
Abstract
Background:
Persons living with HIV (PLWH) who also use crack cocaine may have stressful, chaotic lives and typically do not engage in standard medical care that addresses a multitude of extenuating life circumstances. Yoga/meditation (YM) improves quality of life (QOL) and biomarkers of stress, but the effect of this intervention is almost unknown in PLWH, particularly those who use crack cocaine.
Objectives:
This pilot study sought to compare the feasibility and acceptability of 60-minute, twice-per-week sessions of YM for 2 months with those of no-contact control and to evaluate the effects of the intervention on QOL (according to the Short Form-36, Perceived Stress Scale [PSS], and Impact of Events Scale [IES]) and salivary cortisol and dehydroepiandrosterone sulfate (DHEA-S) among PLWH who use crack cocaine.
Design:
Participants were randomly assigned to YM or no-contact control and were assessed at baseline, 2 months after the intervention, and 4 months' follow-up.
Results:
The YM program was acceptable and feasible, with high overall attendance (89%) and individual participation in yoga sessions (83%). YM participants showed modest improvements on QOL. The PSS total score and the IES intrusion score improved significantly 2 months after the intervention, but cortisol and DHEA-S did not change.
Conclusions:
This pilot study showed a high level of feasibility and acceptability and modest effects on measures of QOL among PLWH who use crack cocaine. The results suggest utility of YM as a simple, safe, and inexpensive format to improve QOL in a population that has many medical difficulties and extenuating stressors.
Introduction
W
Managing these symptoms is vital for coping with HIV and AIDS in PLWH. 1,10 Pharmacologic interventions used to improve psychological, immunologic, and behavioral responses, including QOL, 11,12 are sometimes associated with increased toxicity and adverse effects for the patient, making these interventions intolerable for many. Therefore, to relieve adverse effects of ART and physical and psychological symptoms of HIV, some PLWH turn to other means, including complementary and alternative medicine (CAM). 13 –15 However, some CAM (e.g., herbs and certain nutrients) may negatively interact with ART. 13,15,16 Yoga/mediation (YM), a mindfulness-based stress reduction technique, is a nonpharmacologic intervention devoid of the adverse effects of herbal CAM. YM is increasingly being used to manage symptoms and risk factors associated with many chronic diseases, 17,18 such as cancer, 19,20 diabetes, 21 hypertension, 22 cardiovascular disease, 23 and AIDS. 24 –28 Studies in PLWH showed that YM decreased pain and anxiety, 1,29 increased CD4 T lymphocytes independently of ART, 30 increased CD2+ counts, 31 improved overall survival rates, 32 and increased motivation for drug abstinence and HIV prevention behaviors. 33
A large body of evidence suggests that HIV and ART, along with drug abuse, lead to a wide spectrum of abnormalities in immunologic, neurologic, and neuroendocrine systems, even during the asymptomatic phase of infection. 34 –37 Dysregulated cortisol profiles in response to stress or disease have profound effects not only on behavioral, circulatory, endocrine, metabolic, and immune functioning but also on cognitive functioning and behaviors. 38,39 HIV also has a deleterious effect on another adrenocorticosteroid hormone, dehydroepiandrosterone (DHEA), which is converted to a more stable form, DHEA-S, in the adrenal glands, liver, and small intestines. Various studies have reported an increase in cortisol and a decrease in DHEA-S in asymptomatic PLWH, 38 suggesting that the cortisol-to-DHEA-S ratio may be a useful biomarker for stress reduction interventions.
The practice of YM generates a more relaxed, calmer mental state and allows individuals to cope with symptoms of anxiety, depression, and stressful situations, common problems faced by PLWH. However, research on these increasingly popular nonpharmacologic medical interventions in PLWH remains limited. Furthermore, compared with PLWH who are not substance users, the subpopulation of PLWH who use crack cocaine is typically more socioeconomically unstable and has a greater tendency to be unemployed, to be homeless, 40 and to have legal problems and stints in detention. As a result this group is more difficult to follow. The effect of YM does not seem to have been studied in this population. Therefore, this pilot study was initiated to assess the potential feasibility and acceptability of a YM program within this subpopulation and to explore effects on their QOL and circulating cortisol and DHEA-S levels.
Methods
Participants
Following the approval of the University of Miami Institutional Review Board for human subjects research, English-speaking PLWH were recruited from the Patient Education Program of the Division of Infectious Diseases at the University of Miami Miller School of Medicine. Potential participants were interviewed to assess initial interest in and eligibility for the study. They were asked three questions: (1) Do you use or have you used drugs (i.e., crack cocaine)? (2) Are you HIV positive? and (3) Do you speak and/or understand English? Those who answered “yes” to all three questions were then asked if they were interested in participating in or learning more about the study. Twenty-four eligible persons completed informed consent and Health Insurance Portability and Accountability Act forms before participating in the study. Then, each participant was randomly assigned to one of two groups—YM (n=12) or control (n=12)—by picking an unmarked envelope generated by a computer program.
QOL
QOL was assessed at baseline, at the end of the intervention (i.e., at 2 months), and at follow-up (i.e., at 4 months) with three measures: (1) the Short Form (SF)-36 Health Survey, (2) the Perceived Stress Scale (PSS), and (3) the Impact of Events Scale (IES). The SF-36 Health Survey 41 provides psychometrically based physical and mental health summary measures and a preference-based health utility index. This generic measure does not target a specific age, disease, or treatment group. The 14-item PSS 42 measures how often, over the past 30 days, an individual appraises situations in their lives as being stressful on a scale of 0 (never) to 4 (very often). Positive items are reverse scored, and items are summed to create a PSS total score. The IES 43 is a 15-item self-report measure used to assess the level of distress responses in the past week to a specific traumatic event. In addition to the total score, two subscales were also calculated that measure intrusive thoughts and avoidance behaviors.
Saliva collection and assay of cortisol and DHEA-S
Cortisol and DHEA-S are synthesized in the adrenal gland from a common pathway by hydroxylation of pregnenolone and progesterone. Most of the hormones are bound to proteins in the blood, but measurable amounts of free hormones also migrate to saliva, 44 thus making this fluid a good source of the hormone's measurement. Saliva samples were collected from each participant at baseline, at the end of the intervention (i.e., at 2 months), and at follow-up (i.e., at 4 months). Before saliva collection, participants were asked to rinse their mouth to exclude any food particles or other extraneous materials and offered sugarless gum to stimulate saliva production. A sterile cotton swab was placed under the tongue for 2 minutes to absorb 1–2 mL of saliva and was then transferred to a Salivette® tube, specifically designed for collecting saliva for assays of free-circulating hormones (Sarstedt Inc., Newton, NC). To minimize known diurnal variations in hormonal levels, the saliva samples were collected at the same time of the day (10 a.m. to 12 p.m.). The samples were stored on ice and transferred to the laboratory within 2 hours, where they were centrifuged and the supernatant fluids were frozen at −70°C until assayed for cortisol and DHEA-S. After thawing at room temperature, the saliva samples were centrifuged to separate any cell debris and other contaminants.
Cortisol and DHEA-S were assayed by the enzyme-linked immunosorbent assay method using kits obtained from Immuno-Biological Laboratories, Inc. (IBL-America, Minneapolis, MN) according to the instructions provided by the vendor. The intra- and interassay coefficients of variation of this method are 2.62%–4.07% and 2.04%–4.94% for cortisol and 7.8% or less and 14.9% or less for DHEA-S.
YM program
The YM group was given a description of the program in the first session, including the sequence of yogic postures and general instructions. The intervention included two 60-minute sessions of YM each week for 2 months (for a total of 16 sessions). A certified yoga instructor administered the YM program at least 2 hours after a meal at the University of Miami Medical Wellness Center. The YM program was designed to meet the needs of the participants and provided all the essential elements of different yogic techniques (i.e., warm-up yogic body movements, yogic breathing techniques, meditation, yogic asana, and sava asana [yoga Nidra] for relaxation). Meditation was followed with silent, regular breathing while focusing on an internal sound or word.
Warm-up exercises included simple muscle stretching exercises, surya namaskar (Sun salutation), whereas yogic-breathing techniques included the following. (1) Alom-vilom pranayam (alternate nostril breathing) consists of slow, smooth, and controlled breaths. Inhalation is performed by one nostril, and then the other nostril exhales the air; this process is then reversed. A special hand position is used to gently close the nostrils in alternating fashion. (2) Kapalabhati consists of a series of fast successive bursts of exhalations followed by automatic passive inhalation. In normal breathing (approximately 15 breaths per minute), inhalation is active and exhalation is passive. In Kapalabhati, the process is reversed and rapid (approximately 120 breaths per minute); exhalation becomes active and inhalation passive. Persons with high blood pressure, ischemic heart disease, a herniated disc, or spondylolysis were advised not to do Kapalabhati. (3) Bhastrika is similar to Kapalabhati, except that breathing is focused on the upper torso, rather than the abdomen. (4) Bhramari (humming bee pranayama) is performed by exhaling slowly but forcefully through the nostrils with a high humming sound. (5) Sava asna (yoga Nidra, a yogic sleep for relaxation) involves lying in the supine position with the eyes gently closed, taking regular deep breaths, and relaxing each muscle group and body part. After 30–60 seconds, the participant was asked to slowly awaken by opening the eyes and stretching various parts of the body. 1,45,46
Control group
The control group completed the same assessments as the YM group. Control group participants were not given any form of intervention and were contacted only to schedule their assessments.
Statistical analysis
Data were analyzed by using SPSS software, version 22 (IBM, Inc., Chicago, IL). Frequency and descriptive statistics were calculated on all variables. Linear mixed modeling was used to assess the fixed effect of time by randomization on changes in the outcome variables from baseline, postintervention, and follow-up. If the type III test of the fixed effect of time by randomization was significant, then pairwise comparisons were used to determine the unique differences in effects over time by study arm between baseline, postintervention, and 2-month follow-up for the outcome variables. Linear mixed modeling with heterogeneous compound symmetry covariance accounted for subject attrition, intercorrelated responses between time points, and nonconstant variability. Additionally, generalized linear modeling was used to evaluate the effect of time on the outcome variables for the YM group only. The Mauchly test of sphericity and the Huynh-Feldt degrees of freedom correction factor were used to account for heterogeneity among time points. An α level of 0.05 was used for all analyses.
Results
Demographic characteristics of the participants (Table 1) did not differ between the YM and control groups. The feasibility of the study was widely supported, with an overall YM session attendance rate of 89%; the average number of sessions attended per participant was 88%, and the average attendance per session was 83% (Table 1). At the follow-up assessments, 6 of 12 (50%) and 5 of 12 (42%) participants in the control group and 10 of 12 (83%) and 9 of 12 (75%) participants in the YM group, respectively, were retained.
Ages are expressed as mean±standard deviation (range).
YM, yoga/meditation.
QOL
The descriptive information for the QOL variables for the YM and control groups is presented in Tables 2 and 3, respectively. On the SF-36, the fixed effects for time, randomization, and time by randomization were nonsignificant for the physical functioning, role-physical, vitality, social functioning, and mental health scales. For general health, the fixed effect for randomization (F[1,17.8]=7.7; p<0.05) was significant, but the effects for time and time by randomization were nonsignificant. For role-emotional, the fixed effect for randomization (F[1,16.8]=18.7; p<0.001) was significant, but the effects for time and time by randomization were nonsignificant. For bodily pain, the fixed effect for randomization (F[1,17.3]=9.9; p<0.01) was significant, but the effects for time and time by randomization were nonsignificant. For the PSS total score, the fixed effect for time (F[2,16.9]=3.6; p=0.05) was significant, but the effects for randomization and time by randomization were nonsignificant. On the IES, the fixed effects for time, randomization, and time by randomization were nonsignificant for the total and avoidance scores. For the intrusion score, the fixed effect for time (F[2,23.9]=8.5; p<0.01) was significant, but the effects for randomization and time by randomization were nonsignificant.
Values are expressed as the mean±standard deviation (minimum, maximum).
SF-36, SF-36 Health Survey; IES, Impact of Events Scale; PSS, Perceived Stress Scale.
Values are expressed as the mean±standard deviation (minimum, maximum).
QOL for YM group only
On the SF-36, the effect of time was nonsignificant for all scales. For the PSS total score, the effect for time (F[1.9,17.1]=3.6; p=0.05) was significant, and the pairwise comparisons revealed that the postintervention score was significantly lower than baseline (mean difference, 4.7; standard error of the mean [SEM], 1.8; 95% confidence interval [CI], 0.6–8.8; p<0.05) (Fig. 1). The IES total and avoidance scores showed no significant effect for time. For the intrusion score, the effect for time (F[1.7,15.7]=5.0; p<0.05) was significant, and the pairwise comparisons revealed that the postintervention (mean difference, 7.8; SEM, 2.6; 95% CI, 1.9–13.7; p<0.05) and follow-up (mean difference, 5.4; SEM, 1.7; 95% CI, 1.5–9.3; p<0.05) scores were significantly lower than baseline (Fig. 1).
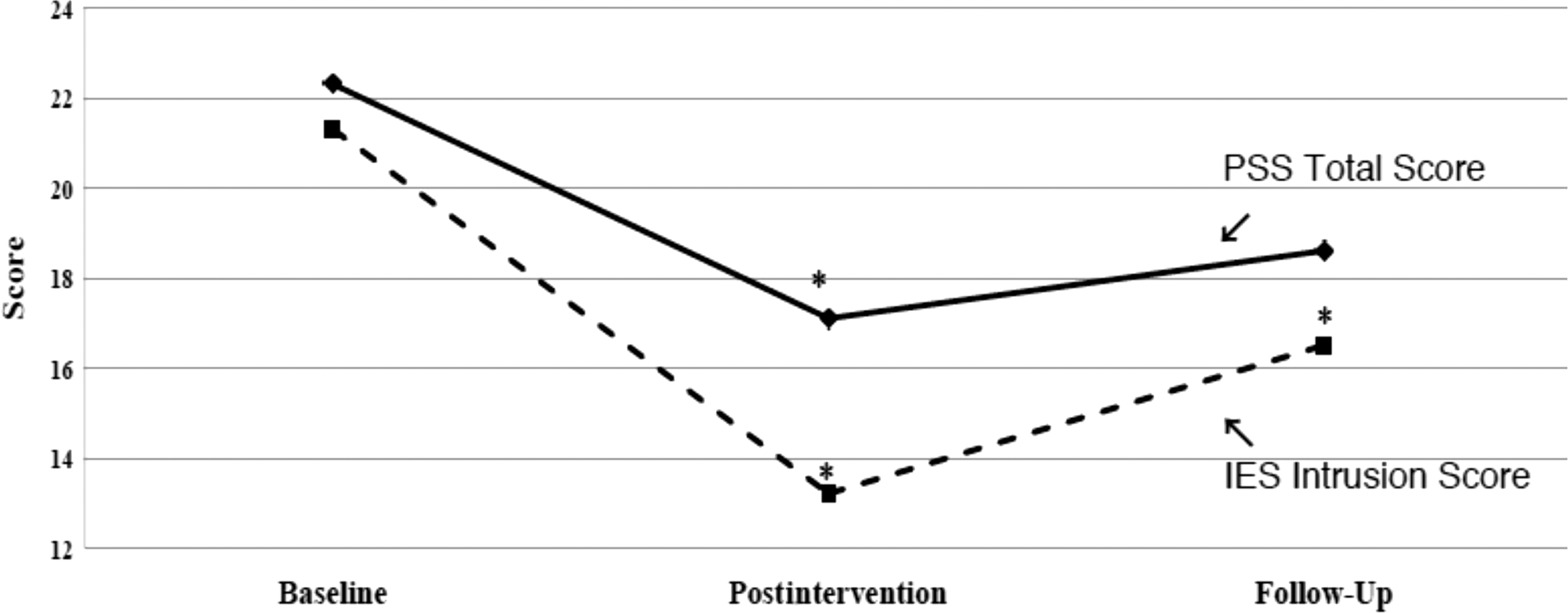
Quality of life scores for yoga/meditation group: Perceived Stress Scale (PSS); Impact of Events Scale (IES) Intrusion. *p<.05 compared with baseline.
Cortisol, DHEA-S, and cortisol-to-DHEA-S ratio
Cortisol and DHEA-S levels and the cortisol-to-DHEA-S ratios are presented in Table 4. The fixed effects for time, randomization, and time by randomization were nonsignificant for cortisol, DHEA-S, and cortisol-to-DHEA-S ratio. For the YM group only, the effect of time was nonsignificant for all variables.
Values are expressed as the mean±standard deviation (minimum, maximum).
DHEA-S, dehydroepiandrosterone sulfate.
Discussion
This pilot study showed feasibility, acceptability, and modest improvement in QOL in response to a YM intervention among PLWH crack cocaine users. A high rate of attendance and retention until the end of the intervention suggests that the YM program was successful in attracting and engaging the participants. Compared with the YM group, 33% fewer control group participants were retained at postintervention and follow-up. Reasons for a lower retention rate in the control group are not known and purely speculative. The participants not using YM might have migrated, become sick or hospitalized, or ended up in detention centers, or simply were uninterested in continuing participation, thus becoming unreachable. If this hypothesis is proven, the use of a YM program becomes more important in this population. In light of these findings, it is possible that if the control group participants are engaged in some type of activity and regularly contacted, their retention may increase.
Although YM modestly improved participants' QOL, cortisol and DHEA-S levels did not change. A small sample size, short intervention time (16 sessions, two sessions/week, for 2 months), and the nature of the subpopulation used in this study may have contributed to the observed anomaly. YM, a subjective intervention, may require continuous repetition for a longer period before desirable psychological and biological effects can be observed. Reports on the effects of relaxation therapies on cortisol levels in PLWH are mixed, with some studies reporting no correlation 47,48 and others reporting a significant reduction on cortisol levels. 49
Generally, PLWH have high degrees of emotional distress, pain, and anxiety, which may negatively affect their QOL. Perhaps to cope with these symptoms, some PLWH increasingly use and abuse illicit substances and become addicted. The use of substances significantly decreases adherence to ART, 50,51 leading to unsuccessful viral suppression, increasing clinical progression of the disease, and development to ART drug resistance, 52 further deteriorating patients' QOL. Significant improvements in the PSS total score and the IES intrusion score in the YM group at postintervention were noteworthy. These findings suggest that a longer YM program might further improve QOL in this population. Mindfulness-based stress reduction techniques, including YM, have previously shown a positive effect on a variety of physical and psychological conditions that often plague PLWH crack users. For example, YM can improve symptoms of stress, anxiety, depression and pain, drug dependence, and QOL and alter disease progression. 1,29,53 The current report appears to be the first on the effect of YM in PLWH crack cocaine users, and the results are consistent with the literature.
The mechanism of action of YM is not known. Its effect may be due to an underlying physiologic and psychological process occurring in multiple disorders, and therefore it is not specific to any particular disease. 54 YM transcends the limitations of physical science and encourages the development of self-control and motivation, which is obviously pertinent and beneficial to PLWH using crack cocaine. 45,55 According to Rama, “most diseases are classified, to some degree, as psychosomatic, having their origin in or being influenced by the human mind, thought, and emotions.” 46 In meditation, the individual strives for a state of attentiveness, concentration, and relaxation. This state is one of a tranquil mind, which improves the activities of the immune system and reduces physical and mental stress. 46 Thus, our findings of improved QOL, particularly better-perceived stress, are important for this population.
The findings of the study are limited by a small sample size and only a 2-month intervention and 2-month follow-up period. In addition, the control group received no intervention. Moreover, because of the nature of the study, markers of disease progression, effect on drug using behaviors, and adherence to ART were not measured. Therefore, the results should be considered preliminary. Further study using a larger sample size and a longer duration of intervention is warranted to address these important questions.
Conclusion
A pilot study of YM was successfully conducted to investigate its feasibility and acceptability in a population that is often difficult to follow and that typically does not regularly use health services. This YM program proved to be feasible and acceptable among the program participants, suggesting that a larger randomized trial should be conducted to evaluate YM's influence on PLWH crack users' QOL, perceived stress, drug dependence, and disease progression. Additionally, in contrast to pharmacologic interventions, which are toxic and costly, this nonpharmacologic, nontoxic, and noninvasive therapeutic approach may be used widely in PLWH and patients with other chronic diseases.
Footnotes
Acknowledgments
This study was supported by developmental grant P30 A1073961 from the National Institutes of Health (NIH) through the Miami Center for AIDS Research at University of Miami Miller School of Medicine.
The NIH had no role in the design and conduct of the study; collection, management, and analysis of the data; or preparation, review, and approval of the manuscript.
The views expressed herein are those of the authors and do not necessarily reflect the views of the NIH. Dr. Ram P. Agarwal had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
The authors thank Thomas Tanner, Nestor Chardon, and Maria Tapia for participant recruitment; Adam Ganuza for project coordination; Beatriz Osario for yoga instruction; Claudine Johnson for providing the Medical Wellness Center facilities; Kristopher L. Arheart for statistical analysis; and Erika M. Richardson for manuscript preparation.
Author Disclosure Statement
No competing financial interests exist.