
Abstract
Objectives:
Neurophysiologic studies of mindfulness link the health benefits of meditation to activation of the left-anterior cerebral cortex. The similarity and functional importance of intention and attentional stance in meditative and biofield therapeutic practices suggest that modulation of recipient anterior asymmetric activation may mediate the energetic effects of intention-based biofield treatments as well. The aim of the current study was to test this hypothesis by using a treatment modality known as IRECA (Istituto di Ricerca sull'Energia Cosmica Applicata).
Design:
Participants' electroencephalograms (EEG) were recorded over a 5-minute recovery period (subdivided into three 100-second intervals) while participants received genuine IRECA, placebo treatment, or no treatment, after completion of a cognitively demanding task.
Participants:
21 undergraduate students (3 men and 18 women; mean age, 22.1 years). All were right-handed and none had a history of neurologic or psychological impairment.
Outcome measures:
(1) Alpha Asymmetry Index (AAI), a standard measure of anterior asymmetric activation of the cerebral cortex, defined as the average right hemisphere minus left hemisphere log alpha power of EEG recordings for homologous pairs of electrodes in frontal and prefrontal regions; (2) self-report measures of state anxiety obtained at baseline, before treatment, and after treatment, using a short form of the State-Trait Anxiety Inventory.
Results:
In line with predictions, recipients of IRECA showed enhanced left-anterior activation of the cerebral cortex relative to placebo and no-treatment controls (as indicated by significantly higher and significantly positive AAI scores) during the first 100 seconds of treatment, and they reported greater overall reduction in state anxiety relative to baseline measures.
Conclusions:
The current study provides preliminary supporting evidence for an intention-based biofield therapeutic modality offsetting the negative effects of stress via sympathetic activation of recipients' left-anterior cerebral cortex.
Introduction
S
The association between positive/negative affect and differential activation of the left-anterior/right-anterior cerebral cortex is well documented; this association underlies the established clinical use of magnetic fields for energetically inducing differential anterior activation as a successful treatment for depression. 10,11 Left-anterior activation, as evidenced by alpha desynchronization and a corresponding decrease in EEG alpha power relative to the opposite hemisphere, is also known to increase with mindfulness meditation, 12 –16 and to be correlated with improved immune function, increased vitality, approach-oriented motivation, and general well-being; right-anterior activation, the reverse. 9,17 –19 Moreover, individuals with greater left-anterior activation recover more quickly from exposure to negative stimulation, suggesting left-anterior activation to be an effective adaptation to stress. 13 While left-anterior activation has also been reported in recipients of intention-based biofield applications, 5 lack of adequate controls render it unclear as to whether this is an effect of treatment over and above, or distinct from, that of a placebo (notwithstanding that “placebo” is a problematic construct in this area). 20 Nevertheless, left-anterior activation is consistent with other reported patterns of psychophysiologic changes in recipients of Reiki and Johrei, including decreases in heart rate and blood pressure, 21 –23 improved immune system functioning, anxiety reduction, enhanced mood, and increased vitality. 24 –27 Collectively then, these findings suggest that energetic stimulation from intention-based biofield applications may similarly offset negative affect and improve well-being via modulation of anterior hemispheric alpha activity in the brain.
The application we focus on here is IRECA. IRECA is an acronym for Istituto di Ricerca sull'Energia Cosmica Applicata (Institute for Research in Applied Cosmic Energy), founded in Italy in the 1990s by Dr. Natale Finocchiaro under the guidance of contemporary Master and Teacher of “The Way,” Alfredo Offidani, 28 with the intention of revivifying and disseminating traditional means of “energy work” in a form suitable for use in ordinary everyday life. One such method, or group of techniques, of Middle Eastern traditional origin developed and taught by members of the Institute under the aegis of the registered nonprofit organization Life Quality Project International, 29,30 has become known simply as IRECA. The method is widely practiced throughout Latin America, Mexico, and southern Europe, and aside from everyday use provides an ideal instrument for scientific investigation of the energetic effects of intention on human neurophysiology—treatment is simple, short in duration (<5 minutes), and requires only comparatively brief training to be used effectively.
Practicing IRECA involves learning to use intention and attention (“presence”) with an attitude of noninterference to facilitate energetic changes in the mind-body, typically for therapeutic and/or performance enhancement purposes. To this end, it uses the familiar operational framework of “energy centers” and “energy transmission” common to many other traditional systems, the primary function of which is instrumental, however, not explanatory (the question of the sense in which these constructs “really exist” is considered unimportant for practical purposes). Aside from this, practitioners claim the essential difference between IRECA and other biofield practices, such as Reiki or Johrei, is a qualitative one stemming from a difference of tradition, or originating intention, which can be felt or perceived experientially. Additionally, as noted, IRECA treatments are often simpler and shorter in duration than other similar techniques.
To date, studies of IRECA exist only in the form of unpublished case histories conducted by individual practitioners and collated by the Institute. Reasons for lack of scientific publication appear to be part sociocultural, part phenomenologic, in that IRECA as a practice or mode of enquiry emphasizes person-to-person communication, and understanding and verification through direct experience, over and above theory or written argument. As such, it can be difficult to translate its study into a scientific context, where the general expectation is that any research be positioned with reference to the history, discursive practices, and normative expectations of a given scientific research community, without compromising the integrity of either worldview. The current paper is an attempt to address this issue.
This preliminary study assessed neurophysiologic changes in the anterior cortex with use of IRECA to assist recovery from stress induced by completion of a cognitively demanding task. Using an experimental paradigm similar to that used by Laidlaw and colleagues in a study of Johrei, 26 the current study investigated differences in recipients' EEG results and self-reported anxiety while receiving genuine treatment, placebo treatment, or no treatment. In line with the neuropsychological literature on emotion and mindfulness meditation, it was predicted that the genuine treatment group would display enhanced left-anterior activation and report greater reduction in anxiety relative to placebo recipients and no-treatment controls.
Materials and Methods
Participants
Participants were 21 healthy, right-handed undergraduate students (mean age, 21.1 years; 3 men and 18 women), with no experience with IRECA. All participants volunteered to take part in the study via the university's research participation scheme.
Treatment
All treatments were administered by a trained IRECA practitioner with 4 years' experience of using the technique daily. Treatment followed a commonly used procedure in which the practitioner stood behind the recipient with an attitude of detached yet compassionate noninterference and a conscious intention to assist recovery, while focusing attention on one or more of the recipient's “energy centers.” In IRECA, as in techniques such as Reiki, Johrei, or qigong, this inner posture is held to facilitate a form of vital energy transfer in accordance with the needs of the individual or situation. The energy centers used in IRECA are similar to those of the yogic chakra system; although these centers are themselves nonmaterial, for operational purposes they are conceived of as “located” at specific positions on the head and spine that are associated with the regulation and expression of various aspects of psychophysiological functioning. 30
In the IRECA condition, the practitioner focused attention on each of the following centers in succession: C7, C7+C6, C7+C5, and C4 (Fig. 1). In each case the practitioner positioned one or other of his hands approximately 10–15 cm away from the relevant center while monitoring his fingertips for a change in sensation signalling completion of treatment for that center (the so-called return of energy). In the placebo condition, the practitioner enacted outward movements identical to those in the IRECA condition, but without intention to assist recovery and with attention inwardly distracted by a mental arithmetic task involving successive doubling of numbers. In the no-treatment condition, the participant was left alone in the room.

Energy centers (C2–C7) used in IRECA (Istituto di Ricerca sull'Energia Cosmica Applicata).
Participants were informed beforehand that they would be randomly allocated to one of the experimental conditions but would not be told which. Allocation to condition was made on a session-by-session basis by the practitioner in a separate room immediately before treatment via selection of a folded paper tab from a box initially containing 21 such tabs, 7 each of which were marked with 1 of the 3 experimental conditions. Participants remained with their eyes closed throughout the treatment phase, and there was no talk or physical contact between practitioner and recipient at any time. All test administration and EEG recording were conducted by a research assistant who was blind to experimental condition.
Procedure
Participants were tested individually in a quiet room, seated in a comfortable chair. Following EEG capping, they first completed a short form of the State-Trait Anxiety Inventory (STAI) state scale consisting of six items each assessed via a four-point Likert scale, 31 after which they were given an auditory N-back memory task to perform for 2–3 minutes to induce mild cognitive stress. 32 They then completed the STAI a second time, after which they were asked to close their eyes, place their hands palm-down on their upper legs, and remain calm, still, and relaxed. The research assistant then left the room and commenced EEG recording while the practitioner entered and administered “treatment” for 5 minutes. Start and finish times were logged as markers on the EEG trace using E-Prime 2.0 (Psychology Software Tools, Inc., Sharpsburg, PA) via a foot switch located in the treatment room. 33 On completion, the practitioner left the room and the research assistant re-entered to administer the third and final STAI.
EEG recording and analysis
The EEG was recorded from a 64-channel WaveGuard™ cap (ANT Neuro, Enschede, the Netherlands) using small sintered Ag/AgCl electrodes placed according to the 10–20 standard system of the American Electroencephalographic Society, with all wires shielded against outside electrical noise. An average reference was used. The signals were digitized online with a sampling frequency of 512 Hz with a 0.01–100-Hz band-pass filter. Electrode impedance was maintained below 10 kΩ (mostly under 5 kΩ). The software package ASA was used to analyze the waveforms (
Asymmetric activation
Anterior asymmetric activation was measured by means of the alpha asymmetry index (AAI), a commonly used metric in emotion and mindfulness research, calculated as the average right hemisphere minus the left hemisphere log alpha power for homologous pairs of electrodes. 13,14 Differences were calculated for electrode pairs in frontal and prefrontal regions (AF3-AF4, AF7-AF8, F1-F2, F3-F4, F5-F6, and F7-F8), then averaged across sites to increase the signal:noise ratio. 34 The AAI reflects an inverse relationship between EEG power and alpha desynchronization due to out-of-phase wave cancellation resulting from activation of independently oscillating neural units. 35 A positive value indicates left-sided activation; a negative value indicates right-sided activation.
Results
Figure 2 shows changes in anterior asymmetric activation during the treatment phase. Two-way analysis of variance on AAI scores by time and condition found a main effect of time (F[2,30]=5.563, p=0.009, ηp 2 =0.271) and a significant time by condition interaction (F[4,30]=2.755, p=0.046, ηp 2 =0.269). Post hoc comparisons with Bonferroni corrections found anterior alpha asymmetry during the early phase of treatment (T100) to be significantly more positive in the IRECA condition than in both placebo (p=0.037, d=2.112) and no-treatment (p=0.002, d=2.077) controls. There were no significant differences between groups during the mid (T200) or final (T300) phases. Additional one-sample t tests with 0 as the criterion reference (where 0=no asymmetry) showed the degree of asymmetry in the IRECA group during T100 to indicate significant left-sided activation (t[5]=3.078, p=0.028, d=1.778) and that of placebo controls during T300 to indicate significant right-sided activation (t[5]=−2.770, p=0.039, d =−1.599).
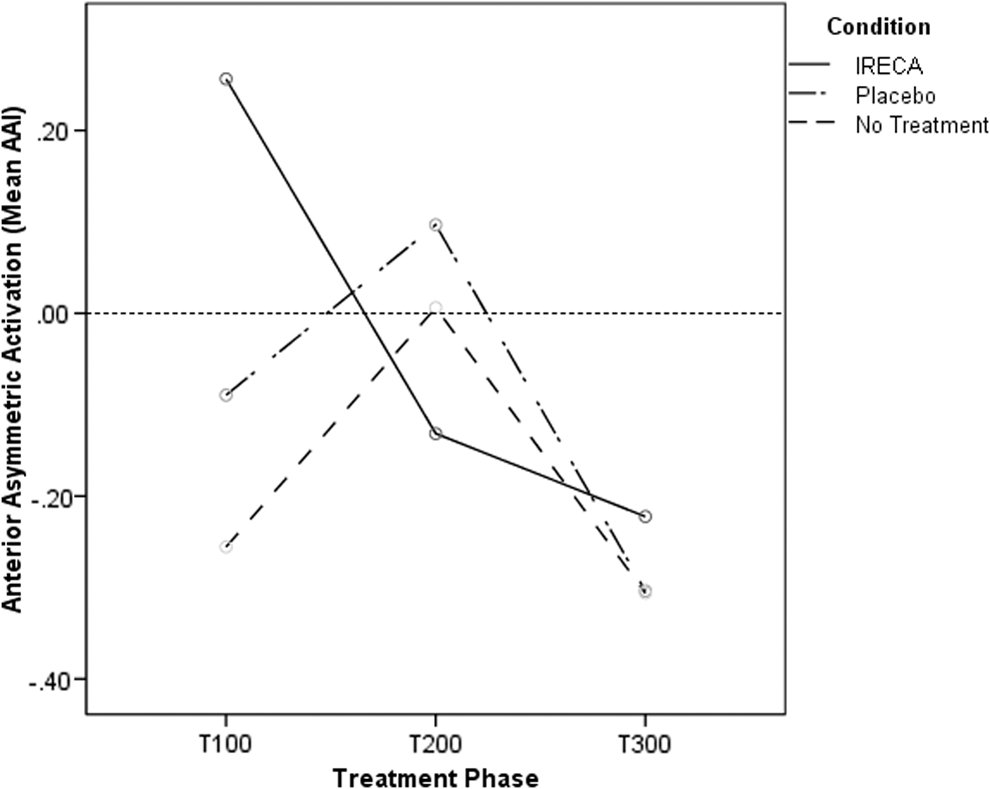
Changes in anterior asymmetric activation across time and condition.
Analysis of within-group changes in AAI scores across the treatment phase found a significant linear trend in the IRECA group (F[1,5]=16.523, p=0.010, ηp 2 =0.768) and a significant quadratic trend in the placebo group (F[1,5]=18.883, p=0.007, ηp 2 =0.791). While all three groups showed similar levels of right-sided activation at T300 (although, as noted, only in the placebo group was the degree of activation statistically significant), the IRECA group showed a gradual shift from left-sided to right-sided activation across the treatment phase, whereas the placebo group displayed a shift in the opposite direction from T100 to T200 before reverting to initial levels of right-sided activation at T300 (Fig. 2). The no-treatment group displayed a pattern similar to that of the placebo group, but the trend was not statistically significant. Accordingly, post hoc comparisons of within-group means, again with Bonferroni corrections, showed AAI scores to be significantly more positive at T100 than T300 in the IRECA group (p=0.029; d=2.002) and significantly more positive at T200 than T300 in the placebo group (p=0.022; d=1.856).
Table 1 shows self-reported anxiety levels before and after treatment. Two-way analysis of variance on STAI scores by time and condition found a main effect of time (F[2,34]=12.778, p<0.001, ηp 2 =0.429) and a marginal interaction between time and condition (F[4,34]=2.560, p=0.056, ηp 2 =0.231). Post hoc comparisons with Bonferroni corrections found significant reductions in self-reported anxiety in the IRECA group from baseline to post-treatment (p=0.012, d=1.787) and from pretreatment to post-treatment (p=0.031, d=1.667). By contrast, no reduction in self-reported anxiety occurred over time in the no-treatment group, or from baseline to post-treatment in the placebo group. Significant reduction in self-reported anxiety did occur in the placebo group from pretreatment to post-treatment (p=0.022, d=1.826), but this was only to baseline level. Although self-reported anxiety did not significantly differ between groups at baseline or pretreatment, self-reported anxiety levels in the IRECA group were significantly lower than in the placebo group after treatment (p=0.022, d=1.686).
Numbers in parentheses are standard deviations.
IRECA, Istituto di Ricerca sull'Energia Cosmica Applicata.
Discussion
In summary, in line with predictions derived from the neuropsychological literature on emotion and mindfulness, recipients of IRECA showed significantly greater left-anterior activation of the cerebral cortex during the initial phase of treatment compared with placebo and no-treatment controls; moreover, the degree of left-anterior activation was itself statistically significant. Asymmetric activation per se tended to diminish in all three groups during the midphase of treatment and to increase again in the right anterior hemisphere during the final phase. Recipients of IRECA reported greater overall reduction in anxiety relative to baseline measures than did placebo and no-treatment controls.
It is significant that left-anterior activation during the first 100 seconds of treatment not only coincided with the period immediately following stress induction, but with the practitioner's treatment of centers C7 and C6, located on the top of the head and forehead, respectively (Fig. 1), both of which are associated with cerebral functioning. This suggests the possibility of some form of local energetic stimulation of the frontal cortex analogous to that produced by magnetic fields in treatments for depression. 10 However, whereas magnetic fields are applied to one or other side of the head (depending on whether activation is being induced or inhibited), in IRECA the practitioner's hands are positioned—and attention is focused—on central positions lying on the midline between the two hemispheres. It is thus unclear why local stimulation of the cerebral cortex via the practitioner's hands should affect one hemisphere differently than the other. Arguably, the effect is more likely to be nonlocal, or intentional, as practitioners themselves maintain.
The tendency for right-anterior activation to diminish in control groups during the midphase of treatment is likely due to natural decay of the effects of the stressor task (which were mild). If so, however, this raises the question of why a reverse tendency should be seen in all three groups during the final phase, and why in the case of the IRECA group in particular did continuing treatment not offset this tendency as it did during the initial phase? The latter also suggests that lower post-treatment self-reported anxiety in the IRECA group may in effect constitute a retrospective evaluation of treatment per se rather than a measure of current affective state. One possibility is that the tendency toward right-sided activation during the final phase reflects emotional fatigue caused by ongoing exposure to laboratory conditions, and that the lack of treatment effect indicates a mismatch between the nature of the problem and the specific “energy centers” treated. Unlike the initial phase where, as noted, treatment of C7 and C6 was functionally concordant with the nature of the stress involved, itself primarily cognitive, in the final phase treatment may not have been optimal if emotional fatigue were the underlying issue. From the operational perspective of IRECA, treatment of C3 and C2 would be thought more appropriate in this context, but this was not included in the experimental protocol. If correct, this interpretation underscores a basic principle of IRECA and other traditional systems that energy centers are functionally (and/or intentionally) related to distinct aspects of psychophysiologic behavior, while suggesting that anterior asymmetric activation may provide a useful generic indicator of treatment action and efficacy. Future research could address this possibility through exploring the comparative effects on anterior asymmetric activation of treating each specific center under a range of different stressor conditions.
If a functional relationship does exist between specific energy centers, psychophysiologic processes and treatment efficacy, this raises the question of the ontologic nature of that relationship. As noted, while for practical purposes the energy centers used in IRECA are conceived of as anatomic locations, they are not in themselves understood as occupying space in the normal physical sense; rather, they are “imaginal” objects (as distinct from “imaginary”), 36 not material. As such, their mode of influence is nonlocal and noncausal, operating in the experiential dimension of intention and presence, and not via physical energy transmission through or across space as is often described and/or assumed. 3,37 While the latter provides a convenient working metaphor in therapeutic contexts (including IRECA), if taken literally it is misleading for scientific purposes. 38
Interestingly, recent attempts by neurophysiologists at theorizing the link between mindfulness (or presence) and anterior asymmetric activation have also foregrounded the role of intention in neurophysiologic activity. Schwartz and colleagues have argued from a quantum-theoretical perspective that intention on a specific goal initiates a process of neural self-organization in which conscious attention facilitates collapse of the global quantum superpositional brain state in such a way that resultant patterns of neural activity tend to actualize the intended outcome. 39 According to Schwartz and colleagues, intention controls attention density, which itself increases the probability of one brain state occurring rather than another, thus overriding and reorganizing habitual patterns of neural response. Similarly, Freeman, in discussing the salience of Aquinas' concept of intention as “action into the world” for understanding nonlinear brain dynamics, emphasizes the influence of intention on the ongoing production, selection, and actualization of potential patterns of sensorimotor neural activity in accordance with changes in an organism's environment or context. 40 Both approaches argue for the unity of mind, brain and body, and accord intention a primary, nonreducible, nonlocal potentiating role in neurophysiologic activity.
While such models lend themselves well to accounting for neurophysiologic effects of intention at an individual level, if intention acts nonlocally, as Schwartz and colleagues suggest, there is no reason in principle why these effects should occur only within biologically defined individuals. Arguably, the theory also allows for the way one person directs intention to affect, or potentiate, the mind-brain-body state of another, as is claimed by practitioners of intention-based treatment modalities and for which the present study offers preliminary supporting evidence. Moreover, such effects, if they exist, should in theory be independent of physical proximity. Equally, it is important to acknowledge that the meaning of the term intention originally also encompassed the inherent tendency of the body toward health as its natural or optimal energetic state of well-being—a state we know in part to be associated with left-anterior activation of the cerebral cortex—and that, as Weiner and Greene have recently argued, intention-based treatment modalities may facilitate, or energetically assist, the operation of this unconscious tendency in the recipient through its sympathetic alignment, or entanglement, with the conscious intention of the practitioner. 41 As such, this may in part account for why, as in mindfulness meditation, an attitude of detached noninterference or nonego involvement on the part of the practitioner is held to be an important determinant of treatment efficacy.
Because the present study was preliminary in nature, it necessarily focused on immediate proximal effects of treatment rather than its potential long-term benefits. However, studies of experienced meditators have found evidence for permanent changes in anterior activation associated with regular mindfulness practice over prolonged periods of time; an example of the more general phenomenon known as self-directed neuroplasticity. 39 As IRECA and other intention-based biofield modalities are typically used not only for remedial purposes but on a daily basis for general maintenance of health and well-being, it seems reasonable to assume that similar long-term changes in brain activity may also occur with regular use of these practices as well. Future longitudinal studies could address this possibility.
While the present study was methodologically sound in terms of blinding procedures, randomisation and controls, future studies may benefit from the following modifications. Firstly, in order to better maximise sensitivity to treatment-related changes in EEG, and in accordance with known individual differences in dominant EEG frequencies, data collection and analyses might more usefully employ individually-defined alpha frequency ranges rather than a conventionally-defined bandwidth. 35,42 Secondly, while clear and predicted differences in neurophysiologic response were still observed in the genuine treatment group relative to placebo and no-treatment controls immediately after task, and similarly in post-treatment self-report measures of anxiety relative to baseline, the fact that the N-back task used in the present study for elevating levels of pretreatment anxiety produced only minor and/or inconsistent effects suggests future studies using this task as a stressor should make the value of N contingent on prior performance to maximize its effect on a given individual. Future studies might also include additional physiologic measures of stress response, such as skin conductance or heart rate variability, allowing analysis of covariation of such measures with asymmetric activation and thereby circumventing the issue of confounding self-report measures of affective state with retrospective treatment evaluation as noted above. Finally, the issue of local versus nonlocal action could be usefully addressed via addition of a proximal-remote treatment condition, while also recording EEG from practitioner and recipient simultaneously. 43
Conclusions
The current study provides preliminary supporting evidence for an intention-based biofield therapeutic modality offsetting the negative effects of stress via sympathetic activation of recipients' left-anterior cerebral cortex.
Footnotes
Acknowledgments
The authors would like to thank Simon Kriss-Rettenbeck for invaluable help and advice on IRECA and Adela Neagu for assistance in collecting data.
Author Disclosure Statement
No competing financial interests exist.