
Abstract
Introduction:
Neck pain presents a tremendous physical and financial burden. This study compared the efficacy of the complementary and alternative medical treatments of integrative muscular movement technique (IMMT) and Swedish massage on neck pain in women of occupation age, the largest demographic group with neck pain.
Methods:
A total of 38 women were assigned to IMMT (n=28) or Swedish massage (n=10) in a blinded manner. Both groups received eight 30-minute treatments over 4 weeks. Cervical range of motion (ROM) in flexion, extension, sidebending, and rotation was measured before and after treatment. Each patient's pain was assessed by using an analogue pain scale of 0–10.
Results:
Compared with the Swedish massage group, patients receiving IMMT experienced a significant increase in ROM in cervical flexion (p<0.001), extension (p<0.001), sidebending (p<0.05), and rotation (p<0.001). Absolute change in pain for IMMT was −1.75 units compared with −0.3 units for Swedish massage (p<0.05).
Conclusion:
Patients receiving the IMMT demonstrated significantly improved cervical ROM in every movement measured compared with Swedish massage. Inclusion of the IMMT in a treatment regimen for chronic neck pain may lead to decreased pain and increased cervical ROM. These positive effects of the IMMT intervention may have a role in enhancing functional outcomes in patients with neck pain.
Introduction
N
In 2008, the multidisciplinary Burden of Musculoskeletal Disease in the United States (BMDUS) study was conducted to determine the effect of neck and back pain on the U.S. population. The BMDUS study showed that the two largest age groups seeking health care for NP were 18–44 years and 45–64 years, which encompass the general age for the working population. 7 Although the complete financial toll of NP is difficult to estimate, the number of work days lost due to NP alone in just 3 months of 2008 was 203,121,000; women made up the majority of this, accounting for 120,348,000 days. 7
The most common treatment prescribed by physicians for neck pain includes non-steroidal anti-inflammatory drugs (NSAIDs) or acetaminophen; however, if those prove ineffective, narcotics or muscle relaxants are often recommended. 11 Although considered to be less hazardous than opioids, NSAIDs have several adverse effects, including gastrointestinal ulcers, which may lead to perforation and bleeding of the intestines. 12 The adverse effects of opioid-derived narcotics include nausea, vomiting, dizziness, and constipation. 13 Previous studies using these compounds often had a significant loss of participants midtrial (30%–40%) due to the harsh nature of the adverse effects. 14 –16
When these mainstream treatments fail or lead to undesired effects and diminished quality of life, alternative and complementary treatments, including massage therapy, become a practical option. Many studies have shown that massage therapy is beneficial for chronic and acute NP by reducing the pain and increasing neck function, as well as improving quality of life. 17 –19 However, as noted in the Cochrane review on massage for mechanical neck disorders, caution must be taken in drawing conclusions from massage trials. The review showed that the inclusion of poor-quality studies was deleterious to the efforts of creating clinical guidelines for determining the efficacy or effectiveness of massage therapy on chronic neck pain. 20 It is important to have evidence-based results obtained by using objective observation, as well as to properly define the types of manual therapy performed, in order to strengthen the understanding of manual techniques most beneficial for neck pain.
In understanding where the integrative muscular movement technique (IMMT) sits within the field, it is best to first define the types of manual techniques. Manipulation usually refers to the use of high-velocity joint movement, as seen in the chiropractic field. 17 In contrast, mobilization involves slower oscillations of the joint, which are often combined with low-impact exercises that are intended improve range of motion (ROM) and strength to help patients return to their normal daily function; mobilization is most often applied in physical and occupational therapies. 18 Massage therapy differs from both of the preceding therapies because it involves the handling of the soft tissues, often times musculature, to normalize tissue and stimulate blood flow. 17
The IMMT is a novel therapeutic massage technique that uses aspects of mobilization without active muscle contraction. The current authors previously published a case series demonstrating that IMMT successfully decreased pain and increased cervical ROM in two patients while enabling one patient to cease using narcotic pain relievers. 21 The current pilot study examined client cervical ROM, measured objectively, to compare IMMT with Swedish massage as a complementary treatment for neck pain in women who are in the age groups with the highest occurrence of chronic neck pain.
Materials and Methods
Study design
This study was designed to compare the efficacy of IMMT and Swedish massage for patients with chronic neck pain and decreased range of cervical motion (Fig. 1). Recruitment, measurement, and treatment were performed in the clinical setting at the Massage Center of Delaware, Wilmington, DE. The study was controlled for bias by massage therapist by recording each patient's self-reported pain and objectively measured ROM, then handing over the sealed information to the investigators at the University of Delaware, Newark, DE. The investigators did not review or analyze the information until the treatment period concluded. Furthermore, to further prevent bias, investigators at the University of Delaware performed analysis without assistance from the therapist. Three forms of analysis were performed: within comparative group (IMMT or Swedish massage), between-group comparisons (IMMT vs. Swedish massage), and age group comparisons within study groups. The University of Delaware institutional review board approved this pilot study.

Study design of integrative muscular movement technique (IMMT) comparison with Swedish massage. Recruitment, randomization, range of motion (ROM), and pain measurement, as well as treatments (Swedish massage or IMMT) were carried out at the Massage Center of Delaware. Measurements were then sealed and handed over to the investigators at the University of Delaware for statistical analysis within and between study groups.
Participant recruitment
Thirty-eight women were recruited for this study by means of locally posted flyers and referrals. Inclusion criteria included self-reported neck pain; participants were excluded if they lacked complete cervical anatomy. Before their initial treatment, participants filled out a general health history survey. Basic patient demographic data, including age range, race, and sex, were also obtained. All trial participants gave informed consent. The participants were compensated in the form of a greatly reduced billed rate of treatment per visit; this discount was applied to cover the cost of consumables used in the study. Participant retention was tracked; one patient was lost to follow-up because of an unrelated medical condition (Lyme disease).
Therapist profile
The massage therapist who created this technique was the principle investigator responsible for all treatments (experimental IMMT and comparative Swedish massage), as well as all measurements of ROM. The massage therapist has over 12 years of experience in massage therapy. He is licensed in the state of Delaware for deep muscle therapy and shiatsu massage by completion of a 600-hour and 200-hour curriculum on each technique, respectively.
Randomization and interventions
Patients were randomly assigned to experimental treatment (IMMT) or control treatment (Swedish massage) and were blinded to treatment assignment. In both groups, TheraPRO Massage Gel (Massage Warehouse, Bolingbrook, IL) was used; all participants received eight 30-minute treatments over the course of 4 weeks.
IMMT was designed to incorporate principles of myofascial release, reduce myofascial adhesions, and combine stretching and compression components to the muscle to increase ROM and reduce the effects of trigger points. The goal is to override the muscles' tendency to contract when forcefully stretched. This approach focuses on four major muscle groups of the cervical region: the sternocleidomastoid, the scalene muscle group, the splenius muscle group, and the suboccipital muscle group, as previously described. 21 In brief, IMMT involves isolating an individual muscle group while passively moving the associated joint through the muscle group's direction of extension and compression.
Swedish massage, or “classic” massage, was used as the comparative technique. The Swedish massage group received light to medium pressure over the cervical region, targeting muscles, tendons, ligaments, fascia, connective tissue, and lymphatic vessels. The purpose of Swedish massage was to generally relax the client's muscles, relieve stress, and promote general wellness. In both treatments, a relaxing environment was created through low light levels, quiet music, and little noise intrusion.
Outcomes and measurements
Before the treatment, each patient's self-reported pain levels were recorded by using a 0–10 verbal pain scale (0 being no pain and 10 being the most extreme pain). In addition, several motions were objectively measured in opposing directions on the cervical axis (flexion, extension, sidebending, and rotation) for each patient before and after each treatment. Flexion and extension were quantified by aligning the axis of the goniometer with the center of the ear while the stationary arm was aligned vertically with the head and the moving arm tracked the tip of the nose. Sidebending was quantified with the axis of the goniometer aligned with the seventh cervical vertebra, while the stationary arm was aligned vertically with the external occipital protuberance of the skull and the moving arm tracked the head during sidebending. Rotation was quantified with the axis of the goniometer at the center of the top of the skull while the stationary arm was aligned with the patient's nose and the moving arm tracked the nose during the rotation movement. 21
Analysis
The measured ROM for each movement was graphed as mean±standard error of the mean. For daily changes in ROM, the value for ROM after treatment was divided by the pretreatment baseline (daily fold change=value day1post through day8post/valuebaseline). The residual effect was the fold change from a given day pretreatment value to the previous day pretreatment value (residual fold change=value day3pre/value day2pre). Change in pain values was calculated as the value of pain on day8 minus the value on day1 (change in pain=value day8−value day1). Statistical between-group comparisons were done by using a nonpaired t-test with unequal variants (p-value). Within-group statistical analysis was performed by using analysis of variance with post hoc Tukey-Kramer minimum significant difference. Both analyses were performed by using Excel software (Microsoft Corp., Redmond, WA).
Results
To determine the efficacy of the IMMT method, cervical ROM was assessed for six different motions: flexion, extension, right and left sidebending, and right and left rotation. Daily change in ROM was determined to be the degrees of movement after treatment divided by the degrees of movement before treatment for each movement described above. For Participants undergoing IMMT experienced an increase in the daily change in ROM for all measured parameters (Table 1).
Values are expressed as mean±standard deviation. Range of motion (ROM) is reported in degrees; pain score reflects score on analog scale.
Daily fold change in ROM
Flexion and extension were not included in the results because there was an unequal baseline. Analysis of variance demonstrated a significant difference before treatment; therefore, the difference between experimental and comparative groups could not be determined for flexion and extension ROM (data not shown).
Participants who received IMMT experienced improvements in left and right sidebending, with a rapid increase in ROM for both directions, until day 2 (Fig. 2). This increase in ROM maintained significance (p<0.05) over Swedish massage from day 1 through day 8. Participants receiving Swedish massage demonstrated an unexpected decrease in right sidebending ROM (Fig. 2A); however, at the completion of all of the treatments, there was no significant change over the treatment period for Swedish massage (p>0.05).

Neck sidebending is greatly improved by IMMT. Right
The second metric for IMMT and Swedish massage was cervical rotation, both left and right. IMMT showed an increase in left rotation on days 1 and 2 and then plateaued, while right rotation increased from day 1 to day 3 before reaching a plateau (Fig. 3). For both motions, patients receiving IMMT had a significant increase in rotation over Swedish massage beginning at day 1 and lasting through day 8. Swedish massage actually showed a statistically significant decrease in both left and right rotation on day 4 of the treatment period when compared to baseline (p<0.05). However, it returned to baseline by completion of the treatment period.
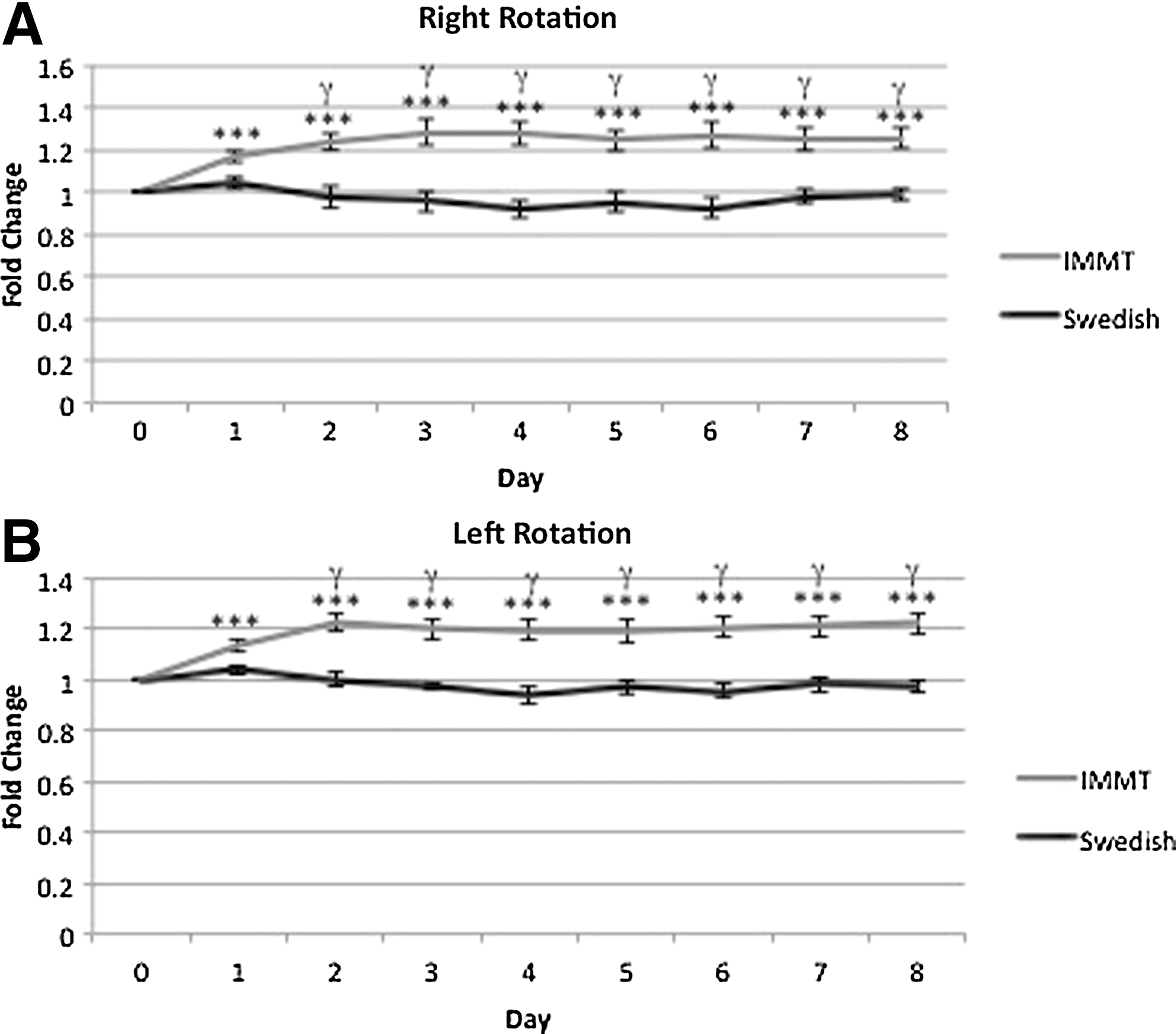
Neck rotation improves with IMMT. Range of motion for rotation is improved in both the right
Residual analysis
The residual effect of IMMT treatment was the fold change in ROM before each treatment divided by the previous days before treatment measurement (e.g., day 2pre/day 1pre). This is a measure of the sustaining effect of the previous treatment. In several cases, the first and second IMMT treatments resulted in a significantly increased residual ROM as compared with Swedish massage. This was noted in left and right rotation on day 2 (p<0.005) (data not shown).
Pain
Pain was measured by using the verbal pain scale. Overall change in pain among clients treated with IMMT was −1.75 units compared with −0.3 units for those treated with Swedish massage (Fig. 4). This is a statistically significant decrease in pain over Swedish massage (p<0.05). In a comparison of daily changes in pain, the trend was that clients receiving IMMT experienced a daily decrease in their pain value, whereas those treated with Swedish massage had no change or slight increases in pain values on average (data not shown).
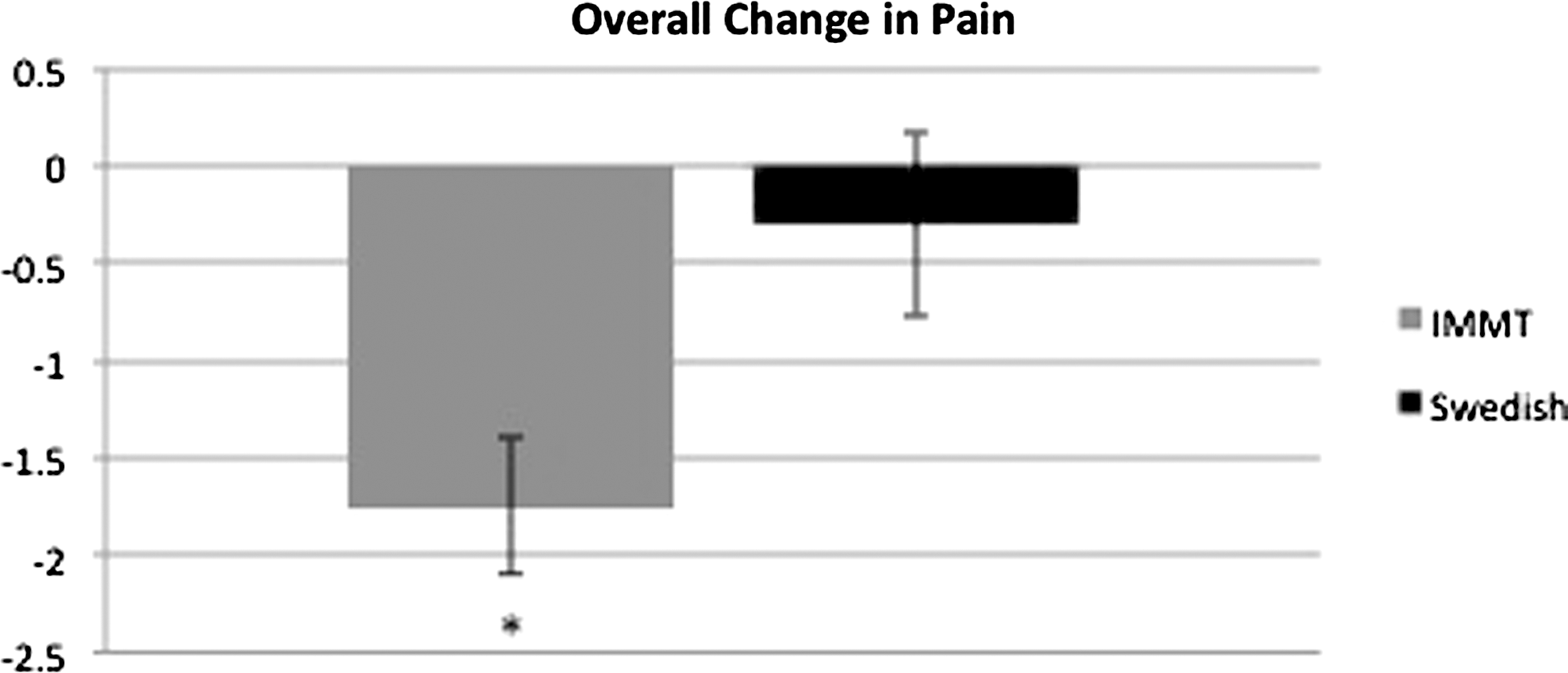
IMMT causes a decrease in neck pain. Subjective neck pain as reported by participants decreases over the total treatment time course an average of−1.75 units as opposed to−0.3 units for Swedish massage. *p<0.05 (IMMT vs. Swedish massage).
Age group comparison
The data were analyzed for comparison between age groups: 20–29, 30–39, 40–49, and 50–59 years. Each IMMT-treated group alone demonstrated an increase in ROM for all the above measured functions. However, there was little to no statistical significance for any extended time period in comparisons between age groups within the IMMT group (data not shown).
Discussion
The point of any clinical trial is to determine whether a technique is similar to or better than the gold standard of treatment. In the case of chronic NP and its alternative or complementary treatment, the standard remains vague. Patients with pain seeking relief often receive Swedish or classic massage and its variants. However, because Swedish massage does not target specific issues, it cannot be classified as therapeutic. Aside from the disadvantage of individual practitioners' interpretation of the technique, which can vary, the benefit from these techniques is poorly understood. In most cases, ROM in the affected area is not recorded before or after treatment. Few evidence-based studies have assessed the efficacy and effectiveness of massage therapy. 22 In fact, while the data on Swedish massage from this study demonstrated a small increase in cervical ROM over the course of the eight treatment sessions, this difference was not statistical significant. Meanwhile, patients receiving IMMT had a measurable increase in cervical ROM in a timely manner. With use of cervical ROM and perceived pain as outcome measures, patients treated with IMMT performed significantly better than those receiving Swedish massage.
The current belief held in the massage industry is that most gain of function and pain relief contribute to the relaxing of connective tissue in either chronic posture-related or acute traumatic injury–related scarring. It is widely known that heat and pressure can alter connective tissue, based on protein denaturation. However, applying the proper amounts of heat and pressure to the connective tissue is time consuming and labor intensive. Also, in most instances, it provides a temporary relief that is lost as the tissues cool and return to their native state of scar tissue. Connective tissue has neither nervous nor circulatory associations, leaving no explanation or mechanism in place to allow for long-term results. The beneficial effect of IMMT treatment is seen days later, as noted by the increased ROM recorded before treatment on days 2–8. The mechanism at this point is not known, but the innervation and vascularization of muscle put in place the machinery necessary for nervous or endocrine regulation.
In manual therapy, it is important to include exercise and stretching in the regimen as long as they do not further damage the affected area. Recent studies have shown that home exercise was more beneficial than medication alone for acute and subacute neck pain 11 and that manual therapies, including stretching and exercise, are also suitable for relieving neck pain. 23 However, there is one caveat to exercise and stretching: Patients may begin to protectively guard the joint and not allow full ROM because they anticipate pain. This guarding and overall joint dysfunction can lead to further chronic neck pain. 24 IMMT does not require muscle activity from the patient because the joint movement is passive. It is believed that this attribute of IMMT allows patients to move beyond their previously guarded ROM endpoints. The average for IMMT-treated patients' daily pain value before treatment consistently demonstrated a decrease in perceived neck pain; this was not seen for patients treated with Swedish massage. The decrease in pain with each treatment likely prevents guarding and may allow the treatment to be more efficacious in returning ROM.
This pilot study has limitations. Among these is the limitation in sample size, which led to the exclusion of flexion and extension. However, there is still valuable evidence to be gained from this study for several other ROMs. Because of the small sample size the cohorts were weighted toward the experimental technique. In addition, the massage therapist that created the technique was also the individual performing both the experimental as well as control techniques. However, during the timeframe of this pilot study this therapist was the only therapist trained to perform the technique that he created. His insight into the technique was vital to proper application. However, there are several instances of similar investigator-initiated research in the chiropractic and physical therapy fields from which this technique is adapted. 25 –28 Finally, the improvement seen with Swedish massage was not statistically significant in the time frame during which IMMT showed vast improvement; this shows another possible limitation to the study. Continuing the treatment for longer periods may show Swedish massage to have a beneficial effect; however, in the timeline of this pilot study those results were not evident.
The positive effects seen for the IMMT technique indicate that this treatment is more efficacious than Swedish massage as an option for patients with musculoskeletal cervical pathologies. This treatment protocol and the related guidelines discussed here can contribute to further studies of patients with chronic NP seeking evidence-based alternative therapy. It is hoped that this pilot study will be followed by a larger clinical study that corrects or accounts for the preceding limitations.
In conclusion, the goal of this pilot study was to compare IMMT to a commonly used massage intervention (Swedish massage). IMMT was designed to incorporate principles of myofascial release, reduce myofascial adhesions, and combine stretching and compression components to the muscle to increase ROM and reduce the effects of trigger points. The outcomes for patients receiving the IMMT treatment were better than expected. These patients experienced greater improvement in ROM than those treated with Swedish massage; however, the group receiving Swedish massage also showed a trend of enhanced ROM.
Footnotes
Acknowledgments
The authors would like to thank Vincent Lanzendorfer, NCTMB, LMT, for his assistance in editing this manuscript.
This study was supported in part by The Center for Translational Cancer Research (B.G.R. and C.R.C.) and the Massage Center (R.C.).
Author Disclosure Statement
One of the lead authors and primary investigators of this pilot study is the creator and instructor of IMMT. This primary investigator's role was to perform all treatments and measurements. The second lead author was responsible for data analysis to prevent bias. No competing financial interests exist.