
Abstract
Background:
This study is an attempt to document the medicinal plants used by the tribal community of Little Nicobar Island. Despite modern healthcare facilities, tribals often consume medicinal herbs, with traditional knowledge practitioners (TKPs) serving as local medical experts.
Objectives:
The aim is to conduct an ethnomedicinal survey among the Nicobarese, whose medicinal practices are yet to be documented.
Methods:
Field research was conducted in all five villages of Little Nicobar Island, situated in the southernmost part of the Andaman and Nicobar Archipelago, during 2012–2013. Seven TKPs were interviewed using a questionnaire-guided ethnomedicinal survey protocol. The data obtained were analyzed using the informant consensus factor (ICF) and use value. Voucher specimens of all the cited plant species were deposited at the Regional Medical Research Centre (Indian Council of Medical Research), Port Blair.
Results:
Uses of 34 medicinal plant species, belonging to 23 families encompassing 32 genera, were recorded during the survey. These 34 species are employed to treat a total of 16 ailments. The highest ICF (1.00) was obtained for respiratory diseases. The Euphorbiaceae family exhibited the highest number of citations, and plants with the highest use values were Glochidion calocarpum Kurz, Senna occidentalis (L.) Link, Ocimum tenuiflorum L., and Passiflora suberosa L. Of the medicinal plants reported, the most common growth form was herbs. Remedies were generally prepared using water. The medicinal plant preparations were administered topically or orally.
Interpretation and conclusions:
Traditional knowledge of herbal medicines is handed down orally through generations. These plants attained a significant role under the healthcare of the Nicobarese residing in Little Nicobar Island. Efforts to ensure their documentation are necessary in order to prevent its loss, either because of natural calamities or lack of interest among younger generations in carrying out their tradition.
Introduction
I
The Nicobarese are the inhabitants of the Nicobar group of islands of the Andaman and Nicobar Archipelago, situated in the Bay of Bengal between 6° and 14°N latitude and 92° and 94°E longitude. The Nicobar group is divided into three zones: the northern zone consisting of Car Nicobar Island, the central zone consisting of the Nancowry group of Islands, and the southern zone consisting of Great and Little Nicobar Islands. 10
Nicobarese are aboriginal inhabitants of the Nicobar group of islands and belong to the mongoloid race, who have a short stature and stout and tough muscular bodies. Their faces, with scanty beards, have thick lips and small broad and flat noses. 11 They are coastal dwellers enjoying the vicinity of exuberant and verdant tropical forests. The people of Little Nicobar still have their customary way of life, while the traditions of the Car Nicobar and Nancowry group of islands are on the verge of decline due to their exposure to modern amenities. Thus, Little Nicobar Island is treasured with an emporium of ethnobotanical wealth. Therefore, the study aimed to document the indigenous knowledge of medicinal plants and healthcare practices among the Nicobarese of Little Nicobar.
Materials and Methods
Little Nicobar Island (study area) includes five villages: Pillow, Pilobaha, Pilopanja, Pilopatia, and Makachuwa (Fig. 1). The traditional medicinal practices of the Nicobarese belonging to Little Nicobar Island have not been documented so far. This island is isolated, and dugont canoes are the only means of transport from village to village. A study was conducted on this island regarding the use of plants in folk medicine by local Nicobarese. The people of this island speak Nicobarese language written in Roman script.
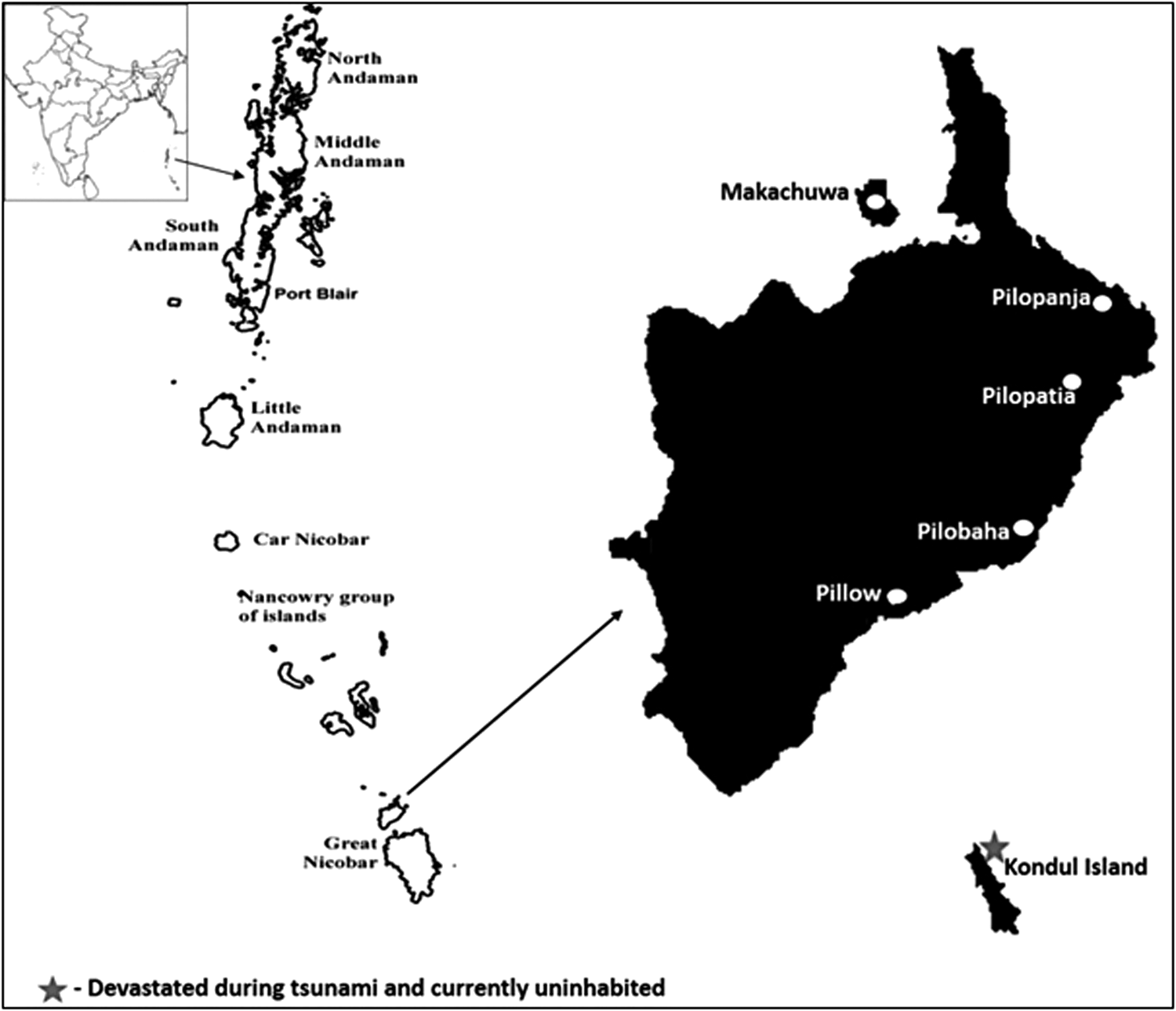
Little Nicobar Island (study area).
Field visits were carried out in all the inhabited villages of the Little Nicobar Islands during 2012–2013, after obtaining prior permission from local authorities. The survey identified the traditional knowledge practitioners (TKPs) of each village. Each TKP was interviewed individually with the help of a semistructured questionnaire. 12,13 The interview included the diseases that he/she has been treating, medicinal plants used, their mode of preparation, their usage and dosage, and so on. The plants were collected in and around villages with the help of TKPs. Photographs of plant specimen, GPS locations, and other botanical field notes were recorded. Taxonomic identification of specimens was done at the Botanical Survey of India, Andaman & Nicobar Circle, Port Blair. Voucher specimens were deposited at the Medicinal Plant Department, Regional Medical Research Centre (Indian Council of Medical Research), Port Blair. Data were tabulated and analyzed using two quantitative ethnobotanical methods: use value and informant consensus factor (ICF).
The use value was calculated using the formula proposed by Ritter et al. 14 To calculate the use value of a species for a TKP (UVis), the formula UVis=Usi/n was used, where Usi is the number of plant uses mentioned by the TKPs for the species, and n is the number of interviews with the TKP. To calculate the use value of each species (UVs), the formula UVs=UVis/n was used, where UVis equals the use value of a species for an informant, and n is the total number of TKPs.
To calculate the ICF, the cited species were grouped into six categories of medicinal uses based on the diseases reported by the TKPs: treatment of respiratory diseases (cough and breathing difficulty), general aches and pains (body ache and headache), skin infections and injuries (cuts, wounds, and pruritus), gastrointestinal (anorexia, jaundice, and abdomen pain) infections and infestations (fever, common cold, and tuberculosis), and miscellaneous (paralysis, prolonged labor, and nourishment). The ICF was calculated using the formula ICF=(Nur−Nt)/(Nur−1), where Nur represents the number of citations in each use category, and Nt represents the number of species cited. 15
Results
A total of seven (two men and five women) TKPs were identified, representing the population across five villages. TKPs reported 34 plant species belonging to 23 families and 32 genera useful in ethnomedicinal preparations. The largest number of plant species comes from Euphorbiaceae family (four species), followed by Moraceae (three species), and the remaining families were represented by one or two species each.
The species with greater use values were “In yőyő” (Glochidion calocarpum Kurz; UVs=0.71), “Phithangri” (Senna occidentalis (L.) Link; UVs=0.71), “Kisinesi” (Ocimum tenuiflorum L.; UVs=0.57), and “Kūőng” (Passiflora suberosa L.; UVs=0.57). Study results are presented in alphabetical order of plant names, with their respective scientific name, family, local name, UVs, therapeutic usage, and plant parts used for ethnomedicinal preparation (Table 1).
UVis, use value of a species for a traditional knowledge practitioner; UVs, use value of each species.
The study of the growth form of medicinal plants revealed that herbs made up the highest proportion of medicinal plants, representing 12 (35%) species, followed by shrubs representing 10 species (29%), trees representing 8 species (26%), and climbers representing 4 species (12%) (Fig. 2).
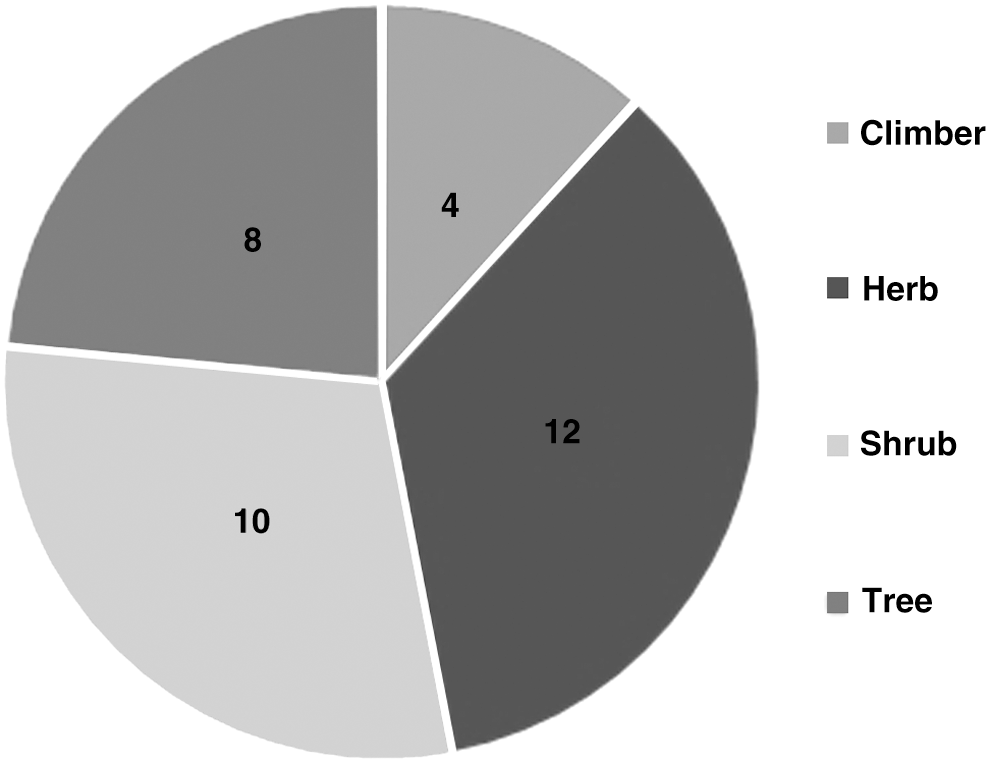
Growth habits of the reported medicinal plant species.
This study recorded that leaf parts of plant species were alone used as medicines. Remedies were generally prepared using water and coconut oil as the excipient, but occasionally remedies were prepared with other excipients, including coconut milk, pig blood, and pig ghee (fat). Some remedies were used directly. The medicinal preparations were either administered by oral route or applied topically. Topical preparations were the most common.
Thirty-four plant species were used by TKPs for 16 different ailments and grouped into 6 categories of use. The highest ICF values, 1.00 and 0.56, were obtained for respiratory diseases (1 species and 3 reports of use) and general aches and pains (9 species and 16 reports). A low ICF value was obtained for the miscellaneous category (8 species and 9 reports of use) (Table 2).
The Miscellaneous category included paralysis, prolonged labor, and nourishment.
ICF, informant consensus factor.
Discussion
The Nicobarese are a reservoir of vast knowledge in terms of their surrounding flora. They have been using medicinal plants for treatment of various ailments since ancient times. As observed in most traditional practices in India and all over the world, 16 –18 the Nicobarese also handed over their traditional healing knowledge from the older to the younger generation in the family through oral narrations and informal training, imparted while working as helpers to folk healers. 19 After the catastrophic Tsunami in 2004 the Kondul Island was devastated, and during the survey period it was found uninhabitable. The traditional practices of this island were never documented. Thus, it is necessary to document and conserve the valuable traditional knowledge of these people.
In the present study, the most highly cited species were members of the Euphorbiaceae family. This family is also reported in ethnobotanical surveys conducted in other regions of India. 20 –22
To identify the important use categories for the population studied, the ICF was calculated. Respiratory diseases (1.00) and general aches and pains (0.57) exhibited the highest ICF values. Main conditions included in categories with higher ICF values were cough, breathing difficulty, abdomen pain, headache, and body ache. These types of illnesses and clinical signs are common and hence easily identified by TKPs, which may explain why these categories exhibited the largest ICF values.
The use value is a quantitative estimate that demonstrates the relative importance of plant species and family for a population. This index was calculated to establish a relationship between the plant species and its uses by analyzing the index in relation to use categories. The species with highest use value (Glochidion calocarpum Kurz, Senna occidentalis (L.) Link, Ocimum tenuiflorum L., and Passiflora suberosa L.) were indicated for treatment of diseases or clinical signs of the category with highest ICF. This finding reinforces the idea that these species are most important for the population studied and that the TKPs share knowledge about practices and plants used in their healthcare practices on Little Nicobar Island.
The usage of a particular plant species to cure disease varies from one practitioner to another, even within the same village. Interestingly, the same medicinal plant is often used by village practitioners for treating various diseases. For example, Glochidion calocarpum Kurz. and Senna occidentalis (L.) Link are used in medicinal preparations to cure three ailments. Glochidion calocarpum Kurz. is endemic in the Nicobar group of islands and used as a cure for headache, skin injuries, and prolonged labor.
Most remedies are prepared from leaf extracts, and use of excipient is a common practice among tribes. Water and coconut oil are common excipients used by the Nicobarese due to their availability. However, water is more commonly used, as most of the active components are highly soluble in it. Similar observations have been recorded among the Kalanguya tribe. 23 Coconut plantation being the major livelihood of the Nicobarese, coconut oil is used in large quantities for medicinal preparation, especially for topical application. Other excipient materials such as coconut milk, pig blood, and pig ghee are also used when needed.
If timely efforts are not taken, the wealth of undocumented information that exists among the Nicobarese of this island is likely to be lost, as happened with the people of Kondul Island. Although a few species listed are already known for their medicinal use, some of them are new. This survey has led to identify the useful flora in Little Nicobar Island, enabling the researchers to come closer to the community and create awareness among them.
Conclusions
The Nicobarese of Little Nicobar Island use medicinal plants to treat different ailments. The present study is a detailed survey covering all villages of the island, carried out with proper documentation. Generating information from the community and documenting it helps not only in preventing the loss of knowledge but also to carry out further research, thus developing a unified knowledge for a better future.
Footnotes
Acknowledgments
The authors acknowledge the Indian Council of Medical Research (ICMR), New Delhi, India, for providing a financial grant for the study (Project No. Tribal/43/2008-ECD-II). The authors are grateful to Shri. P. Jawahar, I.A.S., deputy commissioner, Nicobar District, Andaman & Nicobar Islands, for permission and extensive support during the visits. The authors are thankful to Shri. N.N. Mehrotra, retired scientist, CDRI, Lucknow, for his valuable suggestions. The authors are grateful to the Tribal Council, village captains, and traditional knowledge providers of Little Nicobar of Andaman & Nicobar Islands for providing their valuable ethnomedicine information and cooperation, without which this work would not have been possible. The authors are also thankful to the Botanical Survey of India, Port Blair, for their help in identification of plant specimens.
Author Disclosure Statement
No competing financial interests exist.