
Abstract
Objective:
To examine whether hippotherapy has a clinically significant effect on gross motor function in children with cerebral palsy (CP).
Design:
Randomized controlled trial.
Setting:
Outpatient therapy center.
Participants:
Ninety-two children with CP, aged 4–10 years, presenting variable function (Gross Motor Function Classification System [GMFCS] levels I–IV).
Intervention:
Hippotherapy (30 minutes twice weekly for 8 consecutive weeks).
Outcome measures:
Gross Motor Function Measure (GMFM)-88, GMFM-66, and Pediatric Balance Scale.
Results:
Pre- and post-treatment measures were completed by 91 children (45 in the intervention group and 46 in the control group). Differences in improvement on all three measures significantly differed between groups after the 8-week study period. Dimensions of GMFM-88 improved significantly after hippotherapy varied by GMFCS level: dimension E in level I, dimensions D and E in level II, dimensions C and D in level III, and dimensions B and C in level IV.
Conclusion:
Hippotherapy positively affects gross motor function and balance in children with CP of various functional levels.
H
Researchers distinguish between two types of equine-assisted activities and therapies (EAAT): hippotherapy and therapeutic horseback riding (THR). In hippotherapy, the therapist sets goals aimed at improving the participant's impaired body function, while the goal of THR is to teach the rider how to ride a horse. Patients undergoing hippotherapy take no active control of the horse and merely receive its influence, while in THR the rider is allowed to control the horse. 10 –12,14
EAAT appears to have positive effects on gross motor function, with limited evidence. 11 However, a recent meta-analysis found insufficient evidence for any therapeutic or maintenance effects of EAAT on gross motor function in children with CP. 10 Two randomized controlled trials (RCTs) found no significant effects of THR on gross motor function as assessed by the Gross Motor Function Measure (GMFM). 15,16 Davis and colleagues 15 randomly assigned children with CP (aged 4–12 years), whose disability severity followed the Gross Motor Function Classification System (GMFCS; levels I–III), to an intervention (a 30-minute THR program administered weekly for 10 weeks) or a control group. They found no significant difference between the changes in GMFM-66 scores between groups after the intervention. MacKinnons and colleagues 16 provided a THR program (1 hour weekly for 6 months) to 10 children with CP having mild or moderate degrees of impairment. GMFM scores did not significantly improve with THR compared with scores in 9 controls. However, these two studies examined the effect of THR, not hippotherapy. An RCT with a larger sample size and consistent protocol is necessary to determine the effects of hippotherapy on gross motor function in children with CP.
Thus, the current study was conducted to evaluate the effects of hippotherapy on gross motor function in a relatively large group of CP children with various functional levels. The hypothesis was that there would be a greater improvement of GMFM scores in the hippotherapy group than in the control group and that the pattern of improvement might differ according to the functional status of children with CP.
Materials and Methods
Participants
The Institutional Review Board of the Samsung Medical Center (Seoul, Republic of Korea) approved this study protocol. Informed consent was provided by parents or guardians before enrollment. Children suitable for this study were identified using the Samsung Medical Center database. Inclusion criteria were (1) diagnosis of CP, (2) body weight less than 35 kg, and (3) age between 4 and 10 years. Exclusion criteria were (1) having received a botulinum toxin injection within 6 months, (2) having a selective dorsal rhizotomy or orthopedic surgery within 1 year, (3) displaying severe intellectual disability, (4) experiencing uncontrolled seizures, or (5) displaying poor visual or hearing acuity. The body weight limit was 20% of the horse's weight, as recommended by the American Hippotherapy Association. The maximum allowed weight considering the size of the ponies used was 50 kg.
A total of 124 children were initially assessed for eligibility, but 32 were excluded because of screening failure (n=27) and or a decision not to participate (n=5) (Fig. 1). Thus, 92 children were randomly assigned to two groups (hippotherapy, n=46; controls, n=46). Two children in the hippotherapy group (one with GMFCS level III and one with GMFCS level II) and three children in the control group (one with GMFCS level I and two with GMFCS level II) were exposed to the hippotherapy condition before the study in a twice-weekly program held for 8 to 16 weeks. Table 1 shows the clinical characteristics of children included in the analysis.
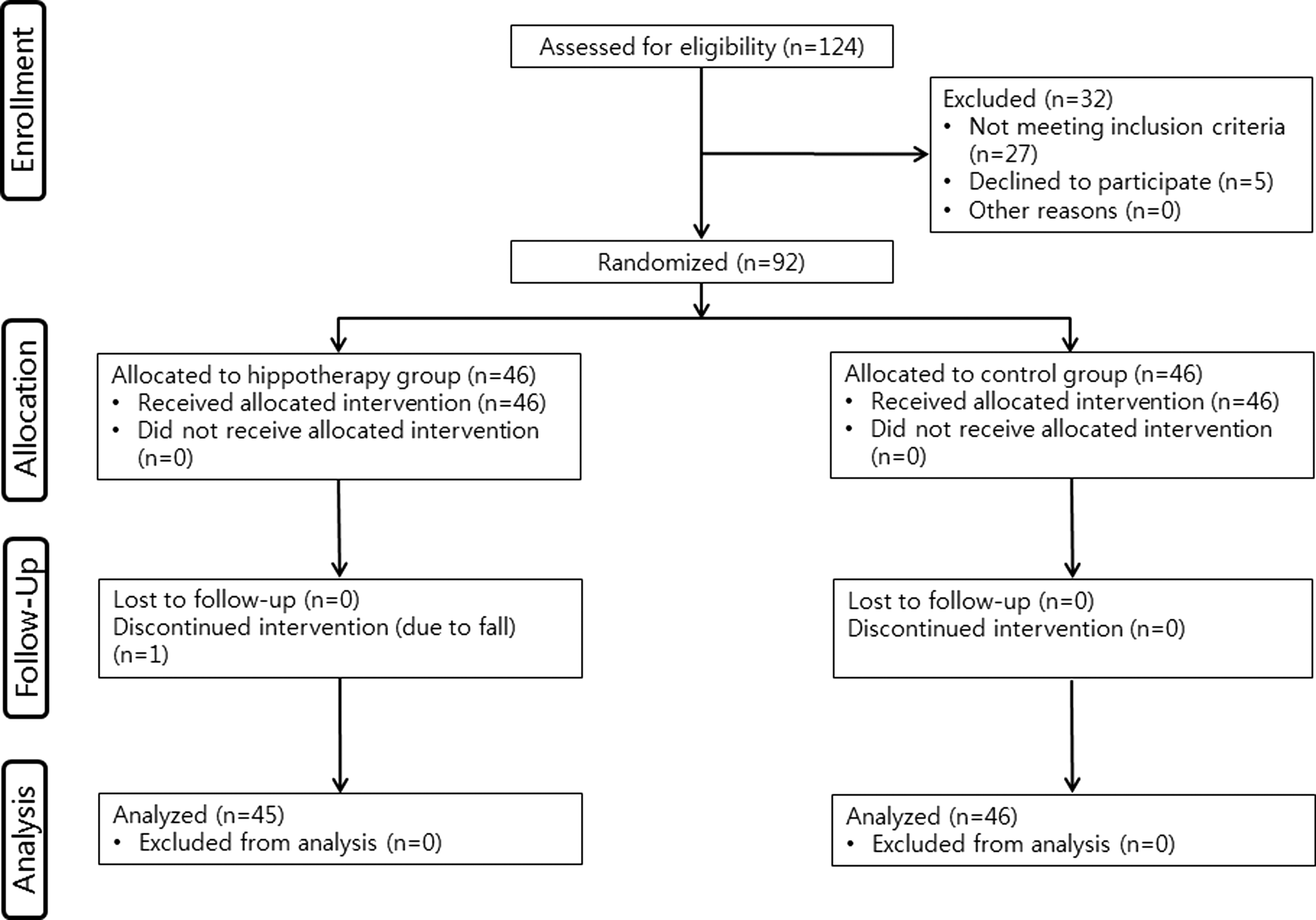
Consolidated Standards of Reporting Trials flow diagram.
Values expressed with a plus/minus sign are the mean±standard deviation.
GMFCS, Gross Motor Function Classification System.
Study design
This study was an RCT. An independent statistician performed the randomization using computer-generated random blocks of 2 or 4, stratified by GMFCS level (I–IV). When consenting to participate, the project officers, participants, and participants' parents or guardians were blinded to whether the child would be placed in the hippotherapy or control group.
Sample size calculation
Sample size calculations were based on 90% power for an independent t-test to compare changes in outcomes from baseline to follow-up between the groups. Forty-one children in each group were needed to detect a mean change of 1.6 points between groups, with a 2.2-point standard deviation (SD) in GMFM-66 scores. This mean change in GMFM-66 scores can be considered a clinically meaningful change in motor function. 17 To allow for 10% nonparticipation at follow-up, the required sample size was 46 children per group. The plan was to recruit a similar number of participants at each GMFCS level: 12 at level I, 12 at level II, 12 at level III, and 10 at level IV for each group.
Treatment
Children in the hippotherapy group received 30 minutes of private hippotherapy (1 child per therapist) twice a week for 8 weeks (16 sessions), in addition to conventional physiotherapy. Hippotherapy sessions were provided by Samsung RD Center of Samsung Equestrian Team in an 18 m×27 m indoor riding arena located in Gyeonggi-do, Republic of Korea. Sessions were conducted by physical therapists extensively trained in hippotherapy by the American Hippotherapy Association and had obtained level II status. Horses walked during sessions with a trained, experienced horse leader. Two volunteers walked along either side of the horse, assisting participants. Thus, four people assisted in one hippotherapy session: a therapist, a horse leader, and two side walkers.
A soft saddle (made of fleece) was selected to maximize contact between participants and the pony. For safety, all patients wore helmets.
Four ponies were trained by staff to participate (mean height±SD, 135±7.5 cm; mean weight, 294±44.6 kg). Ponies and participants were matched according to the size and functional status of the children and the movement characteristics of the ponies as best as possible.
This study used the hippotherapy treatment protocol described by McGibbon and colleagues, 3 directed by the therapist. The protocol included muscle relaxation; optimal postural alignment of the head, trunk, and lower extremities; independent sitting; and active exercises (stretching, strengthening, dynamic balance, and postural control).
Children in the control group received 30 minutes of home-based aerobic exercise (walking or cycling) twice a week for 8 weeks with conventional physiotherapy.
Outcome measures
GMFM
This study applied the GMFM-88, a widely used, validated tool for assessing motor function in children with CP. 18 It is also an outcome assessment tool for clinical interventions in children with CP and those with delayed motor development. 19 The GMFM-88 consists of 88 items in five dimensions: (A) lying and rolling; (B) sitting; (C) crawling and kneeling; (D) standing; and (E) walking, running, and jumping. The GMFM-88 total score and dimension scores for B, C, D, and E were calculated. The GMFM-88 was administered before and after the intervention by the same blind examiner. GMFM-66 scores were calculated from the GMFM-88 using the Gross Motor Ability Estimator.
Pediatric Balance Scale
To assess balance, the Pediatric Balance Scale (PBS) was used. This 14-item, criterion-referenced measure evaluates functional balance in everyday tasks. 20 The items assess the functional activities that children must perform to safely and independently function within the home, school, or community. This scale has also been validated for children with CP 21,22 and has good test–retest and interrater reliability when used with school-age children with mild to moderate motor impairment. 20 The same blinded examiner administered the PBS before and after the intervention.
Statistical analyses
Data were analyzed by using paired t-tests or Wilcoxon signed-rank tests to compare changes from baseline to postintervention within groups, depending on whether data were normally distributed (according to the Shapiro-Wilk test). Changes in outcome measures between groups were assessed using independent t-tests or Mann-Whitney tests. The significance level was set at <.05. All analyses were performed with SPSS software, version 19.0 (IBM Corp., Armonk, New York).
Results
Demographic characteristics
One participant (GMFCS level III) in the hippotherapy group dropped out; thus, 45 and 46 children in the hippotherapy and control groups were available for the final analysis, respectively. The groups were similar in terms of sex, age, GMFCS level, neuromotor type, laterality, body weight, height, history of surgery, and amount of physiotherapy they were currently receiving (Table 1).
GMFM
Baseline GMFM-66 and GMFM-88 total and dimension scores did not significantly differ between groups. GMFM-66, GMFM-88 total, and GMFM dimensions B, C, D, and E increased significantly in the hippotherapy group (p<0.05). In contrast, no significant change was noted in the control group between the two assessments. Changes in the GMFM-66, GMFM-88 total score, and GMFM dimensions B, C, D, and E scores significantly differed between the hippotherapy and Control groups (p<0.05). When a secondary analysis was performed according to GMFCS levels, GMFM-88 total score was significantly increased among all levels and GMFM-66 scores were significantly increased for children with levels II, III, and IV. Dimensions of GMFM-88 that demonstrated significant improvement after hippotherapy varied by the patients' GMFCS level; dimension E in level I, dimensions D and E in level II, dimensions C and D in level III, and dimensions B and C in level IV (Table 2).
GMFM-66 values are expressed as mean±standard deviation. GMFM-88 values are expressed as mean percentage±standard deviation.
Paired t-test or Wilcoxon signed-rank test to compare between preintervention and postintervention within groups.
Independent t-test or Mann-Whitney test to compare changes between hippotherapy group and control group.
GMFCS, Gross Motor Function Classification System; GMFM, Gross Motor Function Measure; A, lying and rolling; B, sitting; C, crawling and kneeling; D, standing; E, walking, running, and jumping.
PBS
Baseline PBS scores did not differ between groups (p>0.05). After the intervention, the hippotherapy group showed a significant improvement in PBS scores (p<0.05), but no significant difference was observed in the control group. The hippotherapy group showed increased PBS scores compared with the control group (p<0.05) (Table 3). In a secondary analysis according to GMFCS levels, PBS significantly increased in all functional levels (Table 3).
Values are expressed as mean±standard deviation.
Paired t-test or Wilcoxon signed-rank test to compare between preintervention and postintervention values.
Independent t-test or Mann-Whitney test to compare changes between hippotherapy group and control group.
Participant attendance
Of the 45 children in the hippotherapy group, 11 missed one session, 5 missed two sessions, 3 missed three sessions, and 2 missed four sessions.
Adverse effects
Two participants (2.2%) fell during the study period. No major adverse effects, such as brain injury or fractures, were found after an immediate medical examination that included radiography. One participant returned to the therapy and finished, while the other dropped out.
Discussion
This study appears to be the first RCT showing the beneficial effects of hippotherapy on gross motor function in children with CP. Children undergoing hippotherapy had significant improvements in GMFM scores (both GMFM-66 and -88) and PBS scores. The strengths of the study were the strict inclusion and exclusion criteria, relatively large sample size, and inclusion of children with various functional levels. These factors enable analysis of the functional dimensions showing main effect of hippotherapy according to patients' functional levels.
The GMFM, the primary outcome variable in this study, is the most widely used measure for evaluating CP; indeed, it was used in previous clinical trials to assess the effect of EAAT on children with CP. 3,4,7,9,13,15,16 In the present study, GMFM-66 scores, GMFM-88 total scores, and scores on GMFM dimensions B, C, D, and E improved. These results are consistent with those of previous studies reporting improvements in gross motor function after EAAT. 3,4,7,13 McGibbon and colleagues 3 reported that five children with CP (mean age, 9.6 years) showed a significant increase in dimension E scores after 30-minute hippotherapy sessions held twice weekly for 8 weeks. Casady and Nichols-Larsen 7 also reported significant differences in GMFM total scores after hippotherapy administered once weekly for 10 weeks among 10 children with CP aged 2.3–6.8 years. In addition, Kwon et al 13 reported significant improvement in dimension E scores and GMFM-66 scores among 16 children with bilateral spastic CP after hippotherapy (30 minutes twice weekly for 8 weeks). In contrast, two studies by Davis et al. 15 and MacKinnon et al. 16 reported no significant improvement of GMFM scores in their intervention groups compared with controls. These two studies used THR, but not hippotherapy; furthermore, interventions used by Davis et al. were less intense (30 minutes of THR weekly for 10 weeks) than that used in the current study.
Previous researchers investigating the effect of EAAT on motor function of children with CP have mostly included participants with mild to moderate disability (GMFCS levels I–III) 3,13,15,16 or did not report GMFCS levels. 3 For example, Davis et al 15 randomly assigned children with CP GMFCS levels I–III into an intervention or control group, and MacKinnons et al 16 conducted their study with children with CP who had mild to moderate impairment. Kwon et al 13 also included patients who had bilateral spastic CP with GMFCS levels of I or II. In the current study, gross motor function and balance improved among children with CP, not only those with GMFCS levels I–III but also those with GMFCS level IV. However, the dimensions that show main improvement effect of hippotherapy differed according to their GMFCS levels. Thus, hippotherapy can be considered helpful for children with various functional levels; notably, significant improvements were observed among the dimensions for participant goals.
The observed improvement in PBS scores in this study was consistent with and thus strengthens the findings of previous studies, 2,8,13 which have reported significant improvements in postural control after THR or hippotherapy. Bertoti 2 reported that children with spastic CP showed significant improvement in posture, measured with the Posture Assessment Scale. Shurtleff et al. 8 also reported that hippotherapy improved the abilities of children with CP to control trunk and head movements. In addition, the previous study, 13 a nonrandomized prospective controlled trial, demonstrated an improvement in PBS after hippotherapy in children with CP.
Locomotor impulses from the horse's back are transferred to the participant at a frequency of 90–110 impulses a minute (1.5–1.8 Hz) in three movement planes. 23 During a 30-minute hippotherapy session, children could have experienced approximately 2700–3300 repetitions of forced-use postural challenge. As McGibbon et al. 5 proclaimed, motor strategies that could be improved with hippotherapy included control of mediolateral and anteroposterior postural sway, postural adaptation to a changing environment, anticipatory and feedback postural control, and more effective use of multisensory inputs related to posture and movement.
Habilitation of postural control in children with balance deficit should include activities that address the musculoskeletal, motor, and sensory processing rate-limiting factors. Further, these intervention should focus on static and dynamic equilibrium tasks during mass and random practice so that children can actively participate. 24,25 Hippotherapy is a task-oriented training that meets the above requirements. 25 For optimal skill acquisition in task-oriented training, training must be sufficiently challenging to facilitate learning, progressive and adaptable so users will continue to acquire or refine new skills, and sufficiently interesting and meaningful to engage the user in active problem solving. 26 The tasks must also be salient to the performer to influence the person-task-environment triad. In the current study, most participants were experiencing hippotherapy for the first time; thus, it could be presented as a set of novel tasks involving massive postural challenges. Furthermore, participants found hippotherapy to be an exceedingly enjoyable and meaningful activity. Another potential reason for the beneficial effect of hippotherapy could be the human–horse interaction acting as a powerful motivator for engaging children's participation. 27
This study could not evaluate the sole effect of hippotherapy on motor function because it did not control for the participants' other therapeutic activities. Because hippotherapy is still regarded as a complementary therapy in many countries, the study did not control for participation in conventional physiotherapy. Moreover, the therapist did not completely supervise aerobic exercises performed by the control group. However, considering that children in both groups received enough conventional physiotherapy (3 hours per week), the differences in improvement between the two groups after 8 weeks of intervention might be counted as an effect of hippotherapy. Another limitation is that despite the possible beneficial effect of complementary hippotherapy, this study did not determine its cost-effectiveness; hippotherapy needs more assistance (four versus one assistant) and therefore usually incurs higher costs (e.g., maintaining horses, an arena, and training volunteers) than conventional physiotherapy. Finally, the current study only showed the short-term effects of hippotherapy in children with CP. Future studies must assess the maintenance effects of hippotherapy over time.
In conclusion, this study demonstrated the beneficial effects of hippotherapy on gross motor function and balance in children with CP. Hippotherapy provided by licensed health professionals may be used in conjunction with standard physical therapy for improving gross motor function and balance in children with CP at various functional levels.
Footnotes
Acknowledgments
This research was supported by IN-SUNG Foundation for Medical Research CB08161.
Author Disclosure Statement
No competing financial relationships exist.