
Abstract
Objectives:
To review and evaluate the efficacy and safety of tian jiu therapy on san fu tian for adults with asthma.
Methods:
A literature search through August 31, 2013, was done to identify comparative studies evaluating effective rate, pulmonary function, immune response, recurrence rate, quality of life, and adverse events. The Cochrane Library, PubMed, EMBASE, and Chinese National Knowledge Infrastructure were searched; only randomized controlled trials with treatment groups using tian jiu therapy were included. Cochrane Collaboration's risk of bias tool and Review Manager software, version 5.2, were used for the data synthesis.
Results:
Six studies involving 657 patients were identified. tian jiu therapy was more effective than the control intervention (odds ratio [OR], 3.51; 95% confidence interval [CI], 2.05–6.00; p<0.00001; I2 =18%). The treatment group had a bigger decrease in IgE level (standard mean difference [SMD], −1.40; 95% CI, −2.18 to −0.63; p=0.0004; I2 =85%) and Eosinophil (Eos) level (SMD, −4.26; 95% CI, −6.28 to −2.23; p<0.00001; I2 =91%) compared with the control group. Included studies had a high risk of bias. Few adverse effects were reported in the included studies, and no serious adverse responses occurred. Adverse effects did not result in any dropouts.
Conclusions:
All studies indicated that tian jiu therapy has a positive effect on adults with asthma and that it is relatively safe because of its noninvasive nature. However, the limitations of the research design of the existing studies resulted in high risk of bias. More randomized controlled trials of better methodologic quality are needed to further confirm efficacy and safety of this therapy.
Introduction
A
Asthma is a worldwide problem, affecting an estimated 300 million people. 4 Like patients with any chronic disease, many people with asthma seek alternative treatments. Surveys indicate that up to 50% of patients with asthma may be using some form of unconventional treatments. 5 However, in their 2012 report, “Global Strategy for Asthma Management and Prevention,” the Global Initiative for Asthma suggested that complementary and alternative medicine has a limited role for asthma because these approaches have been insufficiently studied and their effectiveness is largely unproven. 4
Tian jiu therapy is an ancient technique for treating asthma and allergic rhinitis. For this therapy, Chinese herbal medicine is used in conjunction with acupuncture theory to achieve the treatment effect, but no needle is involved. Asthma is considered a “winter” disease in Traditional Chinese Medicine (TCM), and the acute attacks are more likely to happen in winter. According to the TCM theory of “treating winter disease in summer” and “breeding yang qi in spring and summer,” applying tian jiu in the three hottest days of the year—san fu tian—could help reduce the incidence rate of asthma attacks in winter. 6
The mechanism of tian jiu is straightforward. Carefully selected stimulating Chinese herbs that are in hot in nature are ground into powder and mixed with ginger extract to form pellets, which are then pasted onto specific acupoints. During the hottest days of summer, pores open up, blood flows more freely, and the yang qi in the body is at its peak. The medication acts on the acupoints, causing redness, congestion, or even blister at the local area, thereby stimulating the related meridians and harmonizing the targeted visceral system.
In 1695, the classic TCM monograph General Medicine According to Master Zhang ( )
7
had already recorded the medicine and acupoints to be used for treating asthma with tian jiu. Numerous recent studies have also assessed the clinical efficacy of tian jiu in China. The current article reviews and evaluates the efficacy and safety of tian jiu therapy on san fu tian for adults with asthma.
)
7
had already recorded the medicine and acupoints to be used for treating asthma with tian jiu. Numerous recent studies have also assessed the clinical efficacy of tian jiu in China. The current article reviews and evaluates the efficacy and safety of tian jiu therapy on san fu tian for adults with asthma.
Methods
Literature search
The Cochrane Library, PubMed, EMBASE, and Chinese National Knowledge Infrastructure were searched. English-language databases were searched by using retrieval words “asthma” and “acupoint application” or “acupoint sticking”; the Chinese database was searched by retrieval words  and
and  or
or  or
or  . Dates and language of publications were not restricted; the last retrieval date was August 31, 2013. Only randomized controlled trials (RCTs) were included; animal studies, review articles, republished data, case studies, and reports lacking full text or with incomplete and incorrect data were excluded.
. Dates and language of publications were not restricted; the last retrieval date was August 31, 2013. Only randomized controlled trials (RCTs) were included; animal studies, review articles, republished data, case studies, and reports lacking full text or with incomplete and incorrect data were excluded.
Study patients
The study participants were adults diagnosed with asthma according to clear diagnostic criteria.
Interventions
The treatment groups received tian jiu therapy, in which selected Chinese herbal medicines were pasted on selected acupoints on san fu tian (drugs and foundation treatment were allowed during acute asthma attack). The control groups used different therapy than the treatment groups. Studies that used combination therapies for the treatment group or were designed to compare the efficacy of tian jiu in different seasons were excluded.
Outcome measures
Outcome measures included total effective rate, immune-related biomarker, pulmonary function test results, recurrence rate, Asthma Control Test results, and adverse events.
Risk of bias assessment
The studies were evaluated according to the Cochrane Handbook for Systematic Reviews of Interventions (version 5.1) recommended “risk of bias” criteria: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, (6) selective reporting, and (7) other bias. Individual studies were assessed as having high risk of bias, low risk of bias, or unclear risk of bias. Two authors searched the literature searched and selected and evaluated the studies. When these authors disagreed or were uncertain about the evidence, consensus was reached through discussion or assistance from the third author.
Data synthesis
Review Manager, version 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) was used to perform the meta-analysis. For binary outcomes, the Mantel-Haenszel method for odds ratio (OR) with corresponding 95% confidence intervals (CIs) was used. For continuous data, standard mean difference (SMD) with corresponding 95% CI was used. Heterogeneity among studies was measured by using I 2 statistics; when the heterogeneity test showed an I 2 of ≤50%, a fixed-effects model was used, and when the heterogeneity test showed an I 2 of 50%, a random-effects model was used.
Results
Six studies met the inclusion criteria and were included in this meta-analysis. Figure 1 details the process used to select trials (identification of articles and reasons for inclusion and exclusion). Table 1 shows the characteristics of the six included studies.
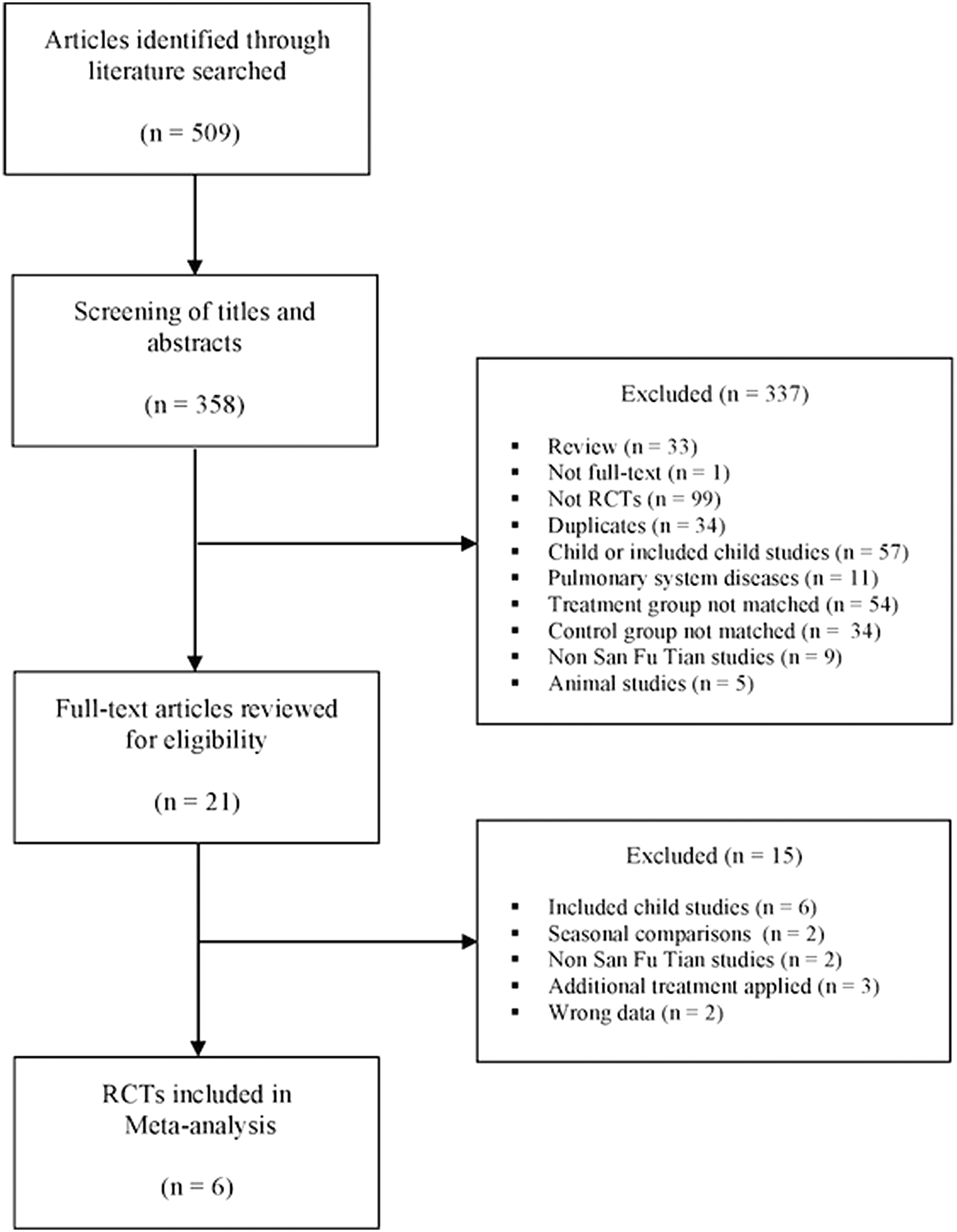
Flowchart for selection of trials. RCT, randomized, controlled trial.
ACT, Asthma Control Test; CG, control group; F, female; M, male; OTC, over-the-counter; QOL, quality of life; TCM, Traditional Chinese Medicine; TG, treatment group.
Risk of bias assessment
Figure 2 shows risk of bias by trial, and Figure 3 shows overall risk of bias. Four studies adequately described random sequence generation and were judged as having low risk of selection bias. 8 –11 The other two studies 12,13 did not describe the methods and were therefore judged as having an unclear risk of bias. No studies described allocation concealment, and thus all were considered to have an unclear risk of selection bias. Five studies had a high risk of performance bias because the physicians who performed the procedures were not blinded; 8 –12 the other study 13 was single blinded and thus judged as high risk because incomplete blinding probably influenced the outcome. Outcome assessors were not blinded for all studies, thereby introducing high risk of detection bias. Studies were of low risk of attrition bias because they had no missing data. Reporting bias remained unclear because there was insufficient information to permit judgment of risk. The included studies had no other important concerns that would introduce other biases.

Risk of bias by trial.
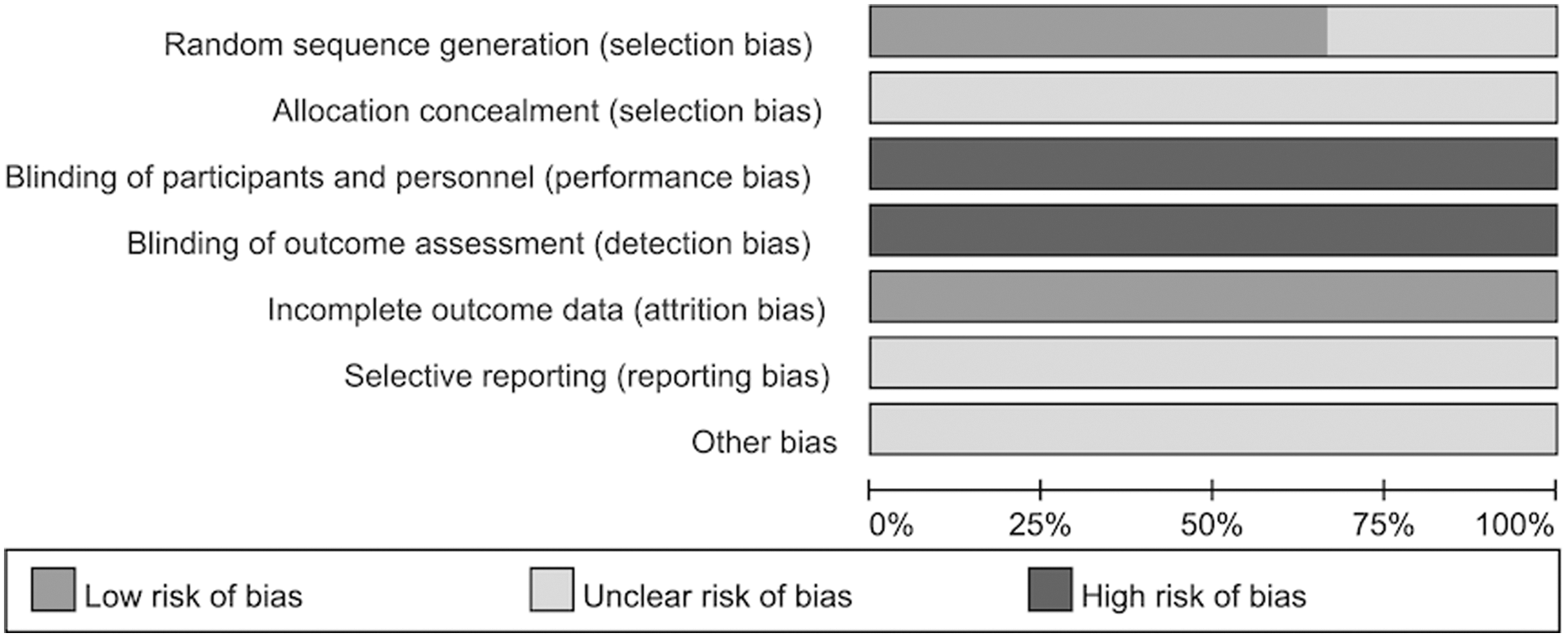
Risk of bias summary.
Effective rate
Tian jiu therapy vs. blank control, placebo, and medicine
Four studies 9 –11,13 with 500 patients reported effectiveness of tian jiu therapy. The finding reached statistical significance (OR, 3.51; 95% CI, 2.05–6.00; p<0.00001; I 2 =18%) (Fig. 4); the effective rate was higher in the tian jiu treatment groups than in the control groups.
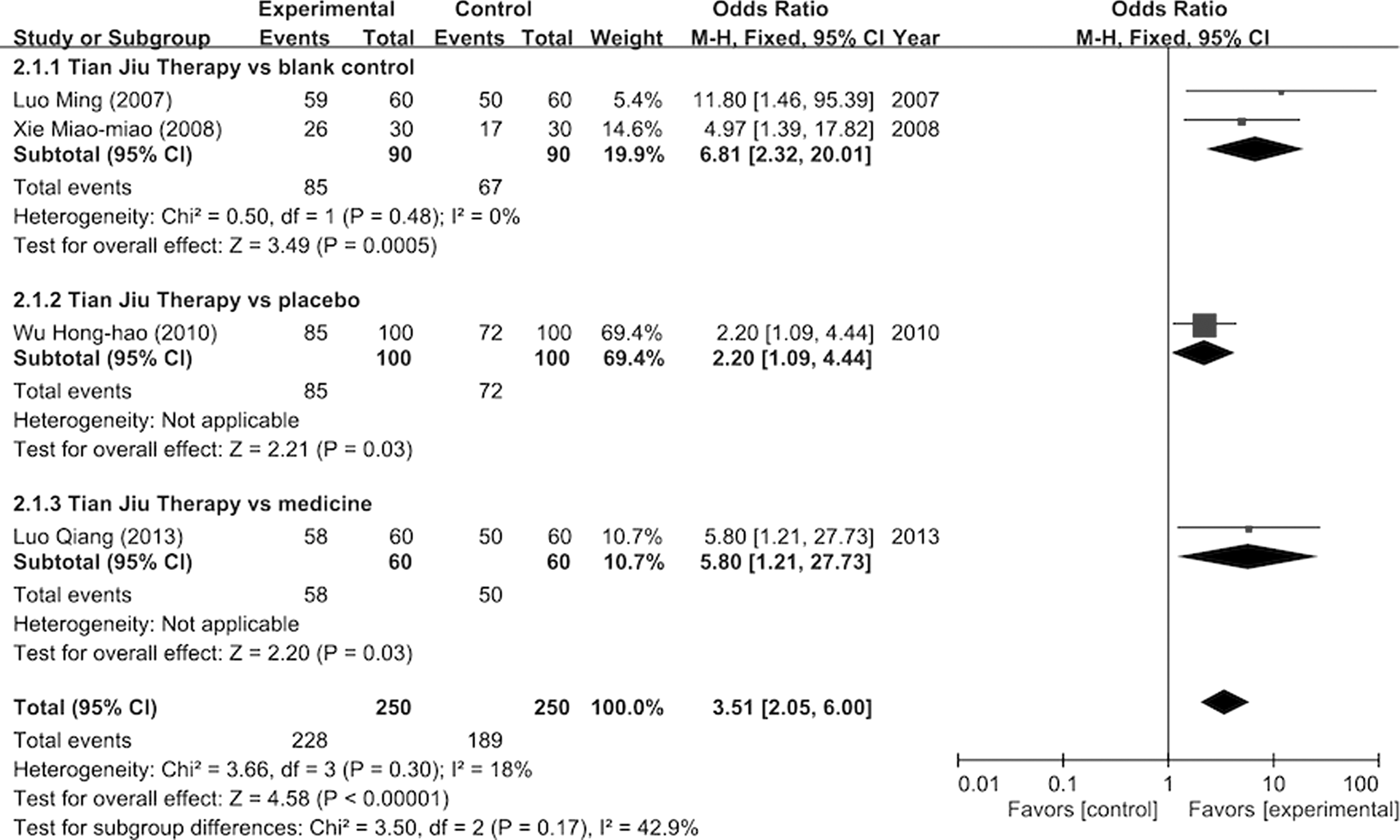
Effective rate of tian jiu therapy. CI, confidence interval; M-H, Mantel-Haenszel.
Tian jiu therapy vs. blank control
In two studies 9,10 with 180 patients that compared tian jiu therapy to blank control, the finding reached statistical significance (OR, 6.81; 95% CI, 2.32–20.01; p=0.0005; I 2 =0%) (Fig. 4). The effective rate was higher in the tian jiu groups than in the control groups.
Tian jiu therapy vs. placebo
Only one study 11 with 200 patients compared tian jiu therapy to placebo; the finding was statistically significant (OR, 2.20; 95% CI, 1.09–4.44; p=0.03) (Fig. 4). The effective rate was higher in the tian jiu treatment group than in the placebo group.
Tian jiu therapy vs. medicine
Only one study 13 with 120 patients compared tian jiu therapy to medicine; the finding reached statistical significance (OR, 5.8; 95% CI, 1.21–27.73; p=0.03) (Fig. 4). The effective rate was higher in the tian jiu treatment group than in the medicated group.
Immune-related biomarker: IgE Test
Tian jiu therapy versus blank control, medicine
Three studies 8,10,12 with 217 patients reported immune response (IgE) of tian jiu therapy; the finding was statistically significant (SMD, −1.40; 95% CI, −2.18 to −0.63; p=0.0004; I 2 =85%) (Fig. 5). The IgE level was lower in the tian jiu treatment groups than in the control groups.

Immune response (IgE) from tian jiu therapy. SD, standard deviation.
Tian jiu therapy versus blank control
Two studies 8,10 with 137 patients compared tian jiu therapy to blank control; the finding reached statistical significance (SMD, −1.75; 95% CI, −2.35 to −1.16; p<0.00001; I 2 =55%) (Fig. 5). The IgE level was lower in the tian jiu treatment groups than in the blank control groups.
Tian jiu therapy versus medicine
Only one study, 12 with 80 patients, compared tian jiu therapy to medicine. The finding was statistically significant (SMD, −0.75; 95% CI, −1.20 to −0.29; p=0.001) (Fig. 5). The IgE level was lower in the tian jiu treatment group than in the medicated group.
Immune-related biomarker: Eosinophil test
Tian jiu therapy versus blank control
Two studies 8,10 with 137 patients compared immune response (Eosinophil [Eos]) between patients receiving tian jiu therapy and those receiving blank control. The finding reached statistical significance (SMD, −4.26; 95% CI, −6.28 to −2.23; p<0.00001; I 2 =91%) (Fig. 6). The Eos level in the tian jiu treatment group was lower than that in the blank control group.

Immune response (Eos) from tian jiu therapy.
Pulmonary function tests
One study 13 reported pulmonary function test results (peak expiratory flow and forced expiratory volume in 1 second); quantitative synthesis was not performed for this single study. The study reported that the treatment group had greater improvement in peak expiratory flow and forced expiratory volume in 1 second than did the control group (p<0.01).
Recurrence rate
One study 13 reported recurrence rate after 1 year of follow-up; quantitative synthesis was not performed for this single study. The study reported that the asthma recurrence rate of the treatment group was lower than that in the control group (p<0.01).
Asthma Control Test
One study 11 reported on the Asthma Control Test (ACT; QualityMetric Inc., Lincoln, RI); quantitative synthesis was not performed for this single study. The study reported that the ACT findings were better in the treatment group than in the control group (p<0.05).
Adverse events
Two studies 8,10 reported adverse events. Adverse responses were not serious and were limited to skin redness, swelling, fever, itching, pain, or blisters; these conditions did not result in dropouts.
Discussion
In the modern pharmaceutical world, various new techniques, such as cavitational ultrasound, microscopic needles, and mild electroporation, have recently been developed to widen the use of transdermal drug delivery. 14 Applying medicine on the skin and acupoints for healing has long been practiced in China to treat both local and systemic disease. According to TCM theory, all medicine has a specific association with the meridians. Applying the appropriate medicine on the specific acupoints could stimulate the meridian and thereby treat the symptoms and irregularity affecting the visceral associated with that particular meridian.
Tian jiu, based on this theory, involves medication associated with the lung meridian to act upon respiratory symptoms. With the help of a medium (normally ginger juice or an essential oil) to open the pores and propel the medicine, the treatment is expected to strengthen the body, rebalance the immune system, and reduce the symptoms associated with asthma.
The medicine used in all six
8
–13
studies were similar to those recommended by the classic TCM monograph General Medicine According to Master Zhang,
7
with the medicine used in one study
8
the same as recommended. All studies used baijiezi ( , Sinapis albae, semen) and xi xin (
, Sinapis albae, semen) and xi xin ( , Asarum heterotropoides, herba). Both medicines are hot in nature and associated with the lung meridian. Xi xin is also associated with the kidney and spleen meridians.
, Asarum heterotropoides, herba). Both medicines are hot in nature and associated with the lung meridian. Xi xin is also associated with the kidney and spleen meridians.
According to TCM theory, the cause of asthma is highly associated with the weakening of the lung, kidney, and spleen systems. Except for one study,
12
the choice of acupoints was targeted to regulate the flow of qi in the lung, kidney, and spleen systems and to control the symptom of coughing and production of phlegm. The most common acupoints used by the studies were feishu ( ; BL13, pishu (
; BL13, pishu ( ; BL20), shenshu (
; BL20), shenshu ( ; BL23), ding chuan (
; BL23), ding chuan ( ; B1), and gaohuang (
; B1), and gaohuang ( ; BL43). The first three acupoints were used to regulate the flow of qi in the lung, spleen, and kidney meridians, respectively; ding chuan (
; BL43). The first three acupoints were used to regulate the flow of qi in the lung, spleen, and kidney meridians, respectively; ding chuan ( ; B1) was used to control the cough symptom; and gaohuangshu (
; B1) was used to control the cough symptom; and gaohuangshu ( ; BL43) was used to control the production of phlegm. Feishu (
; BL43) was used to control the production of phlegm. Feishu ( ; BL13) was used in one study,
12
but the other two acupoints—xinshu (
; BL13) was used in one study,
12
but the other two acupoints—xinshu ( ; BL15) and geshu (
; BL15) and geshu ( ; BL17) were only used in one study,
12
and might have a looser connection to the asthma symptoms.
; BL17) were only used in one study,
12
and might have a looser connection to the asthma symptoms.
The meta-analysis indicated positive changes in patients with asthma after they received tian jiu therapy. Statistically significant differences were detected in comparisons of total efficacy, IgE level, Eos level, pulmonary function, and results on the ACT between the treatment groups and the control groups.
In the selected studies, the efficacy evaluation was based on “The Guiding Rules of Clinical Research of New Chinese Medicine,” 15 issued by the China Food and Drug Administration. The focus was on symptom improvement. The goals of successful management of asthma include achieving and maintaining control of symptoms, maintaining normal activities, maintaining pulmonary function as close to normal as possible, and preventing asthma exacerbation. 5 The efficacy outcome used in four studies 9 –11,13 and ACT outcome used in one study 11 indicated that patients with asthma receiving tian jiu therapy could better maintain and control their asthma symptoms and have improved quality of life.
Three studies 8,10,12 used IgE as a biomarker to measure the outcome; two studies 8,10 used Eos. Both biomarkers indicated that the change in the treatment group was significant in comparison to the control group. However, there is a high degree of heterogeneity among studies; thus, the current evidence cannot be used to conclude that tian jiu therapy is more effective than blank control or medicine in treating patients with asthma. In a recent comprehensive study on biomarkers for asthma, only multiallergen screening was recommended as a core asthma outcome; complete blood count to measure IgE and eosinophils is recommended only as a supplemental measure. 16
One study 13 used pulmonary function as an outcome measure. The researchers reported that improvements in peak expiratory flow and forced expiratory volume in 1 second in the treatment group were better than those in the control group (p<0.01). However, because of this limited number of studies and limited sample size, the results are inconclusive.
In the only study 13 that assessed recurrence rate, this rate was significantly lower in the tian jiu therapy group than in the control group. Again, because of the limited number of studies and limited sample size, the results are inconclusive.
Asthma is a chronic, heterogeneous disease with complex mechanisms. Asthma management must optimize the patient's current clinical state and prevent adverse outcomes, including asthma exacerbation and adverse effects of therapy. 17 It is obvious that the efficacy of an asthma treatment must be evaluated by using several outcome measures and that its long-term effect needs to be observed. None of the selected studies on tian jiu therapy evaluated long-term effects or accumulated effects of tian jiu. In actual practice, patients are recommended to undergo tian jiu therapy for 3 consecutive years to obtain a good clinical result; 18 however, few studies have evaluated the cumulative effects of tian jiu therapy.
Limitations
Various factors limit the conclusions of this meta-analysis. In terms of methodological quality, some studies had unclear randomization procedures, and no studies described the methods used to conceal the allocation sequence. No studies reported complete or adequate blinding. These problems introduce a high risk of performance and detection bias. Included studies examined only the short-term outcomes of tian jiu therapy, without follow-up, and thus cannot provide information on long-term effect of tian jiu therapy. Some outcome measures, such as pulmonary function, recurrence rate, and quality of life, were reported in single study, and thus data couldn't be pooled for quantitative synthesis. Only six studies met the inclusion criteria. Grey literature was not included in this meta-analysis; thus, this analysis may overestimate the efficacy of tian jiu therapy and introduce publication bias. Because of a high degree of heterogeneity among studies in the statistical analysis of biomarkers (IgE and Eos), it is not possible to determine whether tian jiu therapy benefits immune response.
Further study
Although all the studies suggest that tian jiu therapy has a positive effect on patients with asthma and even performs better than common drugs in controlling some asthma symptoms, further studies with low risk of bias are necessary to evaluate the efficacy of tian jiu therapy. Studies must also evaluate the long-term and cumulative effects of tian jiu therapy so as to establish a common treatment protocol. Apart from achieving and maintaining control of symptoms, the goals for successful management of asthma also include maintaining normal activities level and preventing asthma exacerbation. The National Institutes of Health asthma guidelines suggest the use of patient-reported outcomes, including health-related quality of life, to assess asthma control. 17 The same approach should also be adopted for further study of tian jiu therapy. Further investigation on the efficacy of similar medication pasting on selected acupoints in other times of the year may also be worthwhile.
Conclusion
The current meta-analysis indicates that tian jiu therapy has a positive effect on adults with asthma. However, all included studies also present various risks of bias and do not provide enough evidence to fully support the clinical effectiveness of tian jiu therapy. Future multi-center, randomized, controlled trials should be designed to increase the strength of evidence; the therapy's long-term and cumulative effect should also be studied. The cost of administration of tian jiu is relatively low, and few adverse effects have been reported; it could be a recommended adjuvant treatment for asthma management when more clinical evidence is established.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References

 .
.