
Abstract
Objective:
To systematically review and analyze the effects of t'ai chi on balance in older adults.
Methods:
The literature was searched for randomized clinical trials on the effects of t'ai chi on balance, as evaluated by direct, static, dynamic, and mixed measures. The effect sizes (ESs) on balance were calculated by using the standardized mean difference (d) and 95% confidence intervals.
Results:
Thirty-four studies were included. The overall ES of t'ai chi on static balance was medium at 3 months (ES=0.73) and small at 6 months (ES=0.33) for participants with a low risk of falling. For those with a high risk of falling, the ES of t'ai chi on static balance was small (ES=0.47) at 3 months but not significant at 6 months. When compared with the no-exercise group, the ES of t'ai chi on static balance was medium (ES=0.66) at 3 months but smaller at 6 months (ES=0.37). The ES of t'ai chi (ES=0.31) was only significant at 6 months when compared with other exercise.
Conclusion:
The findings of this meta-analysis suggest that persons with a low risk of falling should practice t'ai chi for 3 months to improve their balance. The effects of t'ai chi on balance in those with a high risk of falling were small but significant at 3 months, supporting the safety and effectiveness of t'ai chi. It is important to select reliable and sensitive measures for balance to examine the effects of t'ai chi.
Introduction
P
Exercise using t'ai chi, an ancient Chinese martial art, improves balance in older adults. 5 Indeed, improvement in balance is one of the most commonly observed benefits following practice of t'ai chi. 3 T'ai chi involves slow, gentle, and continuous movements, incorporating unilateral and bilateral weight transfer while bending the knees. This type of constant weight shifting to different target positions is believed to challenge the balance control system to maintain the center of mass within the base of support, consequently leading to improved balance control. 6 Control of the center of mass is essential for balance control. 4 A slip and backward fall is most likely to occur shortly after heel-strike of the swing leg when the body weight is being transferred forward toward the leading foot; Gatts and Wollacott 4 found that 15 sessions of t'ai chi training significantly reduced the incidence of tripping and increased the center of mass anterior/posterior path in older adults with a high risk of falling.
However, the reports included in a meta-analysis on the beneficial effects of t'ai chi on balance remain inconclusive. 7 Such inconsistent findings are likely attributable to lack of control over the type, intensity, and duration of t'ai chi practiced; the characteristics of the study population and the participants' various health conditions; and the wide variations in the use of balance measures. 8 The significant effects of t'ai chi on balance improvement could have occurred as a result of chance, bias, or confounding variables. Various measures have been used to quantify improvement, including self-report tools, dynamic posturography, the Berg Balance Scale, the Tinetti Balance Scale, single-leg stance time, and body sway during quiet stance. Because these measures assess different dimensions of balance, their varied use may have contributed to the inconsistent findings. 9
Furthermore, only a few studies have compared t'ai chi with similar forms of movement therapy, such as yoga or other types of aerobic exercise. 10,11 Most randomized studies have obtained better results for t'ai chi relative to control groups receiving no treatment. 3 The effects of t'ai chi on balance appear to be similar to those of conventional exercise or physical therapy control interventions aimed at improving physical function related to balance. The aforementioned meta-analysis confirmed the beneficial effects of t'ai chi in improving the balance of older adults, but it was suggested that t'ai chi is not necessarily superior to other interventions. 3 The characteristics of the study population should also be considered for the proper selection of an intervention for fall prevention. Previous studies, applied t'ai chi as a low-intensity exercise to older adults, both healthy persons 12,13 and patients with arthritis 14 or other chronic conditions. 15 It is thus necessary to examine the effects of t'ai chi on balance relative to the health condition of the target population (i.e., healthy persons versus those with a high fall risk), the duration of exercise, and the types of balance measures used, as well as by comparing t'ai chi with other types of exercise.
A meta-analysis of this topic would provide a systematic review and statistically comprehensive understanding of the benefits of t'ai chi in balance improvement. In the present study, a systematic literature review and analysis of randomized studies on the effects of t'ai chi on balance were performed, with the following specific objectives: (1) to determine the effect size (ES) of t'ai chi on static balance in groups of patients with low and high risks of falling (referred to henceforth as low-fall-risk and high-fall-risk groups, respectively) at short- and long-term follow-up; (2) to determine the effects of t'ai chi on static balance according to the type of control group at short- and long-term follow-up; (3) to determine the effects of t'ai chi on balance according to outcome measure (i.e., static, dynamic, mixed, and direct) in the low-fall-risk and high-fall-risk groups at short- and long-term follow-up; and (4) to determine the effects of t'ai chi on balance by outcome measures (i.e., static, dynamic, mixed, and direct) according to the type of control group at short- and long-term follow-up.
Methods
Search strategy
The present meta-analysis was performed on the basis of a prospective meta-analysis protocol suggested by the Cochrane handbook. 16 A literature search for potentially relevant articles was conducted by using the following databases: PubMed/MEDLINE, CINAHL, ProQuest Central, Science Direct, Scopus, and Cochrane Library for English-language articles and KISS, NDSL, National Central Library, DBPIA, and KoreaMed for Korean-language articles. Additional manual searches using Google Scholar and reference lists completed the search.
Study selection
Medical Subject Heading (MeSH) terms and Boolean operators were used for the literature search. The most relevant available MeSH terms were “Tai Ji” and “postural balance.” In addition to the MeSH terms, “t'ai chi, Taiji, T'ai Chi,” “balance, stability, equilibrium,” and “randomized controlled trial” (RCT) or “randomized clinical trials” were also used to improve the search results from databases where MeSH terms are not used.
The inclusion criteria were (1) articles published in peer-reviewed English-language journals without specified publication date, (2) articles designed to test the effects of t'ai chi with or without qigong for at least 8 weeks or more (t'ai chi combined with other types of exercise or intervention were excluded), and (3) studies that used an RCT research design. The articles were included in the analysis when the statistical values required to calculate the ES were available. Publication bias was considered by including brief reports and research letters when data were available. When duplicated data were confirmed, those with earlier publication dates and with satisfactory quality assessment were prioritized for inclusion. The selection process complied with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 17
Risk of bias assessment
Three review teams, each consisting of 2 researchers, reviewed 20 or 21 articles by using a quality-assessment tool to verify which ones appropriately followed the conditions of RCTs. The quality-assessment tool was used according to the RCT method checklist of the Scottish Intercollegiate Guidelines Network 18 revised based on Cochrane risk of bias. 19 The content analysis and evaluation were also based on the patient, intervention, comparison, and outcome process. 20 The review team evaluated each article independently using the quality-assessment tool and discussed them at a team meeting to decide whether they should be included.
Data analysis
Comprehensive Meta Analysis software, version 2.0 (Biostat, Englewood, NJ), was used to calculate ESs, for homogeneity testing, and for publication bias assessment. For studies with two or more control groups, the control group used for assessment of the overall effects was selected in the following order of preference: no treatment or wait-list, then active comparator. The standardized difference of means (i.e., ES [d]), 95% confidence intervals, and weights were calculated under the assumption of a fixed-effect model. When homogeneity was not confirmed, a random-effect model was used to calculate the ES. 21 The Z value (p<0.05) was used to identify the statistical significance of the ES, and Q statistics (p>0.10) and I2 statistics were calculated to test the homogeneity of ESs among the included variables. ESs of 0.2–0.5, 0.5–0.8, and>0.8 were defined as small, medium, and large, respectively. 22
Publication bias was considered by examining the symmetry of the funnel plot, the trim and fill method (<10%), and fail-safe numbers (Orwin method; trivial effect=0.20, missing study effect=0).
The studies were analyzed separately for short- and long-term follow-up. For the purpose of this review, a short-term follow-up was defined as the outcome measures taken closest to 12 weeks from 8 to 13 weeks after the randomization; long-term follow-up consisted of measures taken closest to 6 months from 14 weeks or longer.
The series of subgroup analyses were conducted for the participants' physical condition. For the population-based comparison, the participants were dichotomized according to their health condition in terms of fall risk: healthy or low risk of falling versus deconditioned or high risk of falling.
Results
Search strategy
The literature search identified 357 articles to be considered for inclusion. The additional manual search using Google Scholar identified 8 additional articles. The full texts of 61 articles appearing to meet the initial criteria were retrieved for further evaluation. In total, 27 articles were excluded because of a lack of data (n=2), duplicate samples (n=5), t'ai chi intervention combined with another type of exercise (n=4), insufficient quality (n=3), duration of t'ai chi less than 8 weeks (n=1), no randomized groups (n=3), or no measurement for balance (n=9). A final set of 34 articles met all of the inclusion criteria and was included in the analysis (Fig. 1).
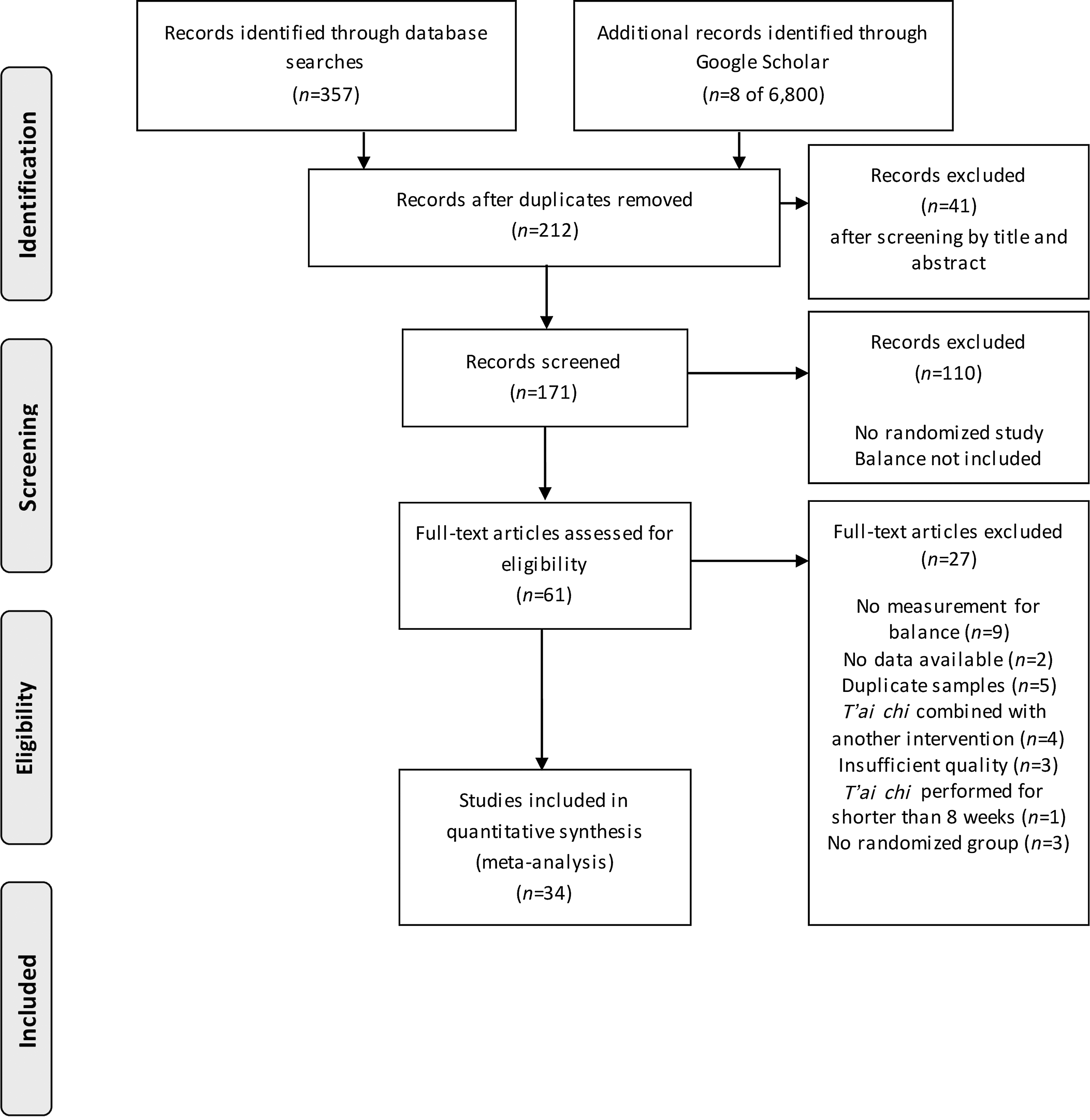
Identification of studies in meta-analysis.
Risk of bias assessment
Table 1 presents the results of the quality assessment of the studies included in the meta-analysis. Although all 34 studies used random assignment, the method used for randomization was not specified in 9. Allocation concealment was specified in 9 studies, and in 14 studies an intention-to-treat protocol was used. Group homogeneity at baseline was confirmed in most of the studies; activities of daily living significantly differed between the groups in one study. 23 Only 8 of 34 studies discussed adverse effect related to t'ai chi, such as mild fatigue (Tsang, Faber), soreness (Song, Tsang), or fall episode (Li).
Adverse effect reported with mild fatigue, pain, or fall.
ITT, intention to treat; NR, not reported.
Study characteristics
Study population
The 34 RCTs were categorized according to population characteristics as healthy elderly with a low risk of falling (n=20) or those with a chronic condition and a corresponding high risk of falling (n=14) (Table 2).
BBS, Berg Balance Scale; COP, center of pressure; EC, eyes closed; EO, eyes opened; FRT, Functional Reach Test; OLS, one-leg standing; POMA, Performance-Oriented Mobility Assessment; PPS, Physical Performance Scale; SD, standard deviation; SOT, Sensory Organized Test; SPPB, short physical performance battery; TC, t'ai chi; TS, tandem standing; TUG, Timed Up and Go test.
Intervention
T'ai chi was provided for 30–90 minutes per session in 27 of the 34 studies (71.1%). The duration of t'ai chi was mostly short term (3–16 weeks, n=22) or long term (20–24 weeks, n=12).
Outcome
The type of balance measure used was categorized as static balance (one-leg standing and Functional Reach Test), dynamic balance (Timed Up and Go test), mixed measure of balance (for both static and dynamic measures combined), or direct measure (mostly computerized measures such as center of pressure and Sensory Organized Test). For research that included various measures of balance, the ES was selected for each representative measure (i.e., for the different categories of measure) or combined (for the same balance measure on the left and right sides). All ESs were analyzed so that they were consistent for direction; a higher score represented better balance. When several measures for balance were investigated in one study, the representative variable was selected for static balance measures, if available, followed by dynamic balance measures or mixed balance measures.
Analysis of ES
A population-based meta-analysis was conducted to determine the ES of t'ai chi by comparing short-term (3 months) and long-term (6 months) measures: low risk versus high risk of falling, t'ai chi versus no treatment/control, t'ai chi versus other exercise, and the four types of balance measure (static, dynamic, direct, and mixed).
Effects of t'ai chi on static balance in the low- and high-risk groups at short- and long-term follow-up
A population-based analysis was conducted for the effects of t'ai chi on static balance, which was the most common measure of balance in the included studies. There were two groups: The low-risk group comprised elderly, postmenopausal women, and the high-risk group comprised people with a preexisting health condition or a frail physical condition.
The ES on static balance for the low-risk group was medium (ES=0.73) at 3 months (p=0.002) but small (ES=0.33) at 6 months (p<0.001) with the random-effect model. However, the ES on static balance for those with a high risk of falling was small at 3 months (ES=0.47; p<0.001), but not significant at 6 months (ES=0.46; p=0.05) (Table 3).
Meta-analysis based on random-effect model.
AS, asymmetric; CI, confidence interval; ES, effect size; Nfs, fail-safe number; S, symmetric.
Effects of t'ai chi on static balance according to the types of control groups at short- and long-term follow-up
Analysis of the 27 studies that compared t'ai chi with no treatment/control revealed that the ES on static balance was medium (ES=0.66; p<0.001) at 3 months and small (ES=0.37; p<0.001) at 6 months. Seven studies were included in the comparison of t'ai chi versus other types of exercise. The analysis revealed no significant difference in the ES of t'ai chi on static balance at 3 months when compared with other types of exercise, but significant effects were found at 6 months (ES=0.31; p=0.001), indicating that the improvement in balance at 6 months was significantly better for t'ai chi than for other types of exercise (Table 4).
Meta-analysis based on random-effect model.
Effects of t'ai chi on balance by outcome measures in the low- and high-risk groups at short- and long-term follow-up
The effects of t'ai chi on balance as evaluated using static, dynamic, direct, and mixed measures were analyzed in populations with low and high risks of falling. For the population with a low risk of falling, the ESs at 3 months were 0.73 (p=0.002) for static balance, 0.52 (p=0.001) for dynamic balance, followed by 0.47 (p=0.003) for direct measure, and 0.45 (p<0.001) for mixed measure of balance. At 6 months, the largest ES of t'ai chi (0.83; p<0.001) was found by the mixed measure of balance, followed by the direct measure of balance (ES=0.64; p=0.028) and static balance (ES=0.33; p<0.001). The ES of t'ai chi on dynamic balance was not significant at 6 months.
For the high-risk group, the ESs for t'ai chi were small at 3 months: 0.47 (p<0.001) for static balance and 0.33 (p=0.04) for direct measure of balance. The direct measure of balance yielded strong evidence (ES=0.83; p=0.013) for effects of t'ai chi at 6 months. The effects of t'ai chi were not significant for measures of dynamic and mixed balance at either 3 or 6 months in this population (Table 3).
Effects of t'ai chi on balance by outcome measures according to the type of control groups at short- and long-term follow-up
The effects of t'ai chi on balance, as measured by static, dynamic, direct, and mixed measures, were compared among the different types of control groups. When compared with the no-treatment group, the ESs of t'ai chi were significant at 3 months, regardless of the balance measure used, ranging from 0.66 (p<0.001) for static measures to 0.32 (p=0.01) for direct measure of balance. The small to medium effects of t'ai chi on balance remained significant at 6 months.
Compared with other exercise as the control group, the effects of t'ai chi on direct measure of balance was large (ES=0.84; p=0.003) at 3 months and medium (ES=0.52; p=0.002) at 6 months. The ES of t'ai chi on dynamic balance was also significant (ES=0.64; p=0.002) at 3 months but not significant at 6 months. The effects of t'ai chi on static balance were not significant at 3 months, but a small ES was found to be significant at 6 months (ES=0.31; p=0.001). The number of studies was insufficient to enable analysis of the mixed measure of balance (Table 4).
Discussion
Prevention of fall for older adults is important with respect to maintenance of their health status and quality of life, 24 and balance is a vital factor of fall prevention. T'ai chi, which is known to be an effective method of balance training, is especially suitable for older adults because it can be applied more safely than other forms of exercise in this population. 25 In the present analysis, 34 studies yielding quantitative data were systematically reviewed to examine the effects of t'ai chi on balance in older adults with various health conditions. The findings revealed that t'ai chi was effective in balance improvement but that its beneficial effects varied according to the fall-risk stratification of the population, the duration of the exercise (i.e., short or long term), the comparator used (i.e., no exercise control or other exercise), and the type of balance measures implemented.
T'ai chi exercise was effective on static measures in both the low fall risk group and the high fall risk group, yielding a small to medium ES when practiced for up to 3 months. The strong evidence regarding the effects of t'ai chi on static balance was found during the first 3 months for the low-risk group and remained small yet significant when participants continued to practice t'ai chi for 6 months or more. The effect of t'ai chi on static balance was also significant at 3 months for the high-risk group. The findings of this study confirm that t'ai chi is an effective way of improving balance for older adults as well as those at high risk of falling.
The aging process affects muscle strength, 26 the reflexes, 27 flexibility, and body posture maintenance. 28 Therefore, older adults with chronic disease are considered to have poor balance and were thus classified as having a high risk of falling. 29 This population would have a greater potential to improve if they were able to continue practicing t'ai chi for at least 3 months. A systematic review by Liu and Frank 5 also found that t'ai chi was effective on several measures of static balance. However, Leung and Chan 3 failed to confirm that t'ai chi was effective using a static measure of balance: the single-leg stance. This discrepancy may have occurred because their meta-analysis included only 3 studies and used only the single-leg stance as a measure of static balance, while the present investigation analyzed 14 studies along with various measures of static balance.
The present study revealed that the effects of t'ai chi vary according to the risk stratification of the population and the type of balance measures implemented. The effects of t'ai chi on dynamic balance were medium for those with a low risk of falling but not significant for those with a high risk of falling. Similarly, the ES of t'ai chi on mixed measure of balance (static and dynamic) was small at 3 months and became larger at 6 months for the low-risk group, while the effects were not significant for the high-risk group. A few meta-analyses of the population with a high risk of falling have also shown that t'ai chi is ineffective for improving the balance of patients with Parkinson disease, as evaluated using mixed measurement (i.e., Berg Balance Scale, Timed Up and Go test). 30 Furthermore, although t'ai chi was effective in frail elderly persons at improving balance, as assessed using the Berg Balance Scale, its effects were not significant when measured by the Timed Up and Go test. 31
The present findings confirm that the effects of t'ai chi on dynamic balance is consistent for the low-risk group, yet the ES of t'ai chi appears to vary according to the type of balance measures implemented when applied to high-risk populations. One reason for this could be the level of physical functioning or condition of the participants. The characteristic of chronic illness should be considered when choosing the most sensitive and reliable balance measures to examine the effects of t'ai chi on populations with a high risk of falling. The present study found that the ES of t'ai chi on balance, as assessed by direct measures (posturography or computerized measures), was consistently significantly applied both for the low-risk and the high-risk groups measured up to 6 months. Similarly, Liu and Frank 5 conducted a systematic review of 8 studies on balance evaluated by a direct measure (posturography) and confirmed significant effects on 6 studies. However, another meta-analysis by Logghe and Verhagen 7 concluded that t'ai chi was not effective; these authors analyzed two studies using a direct measure of balance. While the short-term effects of t'ai chi on balance analyzed by a direct measure were mostly supported by previous studies, the long-term effects seem to be inconclusive because only a few studies have used a direct measure of balance, and even fewer have applied t'ai chi for more than 6 months.
The effects of t'ai chi on balance may differ according to the comparator: either a no-exercise control group or a group performing other types of exercise. In the present study, the ES of t'ai chi on balance was consistently significant when compared with the no-exercise control group, regardless of the type of measure used. However, when compared with other types of exercise, the ES of t'ai chi was significant only on direct measure of balance both at 3 and 6 months. The effects of t'ai chi on static balance was not significant at 3 months when compared with other exercises but became significant when the participants performed t'ai chi for more than 6 months. The review by Leung and his colleagues 3 also confirmed that a positive effect of t'ai chi was found with varying degrees when compared with other treatments. The present study showed that that t'ai chi could be safely and effectively applied even to persons with a high risk of falling, but the effects of t'ai chi were not conclusive in their analysis when compared with other types of exercise. The positive effects on balance improvement varied when compared with those of other types of exercise according to the type of measures of balance.
In conclusion, the effects of t'ai chi on static balance were consistently supported in 34 randomized clinical trials, yet these effects still need to be scrutinized according to the risk of falling and the type of balance measures implemented. It is important to select the most reliable and sensitive balance measures to examine the effects of t'ai chi while simultaneously considering the risk-of-falling category of the participants. The effects of short-term t'ai chi were mostly small on direct measure of balance, both for participants with low and high risks of falling, but increased when they continued practicing t'ai chi for 6 months or more, and especially among those with a high risk of falling. The short-term effects of t'ai chi on balance tend to be medium or large when compared with other types of exercise, but the long-term effects are inconclusive for those with a high risk of falling due to the variation among the type of balance measures.
Several limitations should be considered in interpreting the findings of the present study. Although an extended search was conducted to minimize the publication bias, the search language was limited to English and Korean, leading to a potential language bias. The tests for funnel plot asymmetry to determine publication bias were not conducted because of the small number of studies in subgroup analysis. Only randomized clinical studies were selected for quality assurance, leading to the small number of studies in subgroup analysis. In addition to the small fail-safe number, the changing values in most studies were more than 10% according to the trim and fill method, which should be considered when applying the findings of the present study.
Conclusion
Balance is one of the essential factors for fall prevention, and exercise interventions, including muscle strengthening, should be applied for a sufficient duration and safely to those with a high risk of falling. 32 The findings of the present study suggest that t'ai chi can be safely and effectively applied for improving balance among those with both low and high risks of falling, even on a short-term basis, and that this improvement mostly persists for the longer term. While those with a low risk of falling need to practice t'ai chi for 3 months to improve their balance, the effects of t'ai chi on balance improvement for those with a high risk of falling were also significant even during the short term, supporting the safety and effectiveness of t'ai chi in this population. The effects of t'ai chi on dynamic and mixed measure of balance were inconclusive in the present study; thus, further analysis is warranted to confirm the effectiveness of this type of balance measure with different populations.
Footnotes
Acknowledgment
This research was supported by Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Education (grant no. 2010-0005455 and 2010-0023125).
Author Disclosure Statement
No competing financial interests exist.