
Abstract
Objectives:
To evaluate the existing data on aromatherapy interventions for improvement of sleep quality.
Design:
Systematic literature review and meta-analysis on the effects of aromatherapy.
Study Sources:
Electronic databases, including the Korea Education and Research Information Service (KERIS), Korean studies Information Service System (KISS), National Assembly Library, and eight academies within the Korean Society of Nursing Science, were searched to identify studies published between 2000 and August 2013.
Study Selection:
Randomized controlled and quasi-experimental trials that included aromatherapy for the improvement of sleep quality. Of the 245 publications identified, 13 studies met the inclusion and exclusion criteria, and 12 studies were used in the meta-analysis.
Results:
Meta-analysis of the 12 studies using a random-effects model revealed that the use of aromatherapy was effective in improving sleep quality (95% confidence interval [CI], 0.540–1.745; Z=3.716). Subgroup analysis revealed that inhalation aromatherapy (95% CI, 0.792–1.541; Z=6.107) was more effective than massage therapy (95% CI, 0.128–2.166; Z=2.205) in unhealthy (95% CI, 0.248–1.100; Z=3.100) and healthy (95% CI, 0.393–5.104; Z=2.287) participants, respectively.
Conclusion:
Readily available aromatherapy treatments appear to be effective and promote sleep. Thus, it is essential to develop specific guidelines for the efficient use of aromatherapy.
Introduction
S
Drug therapies, including sleeping pills and antidepressants, are widely used as clinical interventions for sleep disorders. However, problems such as lethargy and confusion during the daytime and habitual drug abuse 4 have increased interest in nonpharmacologic approaches to sleep disorders. Consequently, several interventional studies have been conducted to verify the effectiveness of behavioral and circadian rhythm therapies.
Recently, aromatherapy has also become a common nursing intervention because it is economical, has fewer adverse effects than drug therapies, and improves the sense of well-being. 5 Aromatherapy entails the use of oils extracted from flowers, stems, leaves, roots, and fruits of various plants absorbed into the body through the skin or respiratory system to improve mental and bodily health. The effects of aromatherapy are achieved through inhalation, bathing, or massage. 6 Aromatherapy use is simple, does not require special instruments, and results in positive effects even when used for only a short time. The scent particles reach the limbic system through the olfactory nerves and can produce sedative and relaxant effects, which in turn influence blood pressure, heart rate, reproduction, memory, and stress response. 7
Various studies have evaluated the effects of aromatherapy, and results have indicated that aromatherapy decreased many psychological factors, including depression, anxiety, and stress; 8 had positive effects on physiologic factors, such as fatigue, blood pressure, pulse, and sleep; 9,10 and relieved pain. 11 The prior studies analyzed diverse uses of aromatherapy, as well as the use of aromatherapy in various populations, including night shift nurses, elderly individuals, patients with chronic disease, inpatients, middle-aged women, and college students. 9,10,12,13 Prior studies on the use of aromatherapy for sleep improvement used such methods as inhalation, massage, and skin application and mixtures of such oils as lavender, geranium, mandarin, bergamot, and marjoram. The results of these studies likewise indicated that the effects of aromatherapy on sleep improvement were significant. 14,15
Although investigations into the effects of aromatherapy on improving sleep quality have continued, the application methods, areas to which aromatherapy oils are applied, the duration of application, the types of aromatherapy oils used, and the mixture ratios of the oils have differed across studies. Therefore, a systematic analysis is necessary to verify the reported effects and to present scientific standards for the conduct of aromatherapy studies. Given the current emphasis on proof-based practice, it is critical to provide conclusive evidence of the effectiveness of aromatherapy application methods as a nursing intervention for sleep improvement.
The objectives of the current study were to conduct a systematic literature review and meta-analysis to evaluate the reported effects of aromatherapy on sleep improvement and to present evidence and scientific standards for the application of aromatherapy.
Methods
Study design
This systematic literature review and meta-analysis analyzed the reported effects of aromatherapy used as a treatment for sleep improvement.
Literature search strategies
The key parameters of the literature searches conducted were as follows. The participants were adults aged 20 years or older. The intervention consisted of all types of aromatherapies (inhalation, massage, and skin application). The comparisons included no intervention or other intervention (massage without application of aroma oil). Outcomes were measures of sleep improvement (sleeping time, sleep efficiency, the quality of sleep, and the degree of satisfaction with sleep).
Databases used for literature search and words searched
The databases searched included the Korea Education and Research Information Service (RISS), the Korean studies Information Service System (KISS), and the National Assembly Library. Academic journals from eight academies within the Korean Society of Nursing Science were also searched. The words searched included the following: aromatherapy, scent therapy; sleep disorder, insomnia, quality of sleep, and degree of satisfaction with sleep.
Literature selection and exclusion criteria
Reports of studies published in Korea after 2000 that included aromatherapy used by adults as a main intervention and reported at least one of the intervention results (quality of sleep, degree of satisfaction with sleep, sleep efficiency, or sleep improvement) were selected. College research papers, theses, exhibitions, presentations, review articles, overlapping publications, and research involving animal experiments were excluded.
Literature search results
Two researchers, using three different processes, selected the publications included in the current study (Fig. 1). The words chosen for the literature search were mixed and then used to query the RISS, KISS, National Assembly Library, and the academies under the Korean Society of Nursing Science databases. A total of 202 publications, excluding overlapping studies, were selected from the 245 studies included in the databases. A total of 176 studies were excluded on the basis of title and abstract, and an additional 13 studies were excluded after an evaluation of the full text. Thirteen studies were selected for final inclusion in the current study.
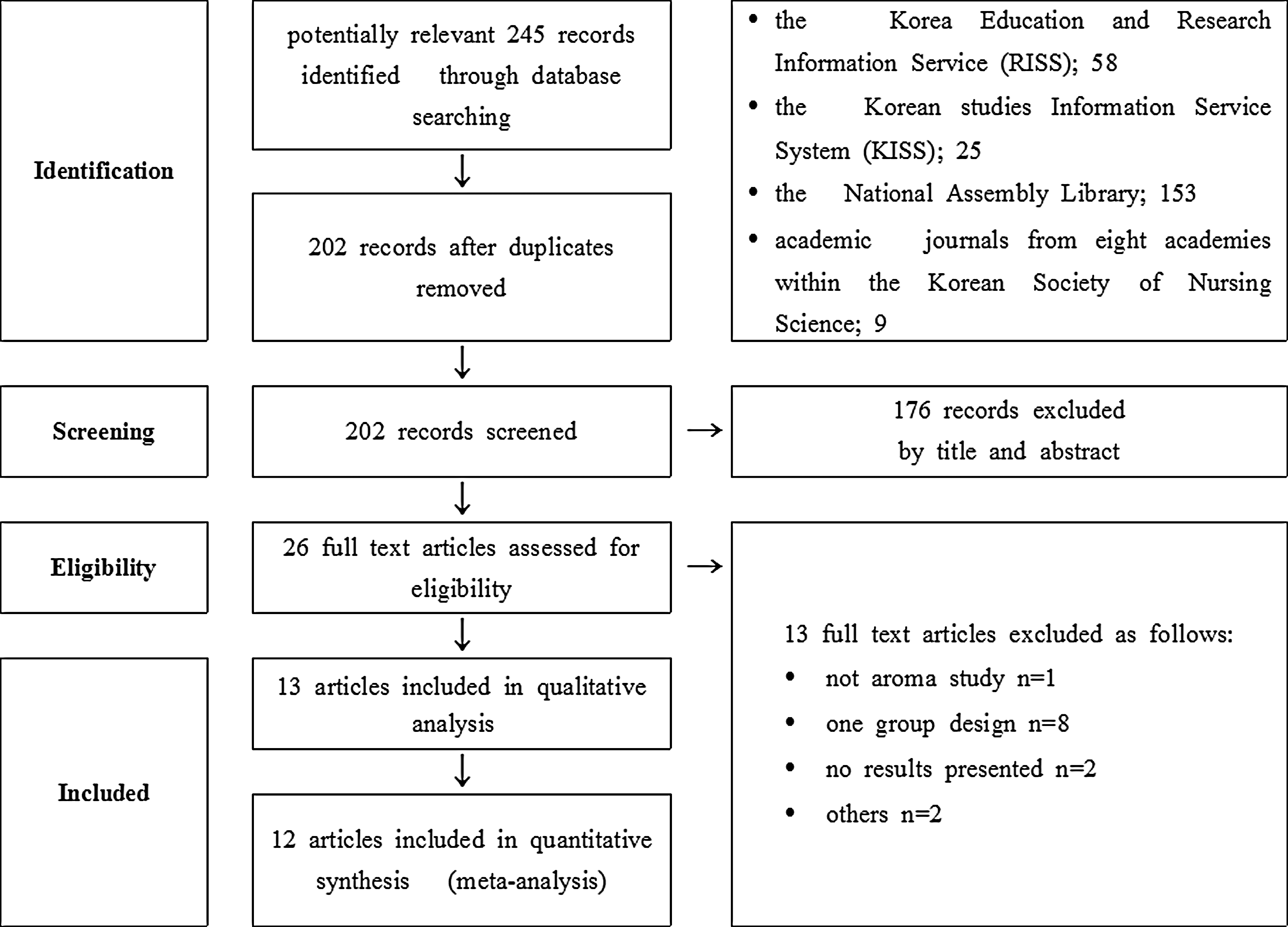
Flowchart of study selection.
Evaluation of study quality
The quality of the studies was evaluated using the quantitative research evaluation framework presented by the McMaster University Evidence-Based Practice Research Group. 16 The framework comprised questions that evaluated eight areas: the purpose of the study, background literature, study design, sampling, results, interventions, conclusions, and meanings. Each question was judged by the responses “yes,” “no,” or “not applicable.” Judgments regarding literature that did not satisfy the quality standards were made following a discussion between two researchers.
Data analysis
Systematic literature review
Results from the 13 papers selected following the systematic literature review were analyzed, encoded, and arranged into forms. The forms included sections on research design, number of participants, standards for participant selection and exclusion, measurement variables and tools, result variables, and statistical values. To maintain accuracy during the process, two researchers independently conducted evaluations, and the results were cross-checked and compared for inter-rater agreement.
Meta-analysis
Statistical analysis of the effect size was conducted by using Comprehensive Meta-Analysis software, version 2.2.064 (Biostat, Englewood, NJ). Out of the 13 studies, one lacked appropriate statistical analysis and was excluded. Thus, 12 studies were included in the effect size analysis. Studies used for the meta-analysis had different scales and therefore integration of the measured values into one unit was necessary. Accordingly, a standardized mean difference was calculated and used for transformation into effect size (Z).
The Higgins I2 test for homogeneity was conducted to summarize the statistical results of each study. When the calculated I2 value was lower than 25%, statistical heterogeneity was considered low, and when the I2 value exceeded 50%, statistical heterogeneity was assumed. 17 According to the analysis results, the hypothesis of homogeneity was rejected, and the effect size calculated using a random effect model and 95% confidence interval [CI] were presented. 18 In addition, subgroup analysis by each categorical variable of major research characteristics was conducted to explore mediator variables. A funnel plot and Egger linear regression asymmetry test were used to test publication bias and sensitivity of the research papers used in the current study. 19
Results
Research trends on the effects of aromatherapy on sleep
Research on the effects of aromatherapies included in this study are shown in Table 1. According to the analysis results, 9 of the 13 studies used validated tools to measure effects. The number of individuals in the studies was 36–72.
RCT, randomized controlled trial.
Trends in research conducted on the effects of aromatherapy on sleep over the past 10 years were examined. Among the 13 studies identified, most were conducted within the past 5 years; 5 studies (38.5%) were conducted in 2011, 2 in 2009, and 2 in 2012. As for study participants, 3 studies included adults and elderly individuals (23.1%), 7 studies included patients with chronic or other specific diseases (53.8%), and 3 studies included hospitalized patients (23.1%). With regards to study design, 4 studies had a randomized control group (30.9%), 1 study was a cohort study (7.7%), and 8 studies were pre/post experimental group studies that included a control group (61.5%).
Aromatherapy variables
Results of the analysis of variables in the papers related to aromatherapy indicated that lavender and bergamot aroma oils were used most often. Two studies used lavender oil (15.4%), and two each used a mixture of lavender and bergamot; lavender and peppermint; or lavender, bergamot, and chamomile (15.4%). The remaining studies involved clary sage, rosewood, lemon, marjoram, ylang, eucalyptus, and rosemary. Among the aroma application methods, seven studies involved massage (53.7%), three studies entailed direct inhalation methods after spraying the aroma on a gauze or a handkerchief (30.8%), three studies involved indirect inhalation methods after placing the aroma in a necklace or a pillow (23.1%), and one study applied the aroma to a joint area in a poultice (7.7%).
Measurement variables and results on the effects of aromatherapy on sleep
Effect variables used in the studies were the quality of sleep, degree of sleep disorder, degree of satisfaction with sleep, and sleep patterns. The four studies measured the quality of sleep as an effect variable, of which three reported that aromatherapy was effective. Eight studies measured the degree of sleep disorder, of which seven reported that aromatherapy was effective. One study measured the degree of satisfaction with sleep and one study included sleep efficiency, both of which reported that aromatherapy was effective.
Effect size of aromatherapy
Twelve of the selected papers were used to analyze effect size of aromatherapy on sleep. Heterogeneity of the 12 papers was verified (I2 =91.84%; p<0.001), and a random-effects model was used. The resulting effect size was 3.72 (95% CI, 0.54–1.75; p<0.001), which indicated that aromatherapy significantly improved sleep (Fig. 2).
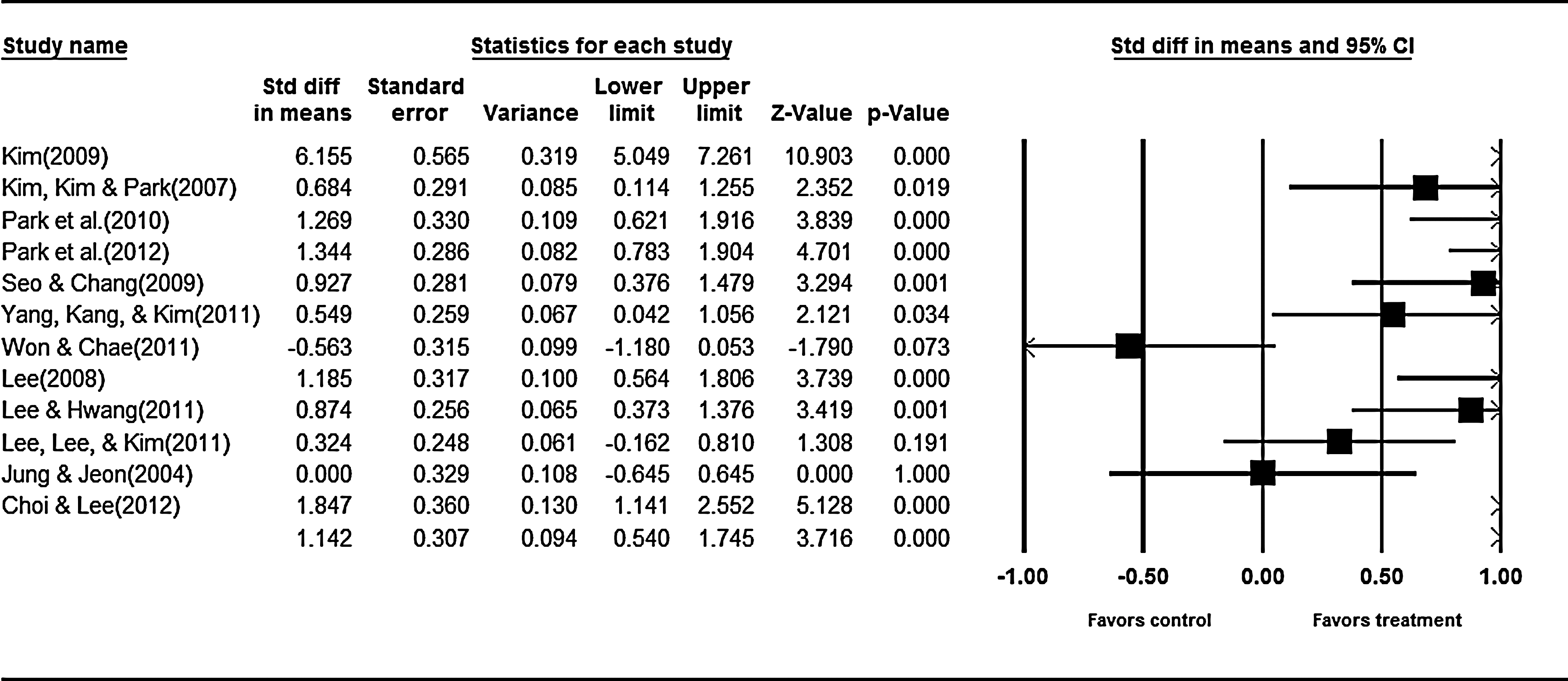
Effect size of aromatherapy related to sleep. Subgroup inhalation: heterogeneity: tau 2 =0.09, Q=8.04, df=4 (p=0.090), I2 =50.23%. CI, confidence interval; df, degree of freedom.
A meta-analysis was conducted based on the intervention factors of aromatherapy application method and the participants' health condition. Inhalation therapy (95% CI, 0.79–1.54; Z=6.11; p<0.001) was more effective than massage therapy (95% CI, 0.13–2.17; Z=2.21; p=0.027), and the effect size for participants with a disease (95% CI, 0.25–1.10; Z=3.10; p=0.002) was larger than that for healthy participants (95% CI, 0.39–5.10; Z=2.29; p=0.022) (Figs. 3 and 4).
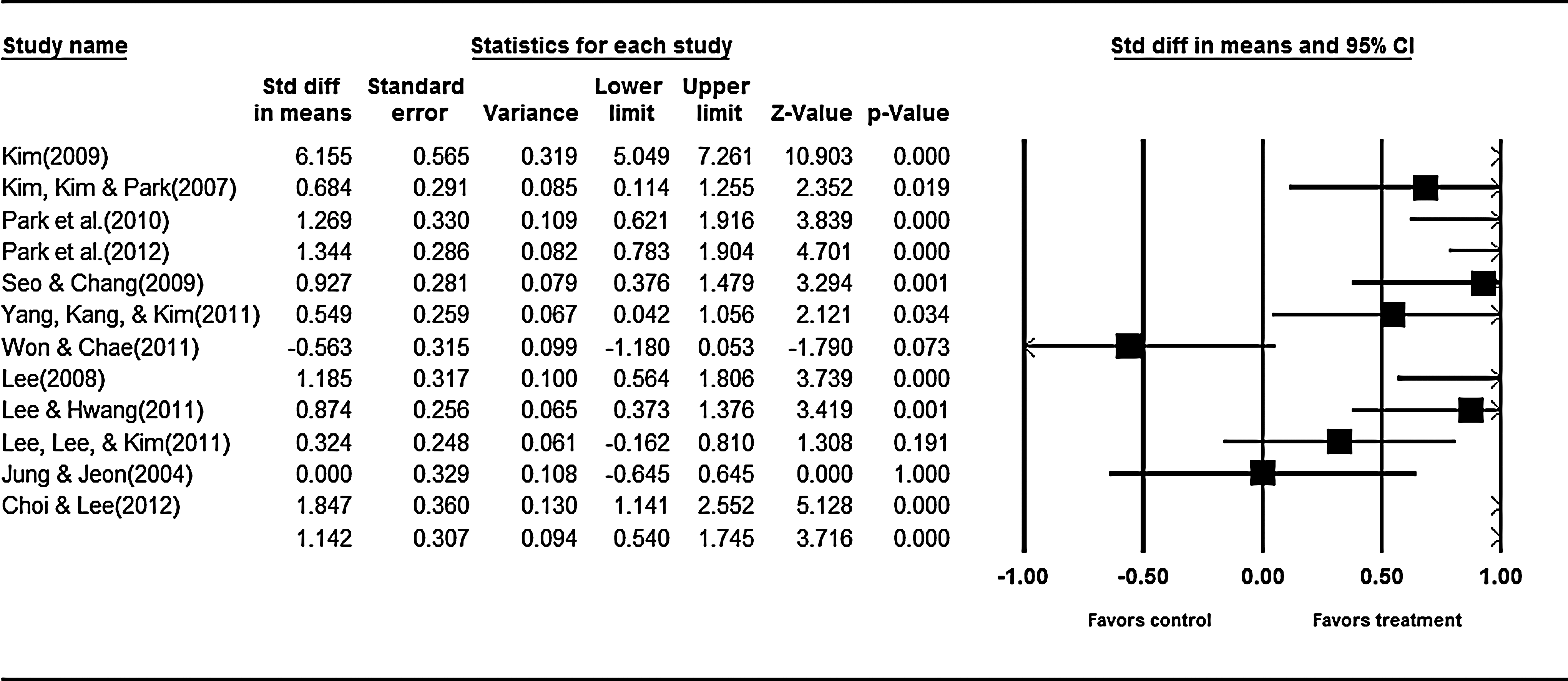
Effect size of aromatherapy according to the method applied. Test for overall effect size: Z=6.107, p<0.001. Subgroup massage: heterogeneity: tau 2 =1.78, Q=119.55, df=6 (p<0.001), I2 =94.98%. Test for overall effect size: Z=2.21, p=0.027. Total heterogeneity: tau 2 =1.03, Q=134.77, df=11 (p<0.001), I2 =91.84%. Test for overall effect size: Z=3.72, p<0.001.
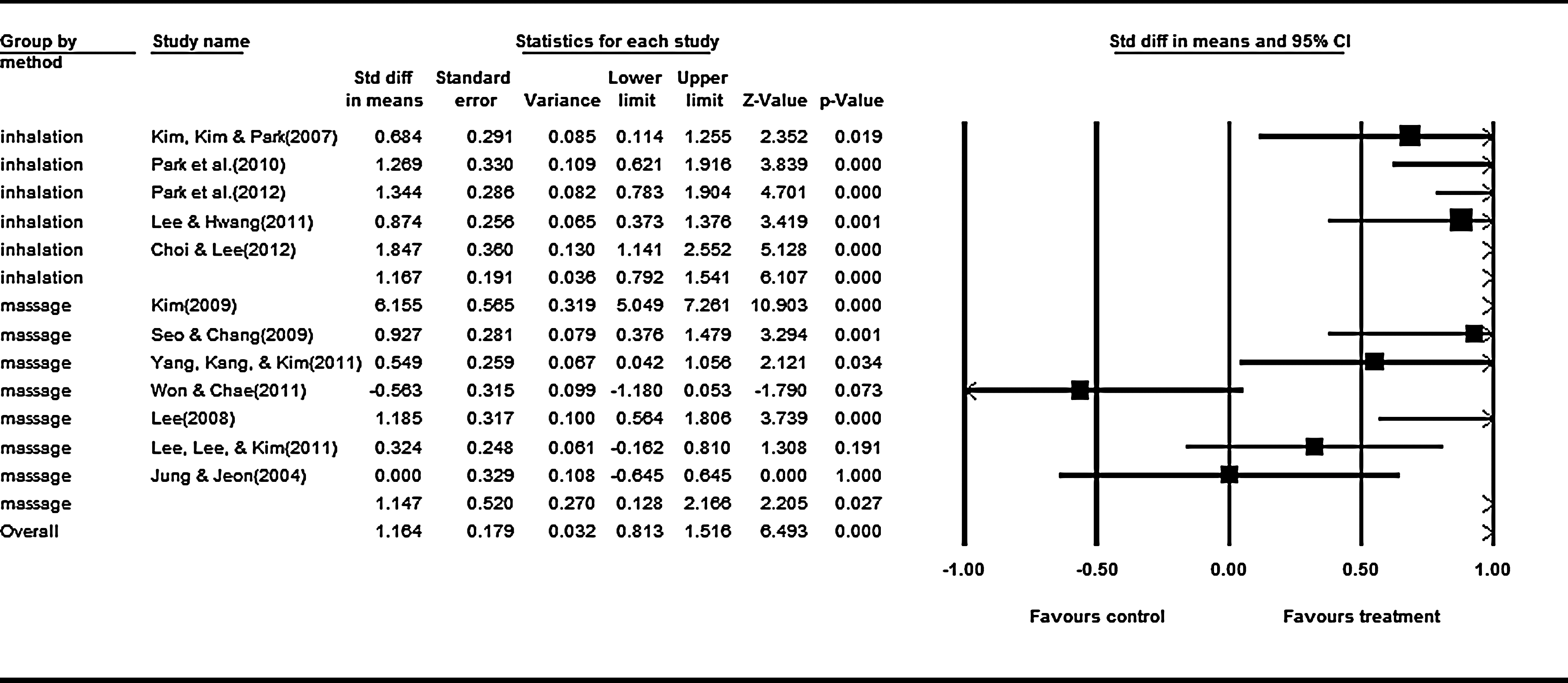
Effect size of aromatherapy according to the condition. Subgroup healthy: heterogeneity: tau 2 =4.18, Q=71.38, df=2 (p<0.001), I2 =97.20%. Test for overall effect size: Z=2.29, p=0.022. Subgroup unhealthy: heterogeneity: tau 2 =0.34, Q=38.83, df=8 (p<0.001), I2 =79.40%. Test for overall effect size: Z=3.10, p=0.002. Total heterogeneity: tau 2 =1.03; Q=134.77, df=11 (p<0.001), I2 =91.84%. Test for overall effect size Z=3.72, p<0.001.
Publication bias
Evaluation of the results of both a funnel plot and Egger test (p=0.008) indicated that there was publication bias.
Discussion
Because of the emphasis on evidence-based clinical practice, the current study was conducted to validate existing data on the effects of aromatherapy on sleep improvement. Accordingly, study trend and effect size of interventions were analyzed for studies that used aromatherapy for sleep improvement in Korean nursing research. Thirteen studies conducted primarily within the past 5 years were selected for inclusion in the study. According to the results of domestic research trend analysis regarding sleep disorders, 20 the number of relevant papers on the topic doubled between 2005 and 2009 to 103 from 55 during between 1990 and 1999. The increase in studies conducted on sleep improvement provided evidence that interest in sleep disorders increased, which was consistent with the current results. With regard to the participants in the selected papers, the percentage of studies in adults and the elderly, individuals with chronic or other diseases, and inpatients was consistent with previous reports. 21 The reported results are most likely explained by the fact that the lack of sleep not only affects the gastrointestinal system and joints but also may trigger muscular pain and influence the balance of physiologic and mental aspects, such as fatigue, anxiety, and tension. 22,23 Therefore, more participants with disease required measures to improve sleep when compared with healthy participants.
Regarding study design, the number of pre/post experimental group studies with a control group was highest, followed by randomized controlled trials and cohort studies, respectively. Although the number of clinical studies has gradually increased, several cross-sectional studies or observational surveys have provided a low level of evidence. Expansion of evidence-based clinical practices using randomized controlled trials or cohort studies with strong evidential power is necessary to improve sleep for those with a sleep disorder. In terms of measurement tools, a majority of the studies evaluated aromatherapy effects by using validated tools. However, concepts such as the quality of sleep or type of sleep disorder were not obvious, and therefore cautious interpretation of the results was required.
The most common aroma oils used for sleep intervention were lavender and bergamot. Most studies used lavender alone or mixtures of lavender and other oils, which was consistent with prior results of research trends in domestic nursing. 24 Analysis of the effects of different aroma oils was difficult because the number of papers on the topic was small, and some studies also measured the effects of aromatherapy on depression or anxiety. Nonetheless, the effects of lavender, cypress, and chamomile, 25 the oils most widely used for sleep disorders, were verified. Following a systematic literature review on aroma massages, 26 Lee reported that massaging both hands with a mixture of lavender and other oils, with jojoba oil as the base, was effective; treatment effects of lavender oil and its effects need to be verified by applying it to diverse patient groups.
Analysis of the effect size of aromatherapy on sleep indicated that aromatherapy significantly enhanced sleep. The effect size of aromatherapy on sleep was smaller than the effect size on anxiety (6.03), depression (5.11), and stress (5.29) but was larger than the effect size (1.97) on pain. 21,27 Thus, aromatherapy had a moderate effect on sleep, which was greater than its effect on the alleviation of physical symptoms, but smaller than its effects on psychological and mental factors. Further, the effect size of aromatherapy was smaller than the effect size (4.24) of music therapy 28 but greater than the effect size (0.47) of exercise therapy. 29
Among the aroma application methods, massage was the most frequently used, followed by direct inhalation and indirect inhalation, which was in accord with previously reported results. 27 A report also indicated that inhalation of lavender was the simplest and that its delivery to the osphresiometer was the quickest through respiration. 25 In a meta-analysis on the intervention factors of aromatherapy application methods and participants' health conditions, the inhalation method had a larger effect size than did massage. This was in contrast to study results reported by Roh and Park, 21 who applied aromatherapy as an intervention for depression or anxiety and indicated the effect size was larger in the massage group than in the inhalation group. It was interpreted that sleep improvement was increased by sustainable effect maintenance by indirect inhalation, unlike other interventions on psychological and mental factors. Results of the analysis regarding the participants in whom aromatherapy was used indicated that the effect size was larger in diseased than in healthy individuals, which was in accord with previous results. 21
A systematic literature review on insomnia and complementary and alternative medicine 30 revealed that acupuncture, tai chi therapy, and yoga were very effective for improving sleep. However, aromatherapy was not included in the analysis because it did not meet selection criteria. The implication was that methodologic problems, including adequate numbers of participants, experimental design, and experimental interventions existed, further verifying that specific and systematic study design and analyses are required in order to examine the effects of aromatherapy on sleep improvement.
Conclusion
These results indicated that additional research on the types of aromas, intervention time, and intervention period are necessary to analyze the effect size of aromatherapy. As well, the effects of aromatherapy on sleep improvement must be verified by measuring physiologic indicators using methods such as polysomnography.
Footnotes
Acknowledgments
The research was supported by Basic Science Research Program through the National Research Foundation of Korea funded by the Ministry of Science, ICT, and Future Planning (2012-0961).
Author Disclosure Statement
No relevant financial relationships exist.