We consider these two groups to be independent each other, and the borderline age effect may not influence the outcome measurements in the present study. The control group consisted of approximately 7 men (23.33%) and 23 women (76.67%); the experimental group contained 3 men (10.00%) and 27 women (90.00%). The groups did not significantly differ regarding gender (p=0.17). A total of 50 women (83%) enrolled in this study, which may suggest that women with neck pain are more willing to be the volunteers and receive aromatherapy. 23,37 The average participant ages (±standard deviation) were 26.13±7.08 years in the control group and 30.93±10.01 years in the experimental one. The duration of neck pain was approximately 51.67±40.43 months in the control group and 61.46±77.85 months in the experimental group, indicating that participants had experienced neck pain for more than 4 years. Forty participants experienced fewer than three neck pain episodes per week, 13 participants experienced more than three neck pain episodes per week, and 7 participants experienced daily neck pain episodes. Forty-one participants felt mildly disturbed by pain, 9 participants felt moderately disturbed by pain, and 1 participant felt severely disturbed by pain. The results of the independent-sample t test indicated that the groups significantly differed with regard to age (p=0.04); however, the remaining discrete variables exhibited nonsignificant differences between the two participant groups (p=0.08–0.68).
Unless otherwise noted, values are the number (percentage) of participants. Values expressed with a plus/minus sign are the mean±standard deviation.
Table 3 lists the pain locations, associated symptoms, and causes of pain among the study participants. Twenty-eight participants (46.7%) in the control group and 24 participants (40.0%) in the experimental group experienced pain in the neck area. Overall, 18 participants experienced back pain: 11.7% in the control group and 18.3% in the experimental group. The associated symptoms were as follows: 45 participants experienced neck stiffness, 31 participants experienced neck pain, 41 participants experienced muscle tightness, 6 participants experienced transferred pain, 19 participants were unable to sleep, and 4 participants experienced dizziness or tinnitus. Twenty participants considered their neck pain to have been caused by bad posture (n=23), pressure (n=17), and work or computer use (n=21). The pain locations, associated symptoms, and considered pain causes of the control and experimental groups exhibited nonsignificant differences.
NDI
As shown in Figure 3, in the control group, the preintervention (32.40%±8.44%) and postintervention (30.33%±7.61%) NDI scores exhibited nonsignificant differences (p=.17). In the experimental group, the NDI score significantly decreased after the intervention (32.60±9.26 versus 29.87±8.14; p=.02).
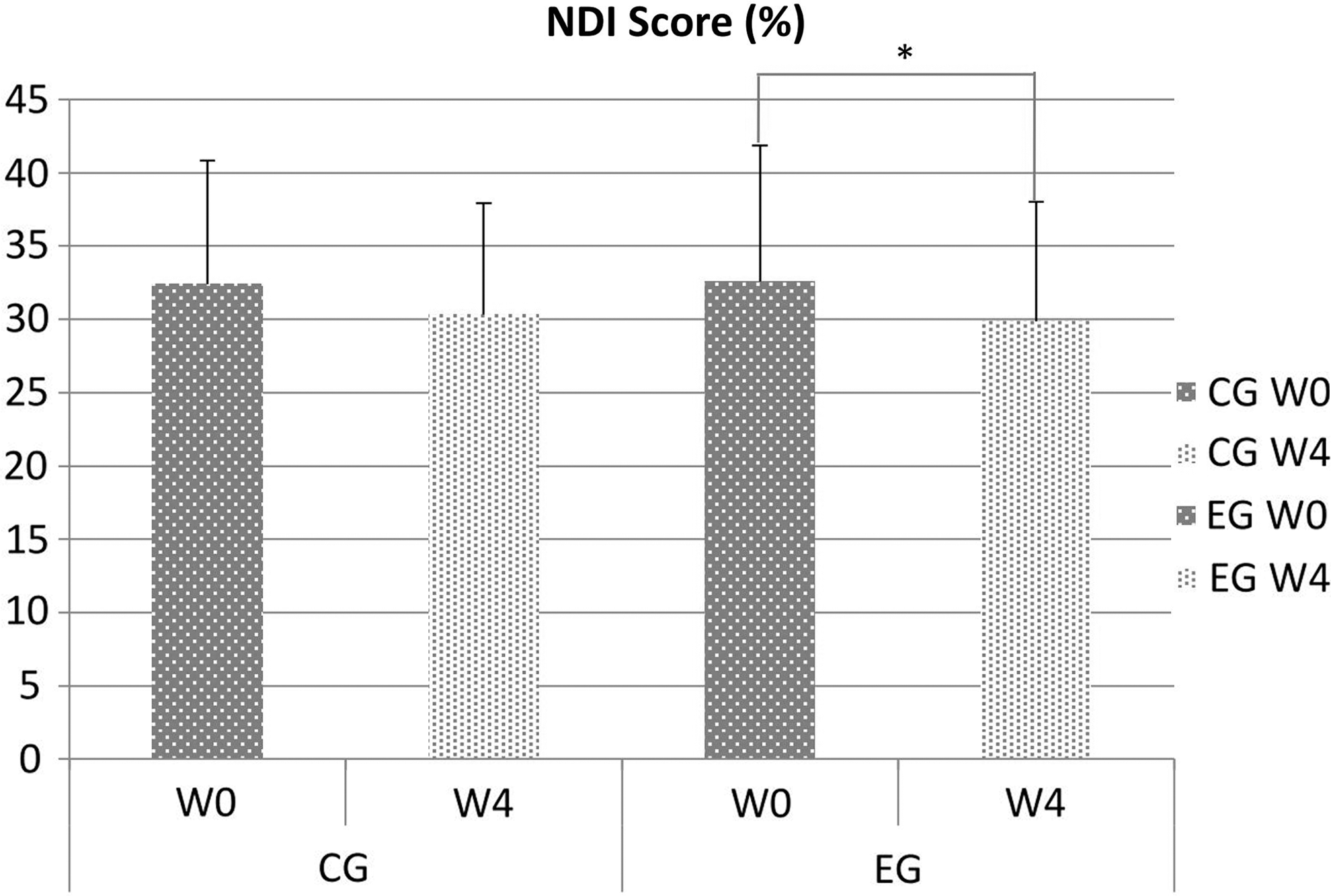
The Neck Disability Index (NDI) scores were evaluated at the pretest and posttest (after 4 weeks of aromatherapy intervention) in experimental (EG) and control (CG) groups. *p<0.05. W0, pretest; W4, posttest after 4 weeks aromatherapy intervention.
VAS
In the control group, the paired t tests indicated that the VAS score significantly decreased after the intervention (3.97±2.22 versus 2.44±1.79; p<0.05) (Table 4). The VAS score of the experimental group also significantly decreased after the aromatherapy intervention (3.93±2.69 versus 2.55±1.75; p<0.05).
W0, pretest; W4, posttest after 4 weeks of aromatherapy intervention; W4−W0, difference between posttest and pretest; PPT, pressure pain threshold.
PPT
Table 4 and Figure 4 show the PPT values of the two groups. According to the paired t tests, in the control group the PPT values collected preintervention and postintervention exhibited nonsignificant differences (left upper trapezius p=0.07, right upper trapezius p=0.07). In the experimental group, the PPT values indicated that pain threshold significantly increased in the left (postintervention−preintervention=2.96±2.54 kg/cm2) and right (postintervention−preintervention=2.88±2.90 kg/cm2) upper trapezius following the intervention. In the experimental group, the PPT values of the upper trapezius showed significant differences (both p=.00), indicating that the participants in the experimental group had greater pain tolerance in the upper trapezius muscles compared with those in the control group.

The Pressure Pain Threshold (PPT) was evaluated at the pretest and posttest (after 4 weeks aromatherapy intervention) in experimental (EG) and control (CG) groups. *p<0.05. W0, pretest; W4, posttest after 4 weeks aromatherapy intervention.
MAS
Figure 5 shows a group comparison of the preintervention and postintervention ranges of neck motion. In the control group, three motion areas were associated with significant differences in the values collected preintervention and postintervention: right bending at the C7 level (14.60±37.05) and left rotation at the C7 (−25.19±29.29) and shoulder (−19.13±38.05) levels. In the experimental group, 10 motion areas were associated with significant differences in the values collected preintervention and postintervention: 1 in extension movement at shoulder level (22.00±38.99); 4 in flexion movement at the occiput (20.10±37.60), C2 (30.80±41.69), C7 (17.60±44.02), and shoulder (22.60±45.60) levels; one in left bending at the C7 level (12.00±24.24), one in right bending at shoulder level (18.50±35.91), one in left rotation at occiput level (16.10±29.84), and two in right rotation at the C2 (26.10±44.16) and C7 (9.62±23.59) levels. Our results indicated that the participants in the experimental group were associated with greater increases in neck motion ranges compared with those in the control group (particularly in flexion movement). On the basis of our results, the data analysis showed the NDI score, VAS, PPT values in the left and right upper trapezius, and motion analysis system in extension-flexion, left-right bending, and rotation improved in the experimental group.
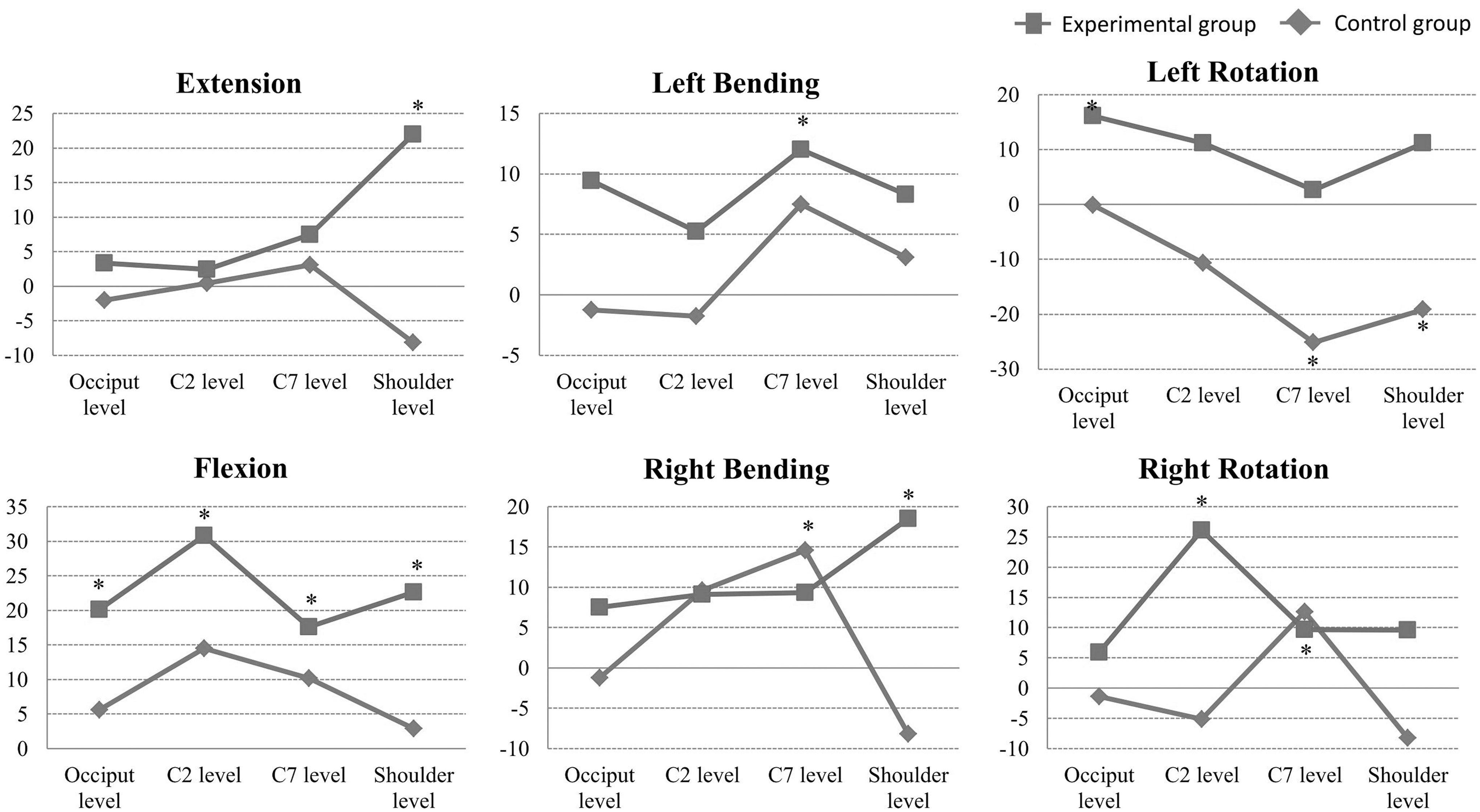
Within-group measure analysis of Motion Analysis System pre- to posttest.
Discussion
This study evaluated the efficacy of using aromatherapy to relieve the symptoms of neck pain by using four clinical and scientific assessments: VAS, PPT, NDI, and MAS. After 4 weeks of aromatherapy, the experimental group showed significant reductions in neck pain symptoms and increased range of motion.
Aromatherapy is considered to stimulate the parasympathetic nervous system and induce pleasant sensations. 38 Previous studies have evaluated the efficacy of aromatherapy on pain reduction by using the VAS. 33,39 –41 In our study, both participant groups demonstrated improved VAS scores following the intervention, but only the experimental group showed improvement in the NDI and PPT values postintervention. Studies have suggested that the VAS provides an indicator of subjective pain but does not objectively measure pain. 42 The NDI and PPT have been described as feasible for evaluating patients with chronic neck pain. 43 The NDI is a standard instrument for measuring self-rated disability caused by neck pain and is used by clinicians and investigators. 30 Ferreira et al. identified neck pain–specific questionnaires and scales that measure functioning and disability. They assessed whether the contents of questionnaires and scales were similar to the International Classification of Functioning, Disability and Health (ICF). The NDI has demonstrated a well-balanced distribution of items across the ICF components. 44 Although NDI scores in the experimental group decreased significantly after the aromatherapy intervention, further investigation is required to establish whether the observed changes are clinically meaningful.
Saiz-Llamosas et al. used the PPT to assess the effectiveness of the cervical myofascial technique over the bilateral fifth and sixth of seven cervical vertebrae zygapophyseal joints. 43 The test-retest reliability of PPT was assessed on the upper trapezius muscles in the pilot study, and the intraclass correlation coefficients ranged from 0.846 to 0.937; these values were consistent with the findings of earlier studies. 45,46 They reported that the repeated measurements showed stable values and suggest that the PPT method can be recommended by experienced examiners. In the current study, the PPT values of the left and right upper trapezius muscles significantly improved in the experimental group following the intervention. The increased PPT of the upper trapezius muscles could be related to the analgesic and neuropeptide inhibitory effects of the essential oils. 47
Studies have investigated the possible causes of the effects of essential oils on pain, and essential oils such as lavender and marjoram have been shown to significantly reduce pain and depression in patients with arthritis and cancer. 48,49 Marjoram oil activates the parasympathetic nervous system, relaxes the sympathetic nervous system, and helps protect against generalized myoclonic seizures in humans. 23,50,51 Hajhashemi et al (2003) proposed the anti-inflammatory and antinociceptive effects of 1,8-cineole, a terpenoid oxide occurring in lavender essential oil. 52 Yip and Tse provided eight sessions of acupuncture point stimulation, followed by aromatic lavender oil application, to a group of participants and reported no adverse effects and the short-term relief of lower back pain. 20 Thus, the increased PPT in the experimental group may be attributable to the lavender essential oil. 53,54
The MAS provides relatively objective measurements of cervical activities and quantitatively analyzes neck motion by using an optical three-dimensional system. 55 –57 A neck model was established to differentiate the movements and posture of cervical spine and to examine the reliability of measuring the cervical movements with surface markers. 35 The results indicated that the average skin movements for surface markers at the end ranges of neck motion ranged from 1.54±0.95 mm to 3.05±0.55 mm. This earlier study indicated that the limited effect of relatively small movements of neck skin and muscles compared to the total cervical range of motion by the application of surface markers in MAS can help predict actual neck motion.
The outcome measurement of neck range of motion in the current study was based on this verified neck model. The findings indicated that the neck range of motion significantly increased in the experimental group following the aromatherapy intervention. There was a trend toward increased ranges of motion among the various cervical levels during neck motion activities (Fig. 5).
This study mixed and applied four essential oils (marjoram, lavender, black pepper, and peppermint) to participants in the experimental group. Marjoram contains flavonoids, phenolic terpenoids, and tannins. 58 It exerts inhibitory effects on blood platelet adhesion and improves blood circulation. 59 Studies have indicated that marjoram extract helps protect against systemic muscle spasm seizures. 51 Therefore, marjoram in the current essential oil mix may have played a role in reducing neck muscle tightness. Previous studies have reported that essential oils effectively stimulate blood circulation, improve oxygen supply, and relax tense muscles. 60 –62 Black pepper contains β-caryophyllene, which exhibits anti-inflammatory properties, and capsaicin, which is an analgesic and a neuropeptide inhibitor. 47 Freeman et al. reported that postural stability in older adults can be improved by smelling lavender and black pepper essential oils. 63 Black pepper has been suggested to relieve muscle spasms. 64,65 Marjoram essential oil has improved blood circulation and reduced muscle tightness, and black pepper can be a neuropeptide analgesic to relieve muscle spasm seizures. Therefore, stronger concentrations of these two oils were chosen for the current study, and they may have contributed to the effect on muscle relaxation and neck pain reduction.
Ghelardini et al. demonstrated that lavender oil, linalool, and linalyl acetate exert local anesthetic effects. 66 Several studies have reported that lavender essential oil applied with massage can reduce patient perception of muscle pain. 20,41,49,67,68 Field and colleagues found that a mixture of bergamot, lavender, and frankincense oil reduced hand pain. 69 Peppermint oil has been considered to exhibit analgesic properties and reduce mental stress. 37,70 The high menthol content in peppermint essential oils can also provide cooling effects. 47 The essential oils in this study may have rapidly penetrated the skin and muscle tissues of participants in the experimental group to increase blood circulation in the affected areas and reduce neck muscle stiffness and pain. On the basis of a review of literature and previous findings, the essential oils applied in this study might help alleviate neck pain and improve neck range of motion.
This study had several limitations. For example, healthy participants with minor neck symptoms were evaluated. Therefore, additional studies are required to establish whether the essential oils exert the same effects in participants with serious neck pain or other pain symptoms. In addition, the experimental period was only 4 weeks. Further research must be conducted to verify the effects of the essential oils on neck symptoms over time and to determine whether the efficacy of the essential oils is reduced after the cessation of application.
Conclusion
These study results indicate that essential oil cream may alleviate neck pain, improve neck range of motion, and be simply and conveniently self-applied. The results of the VAS, PPT, NDI, and MAS assessments suggest that aromatherapy provides an appropriate complementary and alternative medicine option for people with neck pain.
Footnotes
Acknowledgments
This work was financially supported by Hungkuang University. The authors would like to thank the staff and students of Hungkuang University for their assistance. The authors would also like to thank Dr. Ming-Ho Du for his contributions and support.
Author Disclosure Statement
The authors declare that no competing financial interests exist.