
Abstract
Objectives:
Elevated blood cholesterol levels are a major risk factor for coronary artery disease, the leading cause of death worldwide. Probiotics have been investigated as potential cholesterol-lowering therapies, but no previous studies have assessed the effect of the probiotic yeast Saccharomyces boulardii on cholesterol levels in human volunteers. The objective of this study was to examine the effect of S. boulardii on serum cholesterol and lipoprotein particles in hypercholesterolemic adults.
Design:
This study was a single-arm, open-label pilot study.
Subjects:
Twelve hypercholesterolemic participants were recruited into the study; one dropped out.
Intervention:
Participants took 5.6×1010 colony forming unit (CFU) encapsulated S. boulardii (Saccharomyces cerevisiae var. boulardii CNCM I-1079) twice daily for an 8-week period.
Outcome measures:
Fasting concentrations of cholesterol (total cholesterol, low-density lipoprotein-cholesterol [LDL-C], high-density lipoprotein-cholesterol [HDL-C], and triglycerides), lipoprotein particles (very-low-density lipoprotein-particle [VLDL-P], remnant lipoprotein particle [RLP-P], total LDL-P, LDL III-P, LDL IV-P, total HDL-P, and HDL 2b-P), and additional cardiovascular biomarkers (apo B-100, lipoprotein [a], high-sensitivity C-reactive protein, homocysteine, fibrinogen, and insulin) were measured at baseline, after 4 weeks, and after 8 weeks.
Results:
Remnant lipoprotein particles decreased by 15.5% (p=0.03) over the 8-week period. The remaining outcome measures were not significantly altered.
Conclusions:
In this pilot study, 8 weeks of daily supplementation with S. boulardii lowered remnant lipoprotein, a predictive biomarker and potential therapeutic target in the treatment and prevention of coronary artery disease.
Introduction
C
Various mechanisms of lipid lowering by probiotics have been proposed, including the assimilation and incorporation of cholesterol into bacterial cellular membranes, the binding of cholesterol to bacterial cellular surfaces, and the deconjugation of intestinal bile salts by bacterial bile salt hydrolase. 8 In vitro studies have shown that several strains of Lactobacillus and Lactococcus can remove cholesterol from culture medium. 9 –11 Similar to bacterial strains, the yeasts Saccharomyces cerevisiae and Saccharomyces boulardii can remove cholesterol from laboratory culture medium. 12
S. boulardii is a probiotic and substrain of the more well-known budding yeast S. cerevisiae. Like many other probiotics, S. boulardii has been investigated as a treatment for several acute and chronic gastrointestinal diseases. A recent meta-analysis showed that it effectively prevents antibiotic-associated diarrhea and traveler's diarrhea. 13
Previous human subject investigations that have examined the potential cholesterol-lowering ability of probiotics have focused on bacterial rather than yeast strains, and no previous studies have examined the effect of S. boulardii on cholesterol levels in human volunteers. However, a study in mice showed that animals given feed that had been fermented with S. boulardii and L. casei had significantly lower levels of total and LDL cholesterol than mice given control feed without these probiotics. 14
To our knowledge, previous investigations of the effect of probiotics on cholesterol have not investigated their effect on lipoprotein particles. Similar to standard cholesterol levels, lipoprotein particle levels correlate strongly with the risk of future cardiovascular events. 15 Additionally, some individuals exhibit discordance between cholesterol levels and lipoprotein particle numbers, and lipid-lowering therapies may alter cholesterol levels differently than they alter lipoprotein particles. Therefore, monitoring lipoprotein particles in addition to standard cholesterol levels may provide more extensive assessment and monitoring of cardiovascular disease risk than measuring standard cholesterol levels alone. 15 –17
The current study aimed to collect preliminary evidence on the effect of the probiotic S. boulardii on lipids, lipoprotein particles, and additional cardiovascular biomarkers in hypercholesterolemic adults. As a pilot investigation, this study also aimed to assess the feasibility of the study methods.
Materials and Methods
Subjects
Otherwise healthy adults aged 21–69 years with total cholesterol of 200–275 mg/dL, HDL-C of <70 mg/dL, and body mass index (BMI) of 20–45 kg/m2 were recruited online and via flyers posted on bulletin boards in the Portland, OR, area. The recruitment target was 12 participants. Exclusion criteria were as follows: a previous cardiovascular event, congestive heart failure, pacemaker, arrhythmia, valvular disease, or heart surgery (after the age of 1); history of rheumatic fever or abnormal echocardiogram; family history of premature CAD; diabetes, immunodeficiency disorder, having a central venous catheter, bowel, hepatic, or renal disease, untreated hypothyroidism, cancer within the last 5 years, pregnancy, lactation, or planning pregnancy. Participants were also excluded if they were taking cholesterol-lowering prescription medication, red yeast rice, plant sterols, policosanols, fish oil >2000 mg/day, niacin >500 mg/day, CoQ10 >200 mg/day, encapsulated garlic >6 g/day, Commiphora mukul >800 mg/day, probiotic supplements, or systemic antifungal, corticosteroid, or immunosuppressant medications. Furthermore, participants were excluded if they were planning to make significant dietary or lifestyle changes during the study period or if their blood pressure was >160 mmHg (systolic) or >100 mmHg (diastolic) upon screening. The study protocol was approved by the Institutional Review Board at National College of Natural Medicine. All volunteers provided written informed consent before participation in the study.
Study design
The study was a single-arm, open-label pilot study with S. boulardii supplementation for 8 weeks. Participants were screened over the phone and at an in-person screening visit. Data were collected from qualifying participants at baseline, after 4 weeks, and after 8 weeks of treatment. Eligible participants were instructed to take four S. boulardii capsules with food twice per day. The supplement contained S. boulardii (Saccharomyces cerevisiae var. boulardii CNCM I-1079) and rice starch in a cellulose capsule (Pure Encapsulations, Inc., Sudbury, MA); each capsule contained 1.4×1010 colony forming unit (CFU) per capsule at the study end point as measured through third-party analysis (Exova, Portland, OR). Participants were asked to maintain their usual diet and level of physical activity throughout the study.
Data collection
Blood pressure was measured at the screening visit. Height and weight were obtained for BMI calculation at baseline and at the end of the study. Physical activity level was assessed at each study visit by asking participants to rate their average weekly exercise level over the previous 4 weeks; they were provided with categorical responses in 1.5-hour increments. Blood samples were obtained by venipuncture at the screening, baseline, week 4, and week 8 visits. Participants were asked to fast for 12 hours and to abstain from alcohol for 24 hours before blood draws. Supplement compliance was monitored by daily documentation on study calendars given to the participants and an end-of-study count of returned capsules.
Sample analysis
Serum collected at the screening visit was analyzed for total cholesterol and HDL-C levels by Quest Diagnostics (Seattle, WA) on an Olympus AU5400 analyzer using reagent kits (Beckman Coulter, Brea, CA, for total cholesterol, and Roche Diagnostics, Indianapolis, IN, for HDL-C). Plasma collected at the baseline, week 4, and week 8 visits was analyzed for fibrinogen levels by Quest Diagnostics (San Juan Capistrano, CA) on a Siemens BCS-XP analyzer using Dade Thrombin Reagent (Siemens, Munich, Germany). Serum collected at the baseline, week 4, and week 8 visits was analyzed for total cholesterol, LDL-C, HDL-C, triglycerides, lipoprotein particles (very-low-density lipoprotein particle [VLDL-P], remnant lipoprotein particle [RLP-P], total LDL-P, LDL-3-P, LDL-4-P, total HDL-P, HDL2b-P, and non-HDL-P), apolipoprotein B-100 (apo B-100), lipoprotein(a) (Lp[a]), high-sensitivity C-reactive protein (hs-CRP), insulin, and homocysteine by SpectraCell Laboratories (Houston, TX) using patented technology including analytical ultracentrifugation. 18
Statistical analysis
All statistical analyses were performed using SPSS v.20 software (IBM Corp., Armonk, NY). Data for one participant were not available at the week 8 time point; values of all variables at week 8, for this participant, were imputed using the “last observation carried forward” method, according to study protocol. Five (of 33) measurements of insulin, from two participants, were below the laboratory detection threshold; for analysis, they were set equal to the threshold value of 4 μIU/mL. Similarly, 10 (of 33) measurements of Lp(a), from 4 participants, were set equal to the lower Lp(a) threshold of 5 mg/dL.
As primary results of this pilot study, means and standard deviations of all outcomes were calculated, at each of the baseline, week 4, and week 8 time points. Since week 8 changes are considered primary, baseline-to-week 8 changes and percent change relative to baseline were determined. Primary significance values, for each outcome variable, were calculated using a one-way repeated measures analysis of variance (ANOVA) with time point (baseline, week 4, and week 8) as a within-subjects factor. When the ANOVA is significant, results of unadjusted (Fisher's LSD) post-hoc comparisons for the baseline-to-week 4 and baseline-to-week 8 changes are also presented. All results were subsequently retested according to the same method, but with baseline values included as a covariate. In cases where change in BMI or exercise, over 8 weeks, showed sufficiently strong correlations with change in the outcome (r>0.4), the analysis was repeated with the appropriate covariates of change in BMI or exercise level included.
Results
Subject characteristics
One hundred individuals responded to advertisements and 89 phone screenings were completed, with 52% eligibility. Thirty-six screening visits were completed with 39% eligibility. Twelve participants enrolled in the study, 11 completed the study as part of the intention-to-treat population, and 1 dropped out of the study shortly after the baseline visit because of an acute illness. (Additional recruitment and eligibility details are presented in Supplementary Table S1; Supplementary Data are available online at
SD, standard deviation.
The study population consisted of nonsmoking predominantly Caucasian males who were normotensive and hypercholesterolemic. Based on BMI, 27.3% of participants were of normal weight, 54.5% were overweight, and 18.2% were obese. Two participants were taking stable dosages of fish oil (1000 and 1600 mg daily) and two other participants were taking stable dosages of niacin (20 mg niacinamide in a daily multiple vitamin) within allowable amounts (as per exclusion criteria) during the study; each of these four participants had been taking the supplements before beginning the study for at least six months. None of the participants were taking CoQ10, encapsulated garlic, or Commiphora mukul. Supplement compliance, as monitored by an end-of-study count of returned capsules, averaged 92.1% (with a range of 76.1–100.0%).
Serum lipids and lipoprotein particles
Means and standard deviations of lipids and lipoprotein particles at each study time point are presented in Table 2. Levels of total cholesterol, LDL-C, HDL-C, and triglycerides were unchanged throughout the 8-week study (Fig. 1). VLDL-P, total LDL-P, LDL-3-P, LDL-4-P, total HDL-P, HDL2b-P, and non-HDL-P did not differ significantly over the 8-week period. Remnant lipoprotein particles (RLP-P) decreased throughout the study, with an overall decrease of 15.5% (p=0.03 for repeated ANOVA; Fig. 2). Results of post-hoc comparisons between time points confirm that only the baseline-to-week 8 change in RLP-P is significant (p=0.02). Inclusion of baseline covariates had no appreciable effects on any of the outcome measures (data not presented).
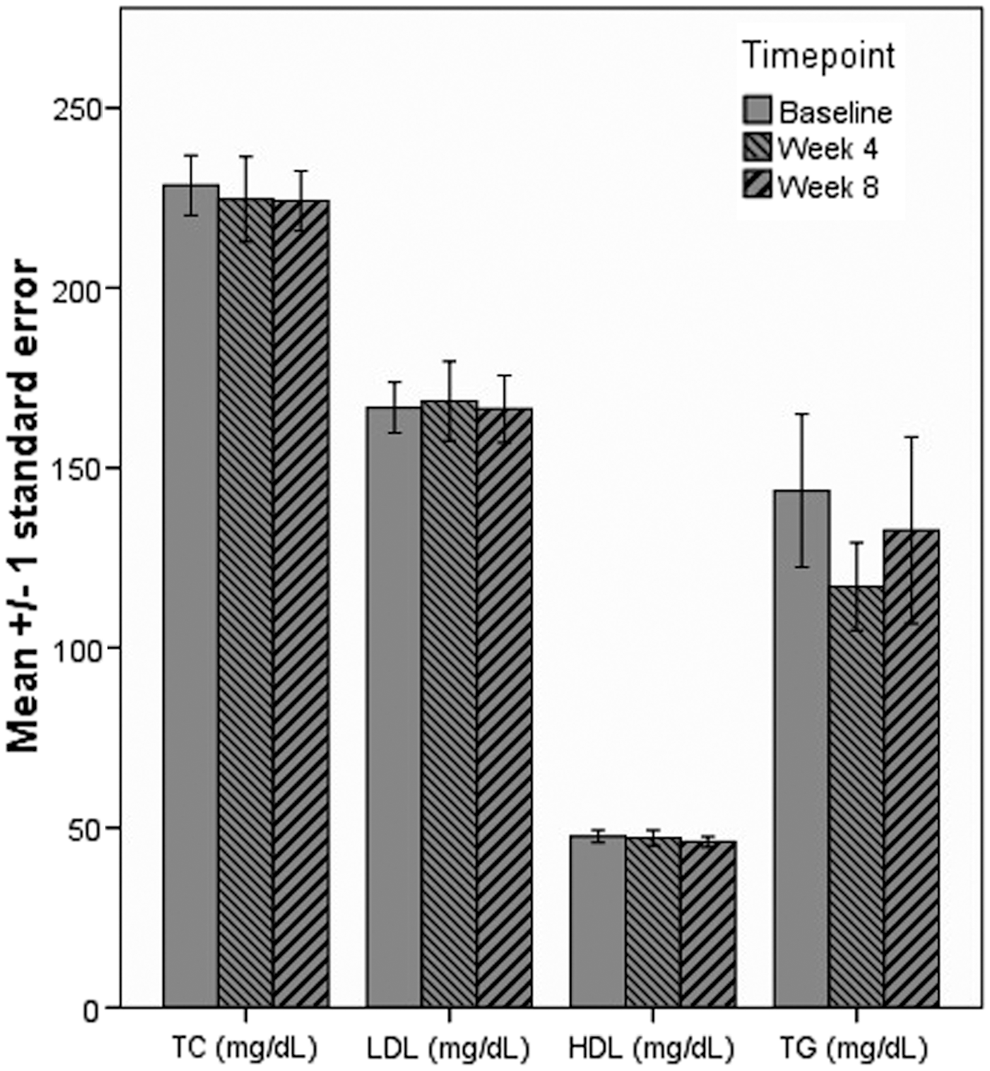
Mean levels of total cholesterol (TC), low-density lipoprotein (LDL), high-density lipoprotein (HDL), and triglycerides (TG) at baseline, after 4 weeks, and after 8 weeks.

Mean level of remnant lipoprotein particles (RLP-P) at baseline, after 4 weeks, and after 8 weeks. p-Value is for a one-way repeated measures ANOVA, with three measurements. Significant difference between time points noted by *p<0.05. ANOVA, analysis of variance.
All p-values for effect of time point in one-way repeated ANOVA. All F(2,20). All additional data are reported as mean±SD.
ANOVA, analysis of variance; HDL-C, high-density lipoprotein cholesterol; HDL2b-P, HDL2b particles; LDL-3-P, low-density lipoprotein-3 particles; LDL-4-P, LDL-4 particles; LDL-C, LDL cholesterol; Non-HDL-C, non-HDL cholesterol; Non-HDL-P, non-HDL particles; RLP-P, remnant lipoprotein particles; TC, total cholesterol; Total HDL-P, total HDL particles; Total LDL-P, total LDL particles; VLDL-P, very-low-density lipoprotein particles.
Additional cardiovascular biomarkers
Levels of apo B-100, Lp(a), hs-CRP, insulin, homocysteine, and fibrinogen did not significantly change over the course of the study (Table 3). The level of hs-CRP increased by 148% (p=0.29) on average, but the increase was predominantly because of one individual. If the data from this outlying individual were excluded, the increase is reduced to 17.9% (p=0.57). Inclusion of baseline covariates had no appreciable effects on any of the outcome measures (data not presented).
All p-values for effect of time point in one-way repeated ANOVA. All F(2,20) except Lp(a) [Huynh-Feldt F(1.40, 14.03)] and hs-CRP [Huynh-Feldt F(1.24,12.41)]. All additional data are reported as mean±SD.
apo B-100, apolipoprotein B-100; hs-CRP, high-sensitivity C-reactive protein; Lp(a), lipoprotein(a).
Exercise frequency, body mass index, and lifestyle factors
None of the participants reported a change in exercise frequency by more than one level. Mean BMI was 28.02±5.36 kg/m2 at baseline and 27.76±5.65 kg/m2 at the study end point, a decrease of 0.91%. Exercise level and BMI were not found to have any significant impact on study outcomes. Although participants were excluded if they were planning on initiating dietary or lifestyle changes during the study period, one participant notified the study staff at his week 8 (study end) visit that he had gone on vacation for several days and had consumed more alcohol than usual in the days preceding his final visit. This individual had outlying levels of hs-CRP as noted previously.
Discussion
This study aimed to assess the effect of the probiotic yeast S. boulardii on cardiovascular biomarkers, including lipids and lipoprotein particles, for the first time in human volunteers. After 8 weeks of daily supplementation, it was found that S. boulardii significantly reduced remnant lipoprotein particles, triglyceride-rich lipoproteins, which are closely related to very low-density lipoprotein. 19 Remnant lipoproteins, like LDL, are considered highly atherogenic and are positively correlated with the severity and progression of CAD, independent of LDL-C levels. 20,21 Levels of remnant lipoprotein have been shown to positively correlate with impaired endothelial function in human coronary arteries and to be significant predictors of cardiovascular events. 22,23 Because of their independent atherogenicity, remnant lipoproteins were previously identified by the National Cholesterol Education Program—Adult Treatment Panel III as a strong candidate for interventions aimed at reducing CAD risk. 3
S. boulardii may have the ability to alter cholesterol levels through a mechanism involving cholesterol assimilation. S. boulardii has been shown to remove cholesterol from laboratory culture medium by assimilation into the yeast cells. 12 Therefore, it may be possible for S. boulardii to assimilate intestinal cholesterol and subsequently alter serum cholesterol levels.
This study was designed to collect preliminary evidence on the efficacy of a specific strain of S. boulardii (Saccharomyces cerevisiae var. boulardii CNCM I-1079) as a treatment for hypercholesterolemia, but eight weeks of daily supplementation with S. boulardii was not associated with alterations in total, LDL, and HDL cholesterol. Previous studies that examined the potential hypocholesterolemic effect of other probiotics have yielded mixed results and this may be a reflection of the broad range of probiotic species and strains, dosages, and intervention lengths studied. 24,25
Participants in this study had good compliance, as measured by the end-of-study count of returned capsules. They reported very little change in exercise frequency during the study and their BMIs were consistent between baseline and the study endpoint. The results of the study demonstrate the feasibility of many of the study methods; however, limitations included not observing the dietary habits of the participants or including a control group. A follow-up study should utilize validated dietary and physical activity assessment tools and include a control group for comparison. The limited sample size in the current investigation may have reduced the ability to capture potentially significant findings; therefore, future investigations should include an a priori sample size calculation. Additionally, the study population consisted of predominantly Caucasian males with hypercholesterolemia, but who were nonsmoking, normotensive, and without diabetes or established cardiovascular disease. Expanding the recruitment criteria to include participants with additional CAD risk factors in a future study may make the results more generalizable to the population at risk for CAD because of the multifactorial nature of the disease.
Conclusions
The effect of S. boulardii on lipids and lipoprotein particles had not previously been investigated in human volunteers, and the most promising result from this investigation was the finding that S. boulardii supplementation lowered remnant lipoprotein, a predictive biomarker and potential therapeutic target in the treatment and prevention of CAD. Further investigation is needed to confirm this finding, expound upon other potential alterations in cholesterol subspecies, and explore the mechanisms involved.
Footnotes
Acknowledgments
This work has been supported by the Helfgott Research Institute at the National College of Natural Medicine and the National Institutes of Health National Center for Complementary and Alternative Medicine (5R25AT002878). We would like to thank Pure Encapsulations, Inc., and SpectraCell Laboratories for donating the probiotic capsules and their laboratory services, respectively. We also thank the study participants for their time and dedication.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.