
Abstract
Purpose:
Acupuncture has been used as a complementary medical treatment for arthralgia and other types of pain. The objective of this review is to assess the effectiveness of acupuncture in the treatment of arthralgia in patients with breast cancer who were treated with aromatase inhibitors (AIs).
Methods:
A literature search was performed, without language restrictions, of 10 databases from their inception through February 2014. The literature reviewed included randomized clinical trials (RCTs) and clinical trials that compared real versus sham acupuncture for the treatment of AI-related musculoskeletal symptoms (AIMSS). The methodologic quality of these trials was assessed by using the modified Jadad Quality Scale. Meta-analytic software (RevMan 5.0) was used to analyze the data.
Results:
Five To compare the effects of real versus sham acupuncture, five RCTs were assessed by meta-analysis and quality analysis. Three of the RCTs reported favorable effects with regard to use of acupuncture in reducing pain and joint-related symptoms, while the other two RCTs did not. The meta-analysis showed trends toward reduced pain and stiffness in patients given acupuncture compared with those who received sham treatment (n=82; pain, mean difference: −2.07 [95% confidence interval (CI), −4.72 to 0.57]; p=0.12; stiffness, mean difference: −86.10 [95% CI, −249.11 to 76.92]; p=0.30), although these differences were not statistically significant.
Conclusions:
Acupuncture has been reported as a safe and promising treatment for AIMSS, but the present analysis indicated that the effects were not statistically significant. Other outcome measurements, such as imaging studies, would be worth including in future studies to further confirm the efficacy of acupuncture in AIMSS.
Introduction
W
In general, AIs are well-tolerated drugs with minimal adverse effects. The common adverse effects include hot flashes, vaginal dryness, and headache, which are typically mild. However, AIs significantly increase musculoskeletal symptoms, such as osteopenia, osteoporosis, and fracture rate, when compared with tamoxifen (375 vs. 234 cases; incidence rate ratio, 1.55; p<0.0001). 9 Studies showed that 28%–47% of patients who receive AI therapy experience musculoskeletal disorders 10,11 and 5%–25% of patients discontinue therapy because of these or other adverse effects. 11,12 More than half of patients with such adverse effects take oral medications (nonsteroidal anti-inflammatory drugs; acetaminophen; opioids; or oral supplements, such as glucosamine, chondroitin, and omega fish oils) for pain relief or use nonpharmacologic interventions, mainly exercise, to relieve joint symptoms. 11 However, the efficacy of these approaches is limited. Effective treatment of AI-associated musculoskeletal symptoms (AIMSS) will enable patients to complete their full recommended course of adjuvant endocrine therapy. 13
The etiology of AIMSS is not well understood; hypotheses include estrogen deprivation; neurohormonal changes causing changes in pain sensitivity; and changes in circulating proinflammatory cytokines, such as interleukin (IL)-1, IL-6, and tumor necrosis factor (TNF)-α. 14 Acupuncture has been used for treating oncology-related issues, with an increasing number of physicians focusing on this form of therapy in the treatment of AIMSS, 15 although no mechanistic explanation has been provided. Since 2007, many clinical trials have addressed this topic, but the results of these trials have not yet been synthesized into a systematic review. In most of the studies on this topic, acupuncture profiles were generally designed as true acupuncture versus sham acupuncture for 6–12 weeks, with specific and local acupoints. The investigators then compared primary outcomes: joint pain, stiffness, and self-reported pain or functional score based on validated tools. Several of the studies also measured changes in serum cytokine, such as IL-1β and TNF-α, which were considered secondary outcomes. 16,17
To improve understanding of the efficacy of acupuncture in AIMSS, the objective of this systematic review was to summarize and critically assess the evidence from all available randomized clinical trials (RCTs) that examined acupuncture in the treatment of AIMSS in patients with breast cancer.
Methods
Data sources and eligibility criteria
The conduct of this systematic review complied with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement to ensure transparent and complete reporting. 18,19 The following 10 databases were searched for relevant RCTs, with no language restrictions, from their inception dates to February 2014: MEDLINE (Ovid), PubMed (Publisher-Supplied Subset, supplementary to Ovid MEDLINE not yet covered), EMBASE, Cochrane Library, CINAHL, PEDro, Index to Taiwan Periodical Literature System, China National Knowledge Infrastructure, and the WanFang Med-Chinese BioMedical Literature Database. Data from completed clinical trials were also obtained from the World Health Organization International Clinical Trials Registry Platform. Reference lists of eligible articles were reviewed to identify additional studies for possible inclusion. E-mail alerts were established to identify newly released studies from the different databases that fell within the scope of our review.
Keywords used in the search included text words and controlled vocabulary (e.g., Medical Subject Headings), where available. On the basis of the MEDLINE (Ovid) search strategy, queries were revised to perform the best searches in the other databases. We also referred to the PRISMA 2009 Checklist 19 in order to determine eligibility. The MEDLINE (Ovid) search strategy is shown in Table 1.
Study inclusion and exclusion criteria
Types of studies
RCTs, with crossover or parallel group design, that evaluated needle acupuncture for AIMSS in patients with breast cancer were included. Only studies with adequate assessor blinding were included. Studies were excluded if they were nonrandomized trials, case reports, abstracts, or letters in order to allow a more thorough analysis based on the highest standards of scientific evaluation.
Types of participants
Participants were postmenopausal women with clinically diagnosed breast cancer. In particular, selected trials focused on patients with stage I–III breast cancer who experienced joint-related symptoms after taking an irreversible steroid inhibitor (exemestane) or a reversible nonsteroidal inhibitor (anastrozole or letrozole), which belong to the class of third-generation AIs, for at least 3 months. All participants in the RCTs had AIMSS with joint pain, measuring at least 3 points based on the Brief Pain Inventory–Short Form or other valid methods of pain assessment. Patients with metastatic breast cancer (stage IV) were excluded from our analysis, although the Food and Drug Administration has approved the use of AIs for this condition. These patients were excluded because of a possible bias of pain monitor form resulting from the metastatic bone lesions typically found in this stage of breast cancer.
Types of interventions
Studies that evaluated any type of invasive acupuncture were included. These included studies using manual acupuncture, electroacupuncture, and auricular (ear) acupuncture. For the consistency of the study design, trials that were designed as comparisons of noninvasive techniques (such as laser acupuncture, acupressure, acu-moxibustion, or transcutaneous electric nerve stimulation) applied in AIMSS were excluded. This meta-analysis focused exclusively on the effects of needle acupuncture.
Outcome measurement
Primary outcomes
The primary outcome measure was based on patient reporting of joint pain and stiffness intensity by using validated pain scales, such as (1) Brief Pain Inventory–Short Form (BPI-SF), 20 (2) Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), 21,22 (3) Functional Assessment of Cancer therapy–General (FACT-G), 23,24 (4) Modified Score for the Assessment of Chronic Rheumatoid Affections of the Hands, and visual analog scale. 25
Secondary outcomes
Secondary outcome measures included any of the following: (1) serum cytokine level changes, such as IL-1, IL-6, TNF-α, and interferon-gamma; (2) functional assessment, such as handgrip strength test or Health Assessment Questionnaire disability index; and adverse events (major or minor).
Data extraction, quality, and validity assessment
The titles and abstracts that matched the criteria of our study were independently read by two reviewers (Chien and Hsu), and the full texts of articles determined to have met this criteria were obtained. Final decisions on inclusion were made after examination of the full manuscripts. In cases of duplicate publications, the most recent and complete versions were selected. The quality of the studies was assessed independently by two reviewers using the validated 5-point modified Jadad Quality Scale, which considers the method of randomization, blinding, and a description of withdrawals and dropouts. 26,27 Trial quality was assessed by using the following five questions: Was randomization adequate? Was allocation concealed? Was a sham control used? Was the outcomes assessor blinded? Were dropouts and withdrawals accounted for?
When data were missing, the authors were contacted and asked to provide methodologic details. A study was rated as “adequate” for each item if the item was present in the paper or according to personal communication with the author; “inadequate” if the item was reported as not present in the paper or by the author as not present; or “unclear” if the item was not reported in the paper and the author could not be located.
To sum up, the modified Jadad Scale was used to assess four major aspects of the examined randomized clinical trials: (1) randomization procedure (1 point if patients were randomly allocated into groups); (2) allocation concealment (1 bonus point if the randomization procedure was appropriate); (3) dropout and withdrawal (1 point for a clear description of dropouts and withdrawals); (4) blinding (2 points) of patients and outcome assessors is considered critical. A sham control group (established to mimic acupoint stimulation) is a well-accepted method for patient blinding in acupuncture studies. Thus, 1 point was given for blinding of patients and 1 point for blinding of outcome assessors. Blinding of caregivers is not possible in RCTs that use manual therapy, such as acupuncture.
Therefore, each publication received a score from 0 (lowest quality) to 5 (highest quality). Studies were classified as “high quality” if they had a score of 3 or more. The critical appraisal of all 5 RCTs according to Jadad Quality Scale is shown in Table 2. To ensure the highest standard, the 5 RCTs selected were qualified as medium (3 points) to high quality (4–5 points).
Modified Jadad score (1 point for randomization, 1 point for appropriate randomization method, 1 point for describing withdrawals and dropouts, 1 point for patient blinding, and 1 point for assessor blinding) with a maximum score of 5 points. The higher the score, the higher the quality of the randomized clinical trial.
ITT, intention to treat.
Data synthesis and statistical meta-analysis
The effects of acupuncture on outcomes (mean change of pain and stiffness in related joints) after and during treatment relative to that at baseline were analyzed by estimation of mean differences, with 95% confidence intervals (CIs), using Review Manager (RevMan), version 5.0 for Windows (Cochrane Collaboration, London, United Kingdom). For mean differences, a point estimate of zero indicated no effect, and a point estimate less than zero favored acupuncture stimulation. Statistical heterogeneity was assessed by the chi-square test (p<0.05). The I 2 statistic was also used to assess variability among studies, and a value greater than 50% was considered to indicate significant heterogeneity. 28 A random-effects model was used if significant heterogeneity was present. Otherwise, results were obtained from a fixed-effects model.
Results
Study description
Searches of the 10 databases led to identification of 263 potentially relevant articles, 251 of which were ultimately excluded. Among the excluded files, 20 articles were duplicates, 223 titles/abstracts were irrelevant, and 8 did not have matching full text or were nonclinical trials (Fig. 1). The aim of this systematic review was to include full studies, not simply reports, so information from multiple reports was integrated if it was from the same study. If a full journal article and multiple meeting abstracts or trial registries were available, it is likely that the major information was available in the journal article. 18,29 Five unique studies were identified from 12 reports: Bao et al., 17,30,31 Oh et al., 32 –34 Crew et al., 35 –37 Crew et al. 16 , and Mao et al. 38,39 Data from all reports were extracted directly into a single data collection form. 29
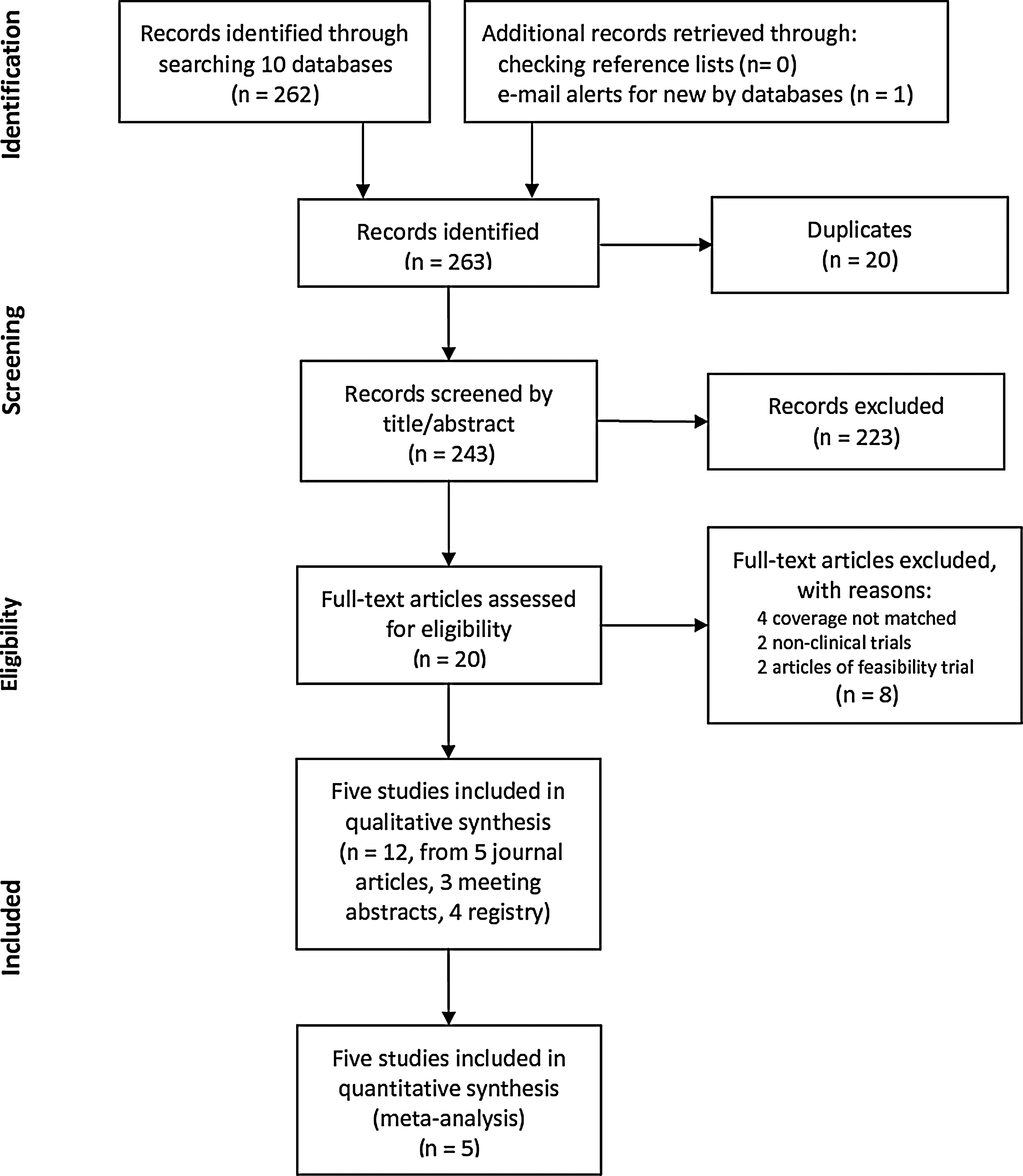
Study selection flowchart, based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. 19
The 5 RCTs, which enrolled a total of 207 patients, were analyzed in this systematic review (Tables 3 and 4). Four of the RCTs were conducted in the United States 16,17,35 and one was conducted in Australia. All of the RCTs selected used a two-arm parallel-group design at minimum, and the populations consisted of homogenous groups; white women constituted the majority in all included trials. Participants had stage I–III breast cancer and so were concordant with regard to diagnosis; this made the reviews less biased. However, the chosen acupuncture points were diverse, with LI4, GB34, and ST36 being the most common points. Two of the included trials discussed specific points at local joints, while the other 3 studies did not mention specific points. 16,40 All of the trials classified joint pain and stiffness as outcome measures, but only some of the studies measured the levels of cytokines without consistency. The duration of follow-up ranged from 6 weeks to 12 weeks.
AI, aromatase inhibitor; BPI-SF, Brief Pain Inventory–Short Form; HAQ-DI, Health Assessment Questionnaire Disability Index; RCT, randomized clinical trial; VAS, visual analog scale.
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; FACT-G, Functional Assessment of Cancer Therapy–General; IFN, interferon; IL, interleukin; M-SACRAH, Modified Score for the Assessment of Chronic Rheumatoid Affections of the Hands; TNF, tumor necrosis factor; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Methodologic quality
The methodologic quality of the trials was generally high (Table 2). Four of the 5 RCTs appropriately described the methods of randomization, 3 trials provided details regarding dropouts and withdrawals, 17,35 4 trials reported details about allocation concealment, 17,32,35 and all 5 trials used patient blinding and recorded adverse events.
Primary outcomes: effects of acupuncture on pain and stiffness of related joints
With the method of meta-analysis, there was significant between-study heterogeneity in the effects of acupuncture on BPI-SF pain score (I 2 =90%) and WOMAC stiffness of related joints (I 2 =93%). Among the 2 trials that reported data using the BPI-SF pain score (n=82), there was a trend for reduced pain in participants given acupuncture (mean difference, −2.07; 95% CI, −4.72 to 0.57; p=0.12) (Fig. 2A), although this was not statistically significant. Among the two trials that reported data using WOMAC stiffness (n=82), there was a trend toward reduced stiffness in patients given acupuncture (mean difference, −86.10; 95% CI, −249.11 to 76.92; p=0.30) (Fig. 2B), although this also was not statistically significant. There were too few studies to allow for meaningful analysis using a funnel plot. In addition, it was difficult to analyze changes in serum cytokine levels because of the heterogeneity of the trials.
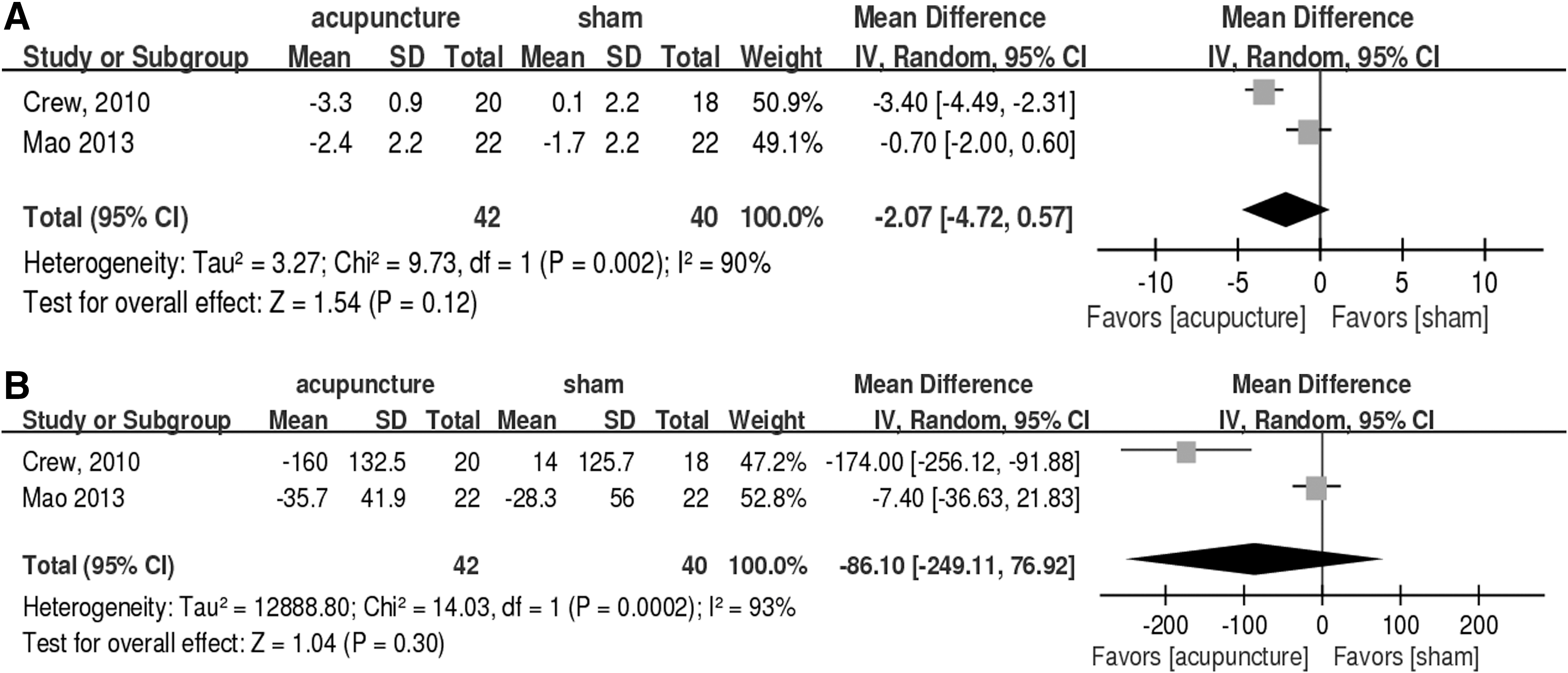
Forest plots of acupuncture effects.
Secondary outcomes
Only 2 RCTs measured serum cytokine levels to evaluate any change in inflammation status. Crew et al. (2007) used biomarkers, such as TNF-α and IL-1β, to monitor whether inflammation improved; no significance was observed after the acupuncture intervention (TNF-α: p=0.163; IL-1: p=0.150). 16 Another selected article, Bao et al. (2013) chose β-endorphin, TNF-α, IFN-gamma, IL-1, IL-6, IL-8, IL-10, IL-12, and IL-17 for comparison pre- and post-acupuncture; changes were not significant (p>0.05 for all cytokine measurements). 17 Meta-analysis of cytokine change could not be performed because of limitation of raw data requisition. Changes in inflammation cytokines may not be suitable for monitoring the AIMSS because the related mechanism of acupuncture in AIMSS still needs to be clarified.
With regard to adverse events, none of the 5 RCTs reported toxicities related to acupuncture, indicating that it is a safe form of therapy for AIMSS.
Discussion
All included clinical trials that assessed the effect of acupuncture for AIMSS were conducted since 2007, so the present systematic review is the first of its kind. All of these studies confirmed that acupuncture was feasible and safe, although the benefits and efficacy in the treatment of AIMSS remain controversial. Most studies indicated acupuncture was a promising nonpharmacologic modality that provided relief from AI-related joint pain and stiffness. However, clinical use of acupuncture is limited because of the lack of insurance coverage in Western countries; 41 this may explain why so few studies have examined the effect of acupuncture on AIMSS. Despite these limitations, we can focus on several major points.
First, although sham controls have been the most commonly used placebo in acupuncture studies, this may not be optimal because some patients apparently benefit from sham acupuncture as a result of the physiologic effects of needling, even when needling is not performed according to established principles. 42,43 For example, Crew et al. 35 reported that 22% of patients who received simulated acupuncture had a 2-point decrease in the BPI relative to baseline. 35 This is consistent with literature reports of a 25%–55% efficacy from use of nonacupoint and superficial insertion sham methods 44 and other studies reporting that sham acupuncture may be as efficacious as true acupuncture. 43 One of the 3 studies examined here confirmed that true acupuncture was superior to sham acupuncture in outcomes such as pain, stiffness, and physical well-being. 35 Other studies showed no significant differences in outcome measures. 17,32 Previous studies showed that real and sham acupuncture can lead to the release of endorphins and activation of pain-related neuromatrices, 45,46 so sham acupuncture may not be a true placebo. Further studies that include a nonacupuncture (or standard care) group may be required to better evaluate the efficacy of acupuncture. Second, because acupuncture may provide analgesia by downregulating proinflammatory cytokines, such as IL and TNF-α. 47 In the studies identified here, cytokine measurements were not consistent and showed no significant difference between the acupuncture and sham groups, except for a significant reduction of IL-17 in both groups in Bao and colleagues' study and a trend toward greater reduction in TNF-α level was also noted (p=0.095). 17 In Liu and colleagues' study (2012), IL-17 and other related cytokines may regulate the T-helper immune pathway by decreasing expression of IL-12 and the IL-12 RB2 subunit, which are linked to severe arthritis. 48 The similar changes in the serum marker in the sham and acupuncture groups may be due to the small sample size or the poor consistency of methodologic estimation. Moreover, only 1 of the examined studies measured estradiol and assessed the effect of acupuncture on estradiol concentration. 17 AIs are classified as reversible nonsteroidal drugs (anastrozole and letrozole) or irreversible steroidal drugs (exemestane), 2 but it is unknown whether the different kinds of AIs have different effects on the molecular pathways associated with AIMSS.
Acupuncture may also provide analgesia by increasing the levels of endogenous opioid peptides in the central nervous system 49 or by changing the levels of other signaling molecules such as serotonin, noradrenalin, dopamine, cholecystokinin octapeptide, glutamate, and γ-amino-butyric acid. 50 Thus, it may be useful to compare measurements of these endogenous substances in patients who have AIMSS and who are given acupuncture or sham treatments. It is uncertain which endogenous molecules should be measured in outcome measurements because multiple pathways may be involved in the pain relief provided by acupuncture. A Cochrane review of studies that used acupuncture to alleviate cancer-related pain concluded that the available evidence was inconclusive or of low quality. 51
Third, most of these trials used pain and stiffness as primary outcome measures and relied on patient-reported outcomes for end-point measurements. The use of patient-reported outcomes for assessment of functional improvement is valid and consistent based on results assessed by the BPI-Short Form, 20 the WOMAC, 22 the FACT-G, 23,24 and the Score for the Modified Assessment and Quantification of Chronic Rheumatoid Affections of the Hands. 52 However, questionnaire-based estimation reflects subjective symptom control, so more patients and treatment centers need to be included. In recent years, some studies have proposed the use of imaging-based measurements, such as magnetic resonance imaging or wrist ultrasonography, for objective assessment of structural changes. 53,54 Future studies should also consider the use of other secondary outcomes, such as thickening of the tendon sheath with intra-articular fluid retention and loss of grip strength. 55
Finally, the included studies have limitations. For example, the sample size is small. These studies did not show the difference in results with regard to stratified use of the AI. Whether arthralgia induced by steroidal AI or nonsteroidal AI would respond differently to acupuncture is unknown. Whether other treatment modalities are being used concurrently with acupuncture should also be considered; 4 of the 5 studies allowed patients to take their usual pain medication. Such variables should be considered because they can potentially influence the outcome of therapy.
This appears to be the first systematic review of the use of acupuncture for treatment of AIMSS in patients with breast cancer. All included trials were intermediate to high in quality. On the basis of the results of meta-analysis, acupuncture appears to lead to a trend toward reduced severity of joint pain and stiffness in AIMSS but has no obvious effects on inflammatory biomarkers. Perhaps other, more precise outcome measurement tools, such as image study or functional testing, should be considered for future studies. 56 Since the National Institutes of Health proposed that acupuncture is a legitimate therapeutic intervention for complementary medicine, the efficacy of acupuncture has become more accepted worldwide.
In conclusion, acupuncture is a safe treatment for AIMSS, although it had no statistically significant effects relative to sham treatment. Future trials of acupuncture for AIMSS should be designed with a more consistent acupuncture profile and with more objective outcomes measurements.
Footnotes
Author Disclosure Statement
No competing financial interests exist.