
Abstract
Objective:
This study investigated the advantage of photoluminescent bioceramic (PLB) irradiation on meridian channels of abnormal meridian currents, as well as the normalization of meridian current levels that may represent the participants' physiologic conditions.
Design:
Statistical analysis of survey data.
Participants:
Forty-six patients with abnormal meridian current in the gallbladder (GB).
Interventions:
The effects on the meridian currents were measured by an electrodermal instrument after PLB irradiation was applied to the GB and other specific acupuncture points. Each meridian was categorized into six physiologic levels to evaluate effectiveness after the PLB irradiation: 1, extremely low; 2, moderately low; 3, normally low; 4, normally high; 5, moderately high; and 6, extremely high level. The positive effect of PLB treatment for each meridian could be defined as the normalized ability of the meridian level from the extreme values (1, 2, 5, or 6) approaching the normal levels (3 or 4).
Results:
Participants with higher average meridian current (Amc >36 μA) calculated from the currents of 24 Ryodoraku points could be significantly normalized after the PLB treatment (p=0.0241). A significant positive effect was seen in comparison with the negative effect of PLB on the GB meridian (McNemar test, p=0.00004) (n=46×2 for left and right GB meridians). A patient with benign facial tremor was treated by PLB for 1 month; PLB improved the facial tremor and normalized effects on Amc and meridian current levels at the GB, lung, small intestine, bladder, and kidney.
Conclusion:
A method was proposed to evaluate the normalization effect of a noninvasive PLB technique on the 12 meridians. PLB acupuncture on the specific meridian points could show the normalization ability of Amc and GB meridian for the participants.
Introduction
A
The scientific basis for acupuncture meridians is not clear. Past studies have suggested that acupuncture meridians are physiologically characterized by low electrical impedance and anatomically associated with connective tissue planes. 3 Researchers reported that acupuncture points correspond to the high electrical conductance and low skin resistance points on the body surface along the meridians. Stimulation of the sympathetic pathways will result in a lower skin resistance level because skin electrical resistance depends on the activity of the sympathetic nervous system. 3 –7
In a previous study, Zhang et al. 8 used a hydromechanic model in the basic state of low hydraulic resistance and tested it in two in vivo models: humans and miniature pigs. The study showed lower hydraulic resistance on meridians compared with non-meridian areas. These researchers also measured transmission of artificial interstitial fluid pressure waves by using a single pressure transducer; 8 the points form channels along the meridians, referred to as low-hydraulic-resistance channels. This means that low-hydraulic-resistance points were found very close to low-impedance points along meridians.
These previous studies used a gamma camera to successfully detect the meridian channel traced by migration of isotope saline. 8 Sheu et al. proposed an electro-osmotic flow model and deduced the relationship of the arteriole, venule, and lymphatics surrounding a path of interstitial fluid, which was suggested as the meridian path. 5
In the current authors' previous studies, electrodermal measurements on various points were used, which are believed to represent different meridian energy. 1,9 Some points with abnormal current conductivity were selected to undergo photoluminescent bioceramic (PLB) treatment. PLB treatment weakens hydrogen bonds and alters the characteristics of water. 10 PLB irradiation of specific acupuncture points demonstrated a reliable complementary effect on the abnormally low or high current levels of meridian measurement, which will return or approach to the normal current levels. These previous data also showed the interactions between the current flows of relative meridians. Because PLB treatment induces fluid/water diffusion, it supports the idea that meridian lines are interstitial microscopic fluid channels. 9,10
Electrodermal measurements have been infrequently evaluated in prospective clinical trials that monitor electrodermal measures over time to assess their correlation with disease course. 2 The method proposed in the current study evaluates the advantage of using noninvasive PLB irradiation on specific meridian channels of abnormal upper and lower extremities and monitoring electrodermal measurements of 24 Ryodoraku meridian points. This study further investigates the possible communication of different meridian channels and the normalization of meridian current levels that may represent the participants' physiologic conditions.
Materials and Methods
Participants
The participants were adults who consented to participate in this trial, sponsored by Taipei Medical University and Fu Jen Catholic University, from January to November 2013. Forty-six patients were involved in this study (18 men and 28 women). The mean age was 51.5 years (range, 26–68 years). All patients had an abnormal meridian current in the gallbladder (GB). The human subjects committee at the hospital approved the study (approval number: TMU-JIRB201207024).
Measurements of meridian current on different candidates
The meridian current was measured (unit of measure, μA) by using a MEAD Me-Pro, 6th generation (Hanja International CO. Ltd, Taoyuan, Taiwan), device, which yielded electrodermal measurements of the 24 Ryodoraku meridian points—lung (LU9), pericardium (PC7), heart (HT7), small intestine (SI4), triple energizer (SJ4), large intestine (LI5), spleen (SP3), liver (LR3), kidney (KI4), bladder (BL65), GB (GB40), and stomach (ST42)—and was similar to the equipment used in the authors' previous studies. 9 The average value of the meridians current (Amc) was calculated on the basis of the measurements of the 24 Ryodoraku meridian points. The machine is composed of two electrodes: the first is a metal cylinder held in the patient's left hand, and the second is connected to a spring-loaded probe containing cotton moistened with physiologic saline solution. A trained technician applies the second electrode to the 24 acupuncture points along the 12 meridians (12 on the left side and 12 on the right side). This device is advantageous because the overall current levels provide good reproducibility when the device is operated by a trained technician. 9 To reduce bias, all measurements were performed between 07.00 and 09.00 pm.
PLB treatment
Ceramic powder was obtained from the radiology laboratory of Taipei Medical University (Taipei, Taiwan). The bioceramic material consisted of micro-sized particles produced from various elemental components. 9 –25 Seven percent bioceramic material was embedded in a silicon sticker with good translucence (YY Rubber Co., Foshan, Guangdong, People's Republic of China). Photoluminescence of the bioceramic material emits specific wavelength spectra, including near, middle, and far infrared. 9 –25 It was provided by using visible light source irradiation, which was directed to the silicon sticker placed on the selected meridian lines at the corresponding acupuncture point (Fig. 1A). The light sources were visible light-emitting diodes, which emitted wavelengths of a visible white light spectrum between 480 and 780 nm. The level of illumination was strictly controlled at 450±50 lux (mean±standard deviation), avoiding thermal effects on the participants' skin.
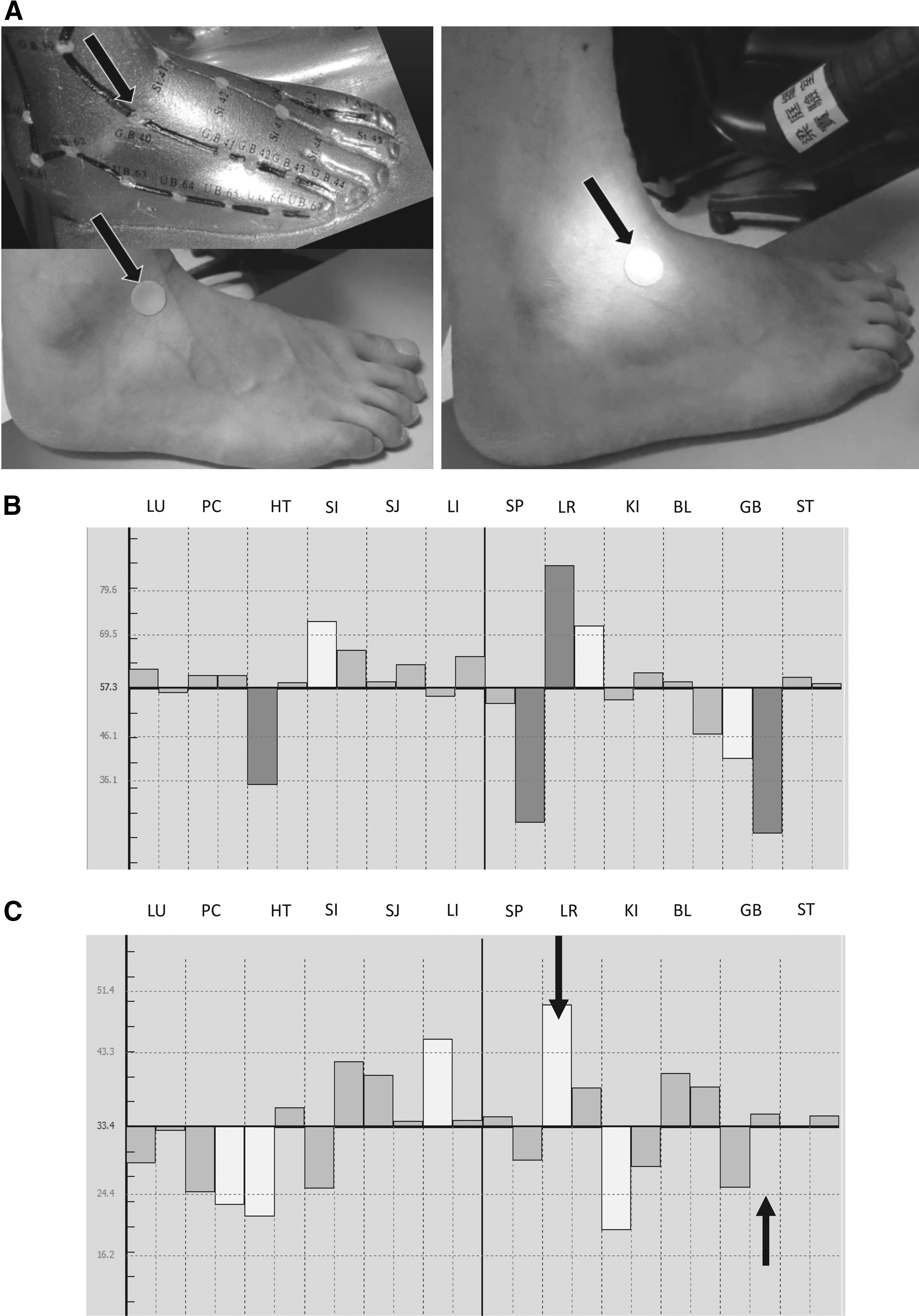
Photoluminescence of the Bioceramic material (PLB) treatment and meridian current measurement.
After the corresponding acupuncture points were selected for each participant, PLB irradiation was performed for 30 minutes. In this study, 46 participants had been treated at the GB meridian to normalize their abnormal meridian current; 1 of these had benign facial tremor. After a review of a Chinese acupuncture textbook, 26 the following points were selected from GB 37 and 40 for all of participants. According to the abnormal meridian current measured from the Ryodoraku meridian points and the individual symptom, additional points could be selected: PC6; HT6, 7; SI3, 4; SP3, 4; LR3, 4; KI4, 7; BL60, 65; ST42, 43. A case of benign facial tremor was treated by PLB for 1 month.
Category of the meridians current level before and after PLB treatment
According to the Amc and standard deviation (SD) calculated from the meridian currents measured from the 24 Ryodoraku acupoints, the two upper lines (U1 and U2 of Amc+1 and 0.5 SD, respectively) and two lower lines (L1 and L2 of Amc−1 and 0.5 SD, respectively) of current deviation from Amc were determined by the MEAD device, as shown in Figure 1B and C. The participants with meridian current findings could be divided into six categories, with the numbers representing their meridian physiologic conditions: extremely high current level (level 6) of meridian current (mc)>U1, moderately high current level (level 5) of U2<mc<U1, normally high current level (level 4) of Amc<mc<U2, normally low current level (level 3) of L2<mc<Amc, moderately low current level (level 2) of L1<mc<L2, and extremely low current level (level 1) of mc<L1. Therefore, the abnormal current levels (1, 2, 5, or 6) will be defined as the meridian current that is above the two upper lines (U1 and U2) or below the two lower lines (L1 and L2) of current deviation from the participant's Amc.
Definition of effects on 12 meridians after PLB treatment
After PLB treatment on the GB meridian, it was noted that the current level of other meridian channels could be influenced. The effectiveness of different meridians was quantified according to the following rules: (1) positive 1 effect (+1): if the level of meridian current changed from extreme levels 6, 5, 2, or 1 to the normal levels 3 or 4; (2) positive half effect (+0.5): if the level of meridian current changed from level 6 to 5 or level 1 to 2; (3) positive one-quarter effect (+0.25): if the extreme levels of meridian current reversed (e.g., levels 6 or 5 to levels 2 or 1, or vice versa); (4) null effect (0): if the level of meridian current unchanged or remained in the normal levels (3 to 4, or 4 to 3); (5) negative half effect (−0.5): if the level of meridian current changed from level 5 to 6, or level 2 to 1; (6) negative 1 effect (−1): if the level of meridian current changed from normal levels (levels 3 or 4) to the extreme levels (levels 6, 5, 2, or 1). Therefore, the summarized effectiveness score of 12 meridians could be obtained for each participant after the PLB treatment. For simplicity, the influence is defined as positive (including +1, +0.5, and +0.25), null (0), or negative (including −0.5 and −1) “crossover” effect by PLB treatment.
This study proposes a method to calculate and compare before and after PLB irradiations for the effects on Amc, physiologic levels of each meridian, and the normalizing ability on different meridian channels.
Data analysis
Statistical analyses were performed using SPSS software, version 15.0 (SPSS Inc., Chicago, IL). Individual variables were evaluated by using percentages, means and SDs, and group differences were assessed by using a paired t test. The McNemar test (a chi-square test for within-subjects designs) is also used to examine the favorability of positive or negative effect on each meridian's currents after PLB treatment.
Results
Ability of PLB treatment to normalize Amc
The participants with a high average Amc value calculated from the 24 Ryodoraku meridian points could indicate a significant decreasing effect after PLB irradiation treatment. Table 1 shows a mild decrease (p=0.0592) in Amc for all participants (n=46) after PLB treatment, but a significant decrease (p=0.0241) in Amc for participants (n=23) with original Amc >36 μA before the PLB treatment. The selection of Amc >36 μA was determined from the mean Amc from all 46 participants before PLB treatment, as shown in Table 1. Meanwhile, the participants (n=23) with original Amc <36 μA showed a nonsignificant effect on their Amc value (p=0.89) after PLB treatment. Figure 2 shows the clinical measurement of Amc before PLB treatment and the Amc difference after PLB treatment of two groups of participants (PLB pretreated Amc <36 and >36 μA).

Change in average meridian current (Amc) during PLB treatment.
Statistical analysis using paired t test.
p-Value<0.05.
Amc, average median current; PLB, photoluminescent bioceramic; SD, standard deviation.
Ability of PLB treatment to normalize meridians
To study the effects of PLB treatment on different meridians, 46 participants with an abnormal GB meridian were selected to calculate the normalizing ability of PLB treatment on all 12 meridians. Figure 3 shows that after PLB treatment, the current level of each meridian channel could be influenced. This finding confirms the expectation that the highest percentage (47.8%) of participants' meridians on both the left and right sides shows a positive effect (including +1, +0.5, and +0.25) on the abnormal GB meridian, and that a small percentage (14.1%) shows a negative effect (including −1 and −0.5). The McNemar test (Table 2) showed a significant positive effect on GB meridian compared with the negative effect (p=0.00004) (n=46×2). If the overall effect on the 12 meridians for all participants after PLB treatment are considered (n=46×2×12), the McNemar test (Table 2) shows a significant positive overall percentage of cross-over effects compared with the overall percentage of negative effects (p=0.033).
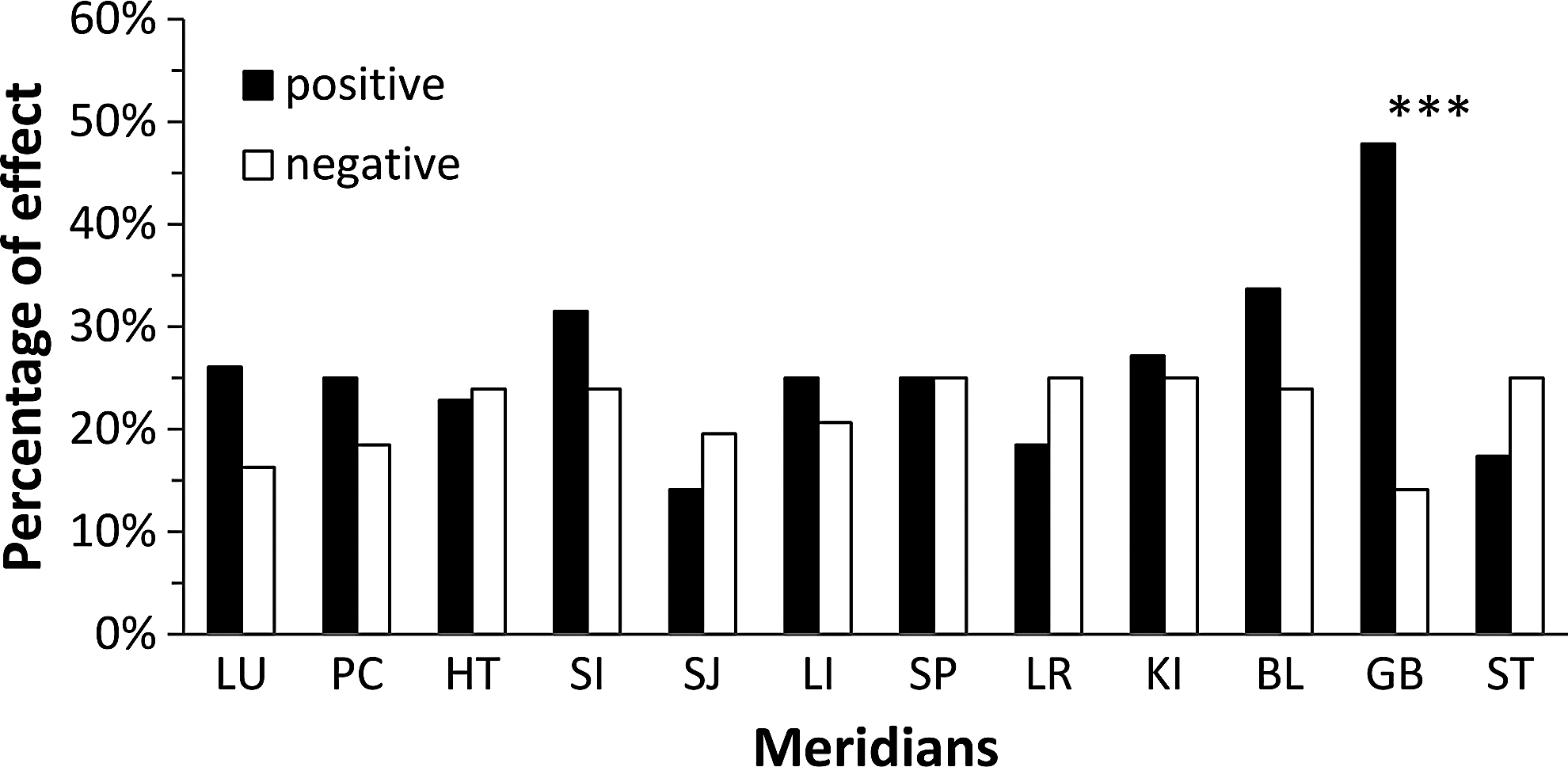
Percentage of positive and negative effects for each meridian after PLB treatment. (n=46×2). ***Significant difference between positive and negative effectiveness score after PLB treatment (p<0.001).
Favorability of positive or negative effect examined by the McNemar test on the crossover effectiveness score of 12 meridians from participants (n=46×2) after PLB treatment.
p<0.05 (significant positive effect compared with negative effect).
The overall significant positive effectiveness score may due to the higher positive crossover effect on meridians, such as GB, LU, PC, SI, LI, KI, and BL, as shown in Figure 3. The moderately negative effect may due to the insufficient effects of present PLB treatment on other meridians (e.g., HT, SJ, SP, LR, and ST meridians), as shown in Figure 3. However, Table 2 demonstrates that the McNemar test showed no significant difference (with p>0.05) in the percentages between the positive and negative effects by the present PLB treatment on meridians except for the GB meridian. This technique needs to be improved, thereby allowing evaluation of the normalizing effect of any meridian by a more efficient PLB treatment on the combination of synergic acupoints or the sufficient irradiation time on different acupoints.
In calculating the summarized effect (sum of effectiveness scores from +1 to −1) of the 12 meridians after PLB treatment for each participant, 57.4% of participants (n=46) had a positive summarized effectiveness score, and 36.2% of participants had a negative summarized score. Therefore, the summarized scores for each participant from their 12 meridians might be an index for evaluating the efficiency of PLB treatment. This study further investigated the changes of 12 meridian currents, Amc, and summarized effectiveness scores for a clinical case of benign facial tremor during 1 month of PLB treatment, as described in the following section.
Normalizing ability of PLB treatment for a case of benign facial tremor
This patient had an unusual benign facial tremor before the PLB treatment. Figure 4A shows the significant decrease from an extremely high Amc (original Amc, 53.6 μA) to a moderate low value (19.5 μA) after the first PLB treatment. The low Amc lasted for 1 week (day 7) until the second PLB treatment, which resulted in a slight increase in Amc (23.5 μA). This increase lasted for another week (day 14) until the third PLB treatment; the Amc then decreased slightly (18.4 μA). During the first 2 weeks of treatment, the patient's benign facial tremor improved, and the summarized effectiveness score of the 12 meridians (Fig. 4B) showed a significantly high positive score (+8.5) after the first PLB treatment. The score was subsequently maintained around the null value for the first 2 weeks. From day 14 to day 24, the patient showed an unexpected tendency of increasing Amc; during this time, the summarized effectiveness score of the 12 meridians gradually decreased to a negative value of −9.25. The PLB treatment was then shortened from 7 days to 3 days, and the patient again showed a normalized Amc (Fig. 4A) as well as a summarized effectiveness score that approached the null after day 27 (Fig. 4B). Because the improvement of facial tremor lasted and sleep difficulty and anxiety were relieved during the treatment period, the patient stopped the PLB treatment after 1 month.
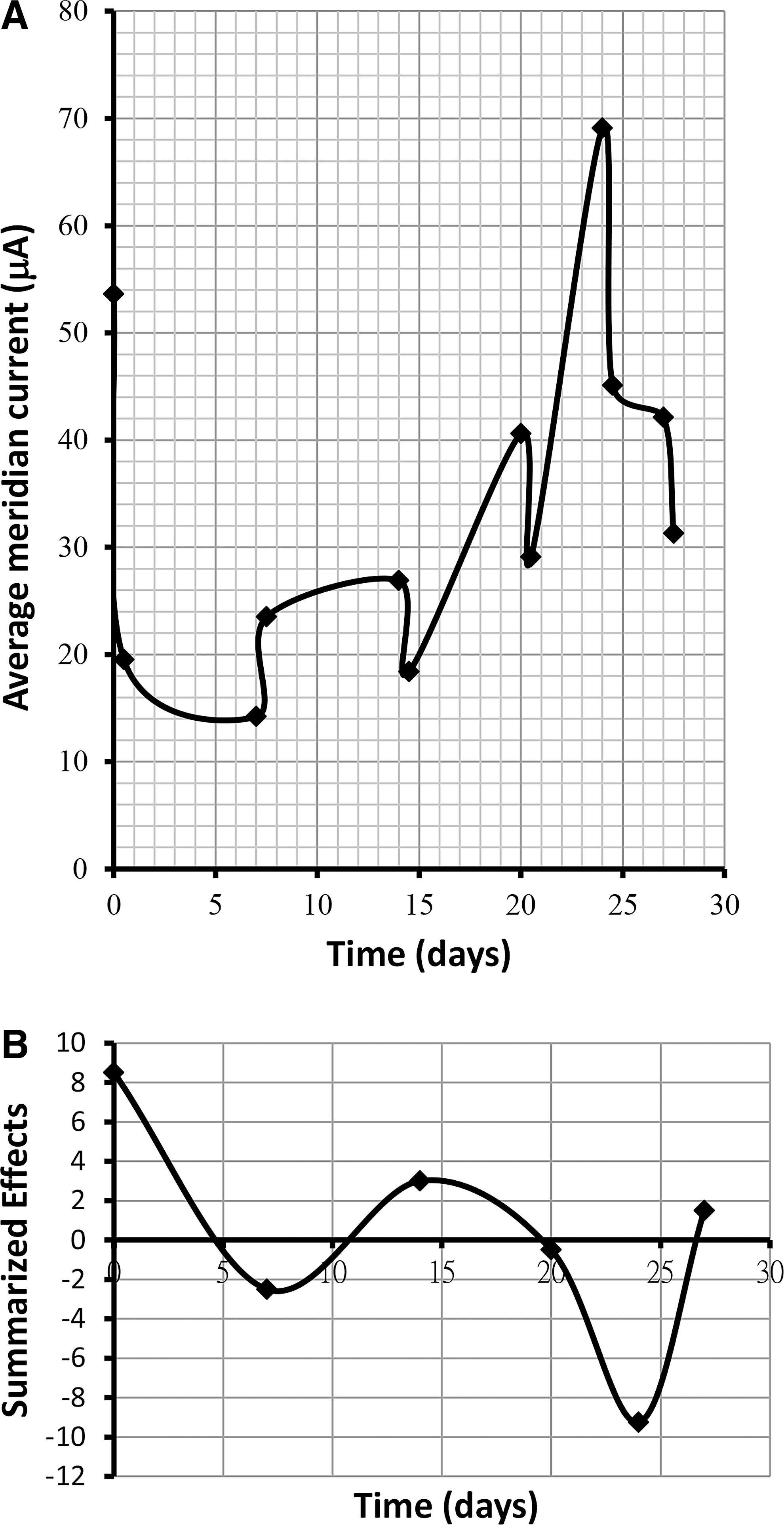
Changes in Amc
Figure 5 shows the variation in physiologic levels in each meridian on both the left and right sides for the patient with benign facial tremor during the 1-month PLB treatment. The mean physiologic levels during this 1-month period were calculated. The following mean current levels were normal: GB, 3.5±1.06; LU, 3.46±0.78; SI, 3.21±1.22; BL, 3.63±1.17; and KI, 3.04±1.12. However, moderately abnormal mean levels were seen for LI (2.08±0.97), ST (4.64±1.01), SP (1.83±0.82), HT (4.21±1.98), and PC (4.64±1.01), SJ (2.33±0.96). Extremely high meridian levels were seen for LR (5.46±0.78). Therefore, although facial tremor improved in this patient, the simple PLB treatment in this study is not sufficient to compensate for all of the abnormal meridian levels. Other combinations of synergic acupoints or even medical treatment on meridians will be considered in the future.
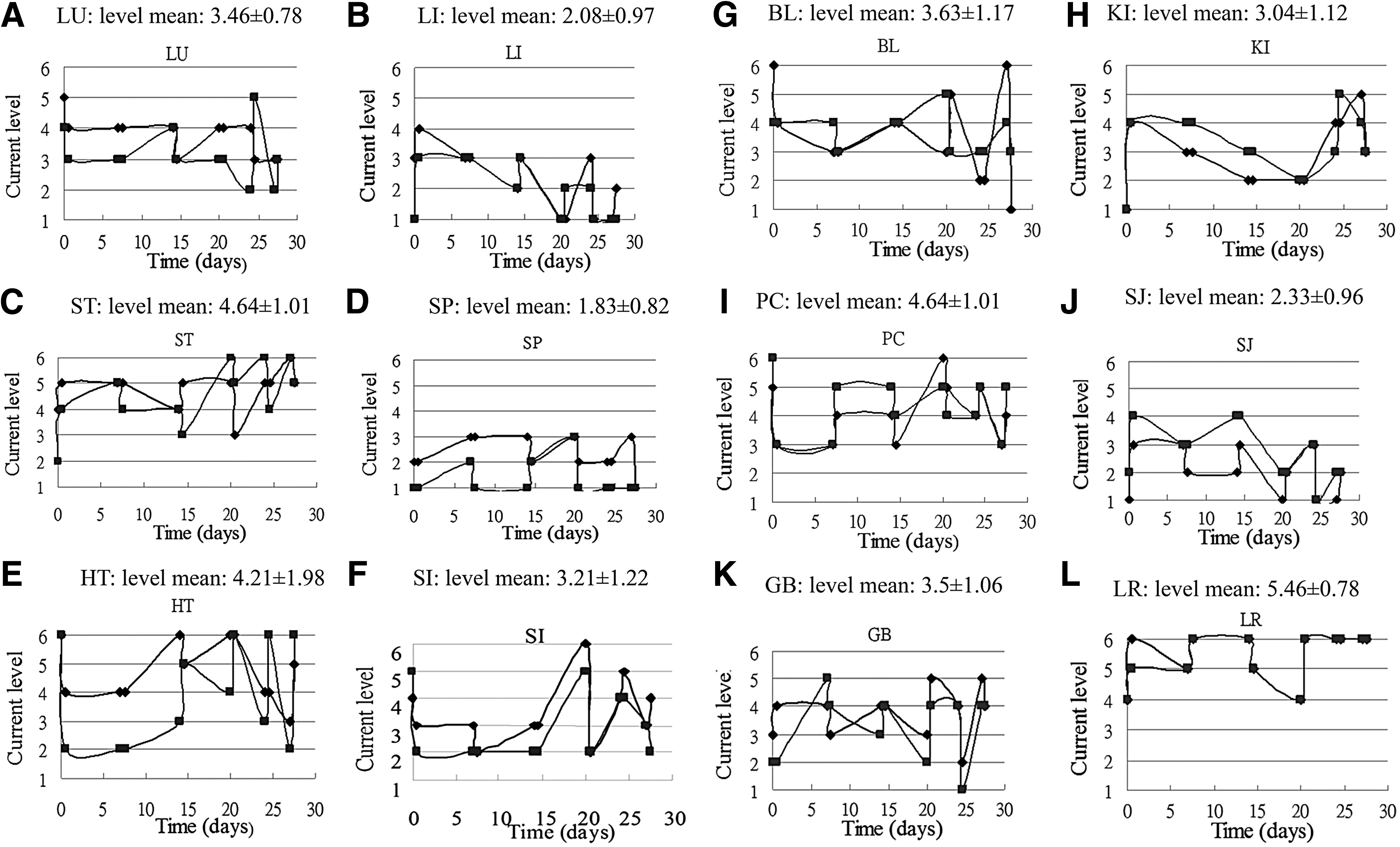
Change in current level in 12 meridian of left and right sides during PLB treatment.
Discussion
Table 1 and Figure 2 propose a method to study clinical cases with higher Amc. The normalizing effect of an abnormal high Amc was obvious for participants after the PLB treatment; however, as a result of the few cases of extremely low Amc in the present study there are still insufficient clinical cases with which to study the normalizing ability of extremely low Amc by the present acupoint treatment of PLB irradiation. Huang et al. reported that participants with abnormal stomach and esophageal findings according to gastroscopy had significantly lower mean meridian energy. 1 The current study could be expanded in the future to include the possible normalizing procedure in elderly patients and those with cancer or chronic illness, who may show extremely low Amc.
Figure 3 shows the possible tendency of balance effects on LU, PC, SI, LI, KI, BL, and GB meridians and the probable non-normalized effects on HT, SJ, SP, LR, and ST meridians in the present study. However, from a statistical analysis using the McNemar test, no significant positive effect could be seen on any meridian except for the GB meridian. Figure 5 demonstrates that the case of benign facial tremor occurring during 1 month of PLB treatment resulted in normal mean current levels at LU, SI, BL, KI, and GB but moderately abnormal levels at LI, ST, SP, HT, PC, SJ, and LR. Therefore, there is some consistency (e.g., LU, SI, BL, KI, and GB) in positive effects between the participants with abnormal GB meridian and the patient with a benign facial tremor after PLB treatment. In the meantime, the normalized tendency of Amc, as shown in Figure 4A, is also consistent with the ability of PLB treatment to normalize values among the participants with higher baseline Amc (Fig. 2B). Further study to improve the current PLB treatment is needed. Some traditional Chinese acupuncture practices may help in finding a better combination of acupoint irradiation by PLB. Some researchers might also study normalized balance between meridian currents of the left and right sides or of yin and yang. 1,2
In the future, to explain the preceding findings, the basic physiologic concepts about current conductivity of the skin should be reviewed. Skin conductance depends on current flow through skin due to an electro-osmotic effect. 27 A report of skin electrical impedance by use of hairless mouse skins showed a decrease in skin electrical resistance with increasing the ionic strength of the bathing medium. With increasing temperature, resistance of electricity of skin also decreased. 28 Ahn et al. proposed that collagenous bands, represented by increased ultrasound echogenicity, are significantly associated with lower electrical impedance and may account for reduced impedance at acupuncture meridians. 3 Schimdt et al. reported that the measurement of electroconductivity of Ryodoraku meridian points is a useful technique for evaluating sympathetic nervous activity, which could help to estimate the milder surgical trauma of needlescopic cholecystectomy (showing a lower Amc after 30 minutes from the start of surgery) than laparoscopic cholecystectomy. 29 Ryodoraku method is widespread in Japan, where electroconductivity in dermatomes corresponding to the level of sickness is used to stimulate the acupoint or suppress it. 29
In recent years, more clinical cases have shown the efficiency of acupuncture medicine. Descriptive statistics showed greater improvement of shoulder mobility for the verum group versus the control group immediately after treatment and after 3 months; the trial indicates that Chinese acupuncture is an effective alternative to conventional orthopedic treatment for chronic shoulder pain. 30 These data presented an opportunity to effectively and quantitatively evaluate the clinical utility of electrodermal measures for pelvic pain. 30 Many successful clinical practices of electrodermal measurement combined with acupuncture medicine highlight future developments based on the findings from the present study. Meanwhile, because of the simplicity and noninvasive characteristics of PLB treatment, the clinical case could be self-cured by PLB procedures applied to specific acupoints at home, with frequent re-examination of meridian conditions at a medical institution.
In conclusion, this study showed that PLB treatment could significantly normalize the high Amc (>36 μA) of clinical cases to a lower value. The proposed method can be used to evaluate the effectiveness score of each meridian, calculated from the change in physiologic levels after the PLB treatment. Compared with a negative effect, we observed a significant positive effect on GB meridian current after PLB treatment. A patient with benign facial tremor was treated by PLB for 1 month period; PLB resulted in alleviation of the symptoms of facial tremor and normalized effects on Amc; summarized cross-over effectiveness score of the 12 meridians; and meridian levels at GB, LU, SI, BL, and KI.
Footnotes
Acknowledgments
The authors are grateful to Mr. Tai-lin Ping (Health Control Consulting Co. Ltd.) for providing technical support.
Author Disclosure Statement
No competing financial interests exist.