
Abstract
Objectives:
To evaluate the role of herbal medicine in drug-induced parkinsonism (DIP) and identify an optimal treatment approach.
Design:
Retrospective review of DIP cases treated with herbal medicine.
Settings/Location:
The Parkinson's clinic at Kyung Hee Traditional Korean Medicine Hospital, Korea.
Patients:
Twenty-one patients whose clinical outcome and offending drug could be identified.
Outcome measures:
Clinical features, treatments, and outcomes and summarized the clinical course and treatment in each case.
Results:
Twelve patients had levosulpiride-induced parkinsonism and 9 had parkinsonism induced by another drug. The offending drugs were discontinued in all patients, and all patients received herbal medications during treatment. Nine of 12 patients with parkinsonism from levosulpiride and 4 of 9 patients with parkinsonism from other drugs had complete reversal of symptoms. The most frequently used herbal formula was Ukgansan (Yigansan). DIP in the levosulpiride group tended to improve faster with herbal medicine, and the percentage of improvement was higher.
Conclusions:
Optimal herbal medicine treatments chosen after a careful history and evaluation for risk factors may be helpful in reversing DIP.
Introduction
A
The known risk factors for DIP are potency and dosage of the causative drugs and individual susceptibility. 5,6 Drugs commonly implicated are typical neuroleptics, antiemetics, calcium channel agents, and atypical neuroleptics. 7 Individual risk factors are older age, female sex, and presence of cerebral atrophy. 8 However, many of the drugs that can cause DIP are being used more often in younger people and more widely for a broader range of indications than ever before. The mechanisms of DIP have been identified as diminished dopamine D2-receptor stimulation in the striatum, blockade of dopamine receptors, increased intracellular monoamine oxidase–mediated metabolism of dopamine, and increased glutathione levels. 1 The delay between drug exposure and onset of parkinsonism varies widely, ranging from a few days to several months. 2,9
DIP is generally thought to be reversible after stopping the offending drug. In most cases, symptoms subside within 4 months, but in some cases they may last from 6 to 18 months. 3,10 Up to 20% of patients with DIP develop a persistent deficit despite drug withdrawal. 1 Management for symptom relief in DIP with anticholinergic agents or dopaminergic drugs may have additional adverse effects, especially in the elderly. 11
Because of the limitations of conventional therapies, many patients with parkinsonism have chosen complementary and alternative medicines for controlling a variety of symptoms, including dyskinesia and autonomic disorder. 12,13 Although several studies have assessed the effects of herbal medicine on parkinsonism, studies of herbal medicine for DIP have not been reported. Review of clinical cases of DIP managed with herbal medicine is needed. This study sought to investigate whether herbal medicine helped patients with DIP.
Materials and Methods
Information on 62 consecutive patients with DIP
1
was extracted from the database of Kyung Hee University Korean Medical Center from January 2010 to June 2012 (18 months). Patients who met the following criteria were included: 1. The drug history of the patient was identified in medical records. 2. No history of extrapyramidal disorders before the use of the offending drug. 3. The patient's clinical symptoms, medical history, and laboratory examinations, including brain images, were evaluated by a neurologist. 4. The clinical outcomes could be assessed by the last follow-up session. The outcome of DIP was categorized as “completely reversible DIP,” “incompletely reversible DIP,” and “irreversible DIP” on the basis of clinical data. In completely reversible DIP, all parkinsonian symptoms completely disappeared. In incompletely reversible DIP, over 50% of symptoms partially disappeared; in irreversible DIP, over 50% of symptoms persisted or symptoms did not improve at all.
Of the original 62 patients, 41 patients were excluded. In 30 cases, it was impossible to assess outcomes because the follow-up period was too short (<1 month). For the other 11 patients, exact medication information was unavailable, and changes in symptoms were checked only during follow-up. From this, it was determined that 3 patients had irreversible DIP, 2 had incompletely reversible DIP, and 5 were completely reversible. One patient had a history of previous extrapyramidal disorders.
Hence, 21 patients were included for analysis in the present study. Levosulpiride-induced parkinsonism is common and has been reported separately in recent studies. 14 Therefore, the 21 patients in this study were classified into 2 groups: those with levosulpiride-induced parkinsonism and those with parkinsonism induced by other drugs (Fig. 1).
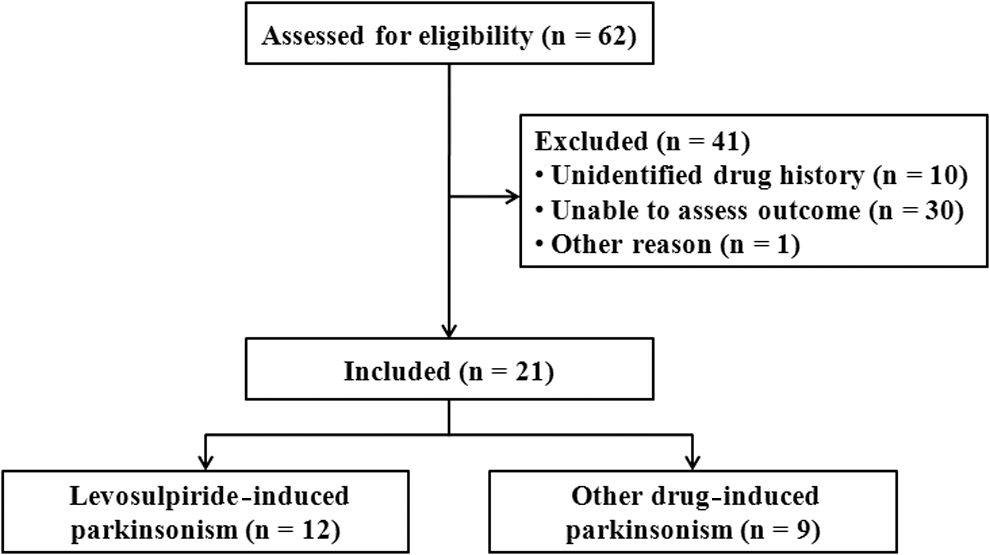
Flowchart for patient inclusion. The study included 21 patients with drug-induced parkinsonism, 12 patients with levosulpiride-induced parkinsonism, and 9 with parkinsonism with another drug.
Clinical features of patients in each group were evaluated, including age, sex, history of illness, medications, onset and duration of symptoms, Hoehn and Yahr stage, and clinical outcomes. In addition, the herbal medicine used for each of the 21 patients, including the frequency of use, was determined. Analysis of the results was purely descriptive. Age, time of onset, and duration of follow-up are expressed as mean±standard deviation and range.
Results
Clinical characteristics of DIP cases
Among the 21 patients with DIP, 12 had levosulpiride-induced parkinsonism and 9 had parkinsonism caused by a variety of drugs not including levosulpiride. The clinical characteristics of each group are summarized in Table 1. The mean age at the time of diagnosis was over 70 years in both groups, and almost all patients were older than age 60 years. DIP was more frequent in women. The delay between drug exposure and symptom onset varied widely, ranging from 15 days to 48 months. The duration of DIP ranged from 10 days to 18 months. Twenty of 21 patients were rated as having Hoehn and Yahr stages 1 to 3, indicating that DIP was of mild to moderate severity in most patients (Table 1).
SD, standard deviation.
The frequently reported symptoms in both groups were orolingual abnormal movements (67%), tremor of upper extremities (52%), gait disturbance (28%), and dysarthria (19%). The tremor types were diverse, including resting tremors as well as postural and action tremors. Seven patients had symmetric tremors and 5 had asymmetric tremors (Table 1 –3).
Herbal prescriptions of major treatment: Korean (Chinese).
DO, delay of occurrence; DS, duration of symptoms; F, female; GERD, gastroesophageal reflux disease; IVD, intervertebral disorders; M, male; mo, month.
Herbal prescriptions of major treatment: Korean (Chinese).
The drugs that were thought to be the most likely cause.
Levosulpiride-induced parkinsonism
DIP was completely reversible in 9 (75.0%) patients after discontinuation of levosulpiride and administration of herbal medicines. Symptoms disappeared after a mean 1.9 months (range, 10 days–4.7 months). Patient L4 did not show any change of symptoms after 2 months of treatment. Patient L5 showed reversible change in a steady curve over 3 months of follow-up, but after that time the patient was no longer seen in the clinic. In patient L9, 30% of the symptoms persisted until 12 months after discontinuation of levosulpiride and initiation of herbal treatments (Table 2).
DIP from other drugs
Many patients in this group (patients O1–O9) experienced insomnia and depression and were taking multiple antianxiety medications and/or antidepressants. The drugs thought to be the most likely cause are noted in Table 3. The symptoms observed were similar to those of levosulpiride-induced parkinsonism. Four cases (44.4%) of DIP were completely reversible after the discontinuation of the offending drugs and administration of herbal medicines. Symptoms disappeared after a mean of 1.1 months (range, 12 days to 2 months). In 3 of 5 cases that were not completely reversible, haloperidol was assumed to be the cause. 15 Patient O4 had not improved after 3 months, and patient O7 had a recurrence of jaw tremor after resuming haloperidol therapy for insomnia (Table 3).
Herbal prescriptions used for management of DIP
The 21 patients included in the study were treated with 13 types of herbal prescriptions, as detailed in Table 4. Most of the herbal prescriptions were used as dry extract, and the most frequently used formula was Ukgansan (Yigansan, 14 patients). Chyeugansoyosan (Qingganxiaoyaosan) was used in 4 patients.
Herbal prescriptions: Korean (Chinese).
The 13 herbal prescriptions contained a total of 54 medicinal herbs. The most frequently used herbs were Poria species (in 8 prescriptions), Glycyrrhizae radix (in 8), Atractylodis rhizoma Alba (in 7), Citri pericarpium (in 7), Magnoliae cortex (in 6), Zingiberis rhizoma (in 6), Angelica radix (in 5), Cyperi rhizoma (in 5), and Ginseng radix (in 5). There were 37 other herbs that were involved in only 1 prescription each (Table 4).
Discussion
The results of this study indicated that patients had a more favorable outcome than those analyzed in previous studies. In the levosulpiride-induced parkinsonism group, the patients who received herbal medicine tended to improve faster and the percentage of improvement was higher compared with the 2009 results from the Asan Medical Center. 14 In a study by Shin and colleagues, the symptoms subsided completely in half of the patients with levosulpiride-induced parkinsonism after levosulpiride was discontinued, but the other half had symptoms that persisted over a year. 14 This could indicate that herbal medicine may be helpful in recovery from DIP, especially in cases of levosulpiride-induced parkinsonism.
Still, 3 of 12 patients in the levosulpiride group and 5 of 9 in the other group had irreversible or incompletely reversible DIP. One explanation may be that the offending drugs aggravated a preexisting subclinical nigrostriatal defect and unmasked underlying PD. In addition, some patients had follow-up periods insufficient for determination of a final outcome; every DIP patient should be observed for at least 6 months. Finally, the effects of long-term use of haloperidol, a typical neuroleptic with potent dopamine D2 receptor–blocking actions, may be difficult to completely reverse in elderly patients, as was observed in patients O4, O7, and O9.
An optimal approach with herbal medicines, which have relatively fewer adverse effects and wide applications in symptom control, can be reasonable for DIP. Conventional drugs have limitations for relief of DIP, particularly in the elderly. 16 Anticholinergic agents should be avoided in the elderly because of such adverse effects as urinary retention, exacerbation of cognitive impairment, and precipitation of angle closure glaucoma. 11,17 Moreover, amantadine is generally not well tolerated by older patients. 11 Furthermore, in the current study, symptoms in patients O4 and O6 worsened after administration of such antiparkinson agents as benztropine and levodopa.
More than half of the patients in this study had levosulpiride-induced parkinsonism. In 8 of 12 cases, the patients were taking levosulpiride for dyspepsia caused by complications of nonsteroidal anti-inflammatory drugs that were used for pain control for degenerative arthritis or vertebral spondylosis. Levosulpiride, a substituted benzamide that exerts antidopaminergic activity on both the central nervous system and gastrointestinal tract, is prescribed for dyspepsia, gastroesophageal reflux disease, and emesis in many countries in Europe and Asia. 14 Prescriptions of levosulpiride for dyspepsia control have been popular in Korea. The National Health Insurance Corporation in Korea reported 7,937,000 levosulpiride prescriptions during 2007. Unfortunately, levosulpiride can cause movement disorders, such as parkinsonism and tremor. 14
The current results indicate that levosulpiride, and not only antidopaminergic neuroleptics, can be a leading cause of DIP in elderly patient populations. Seven patients had parkinsonism due to anxiolytics and antidepressants for senile depression, anxiety, or insomnia. The patients were likely to be using multiple medications, and it was difficult to confirm the offending drug in some of the cases of DIP. Polypharmacy may influence the development of adverse drug reactions in such cases. 18
Several kinds of herbal treatments were used for management of DIP in our study. Ukgansan (Yigansan) has been the most frequently used herbal medicine in neurodegenerative disorders. Ukgansan (Yigansan) has shown positive effects on PD in experimental and clinical studies. It has been reported that Ukgansan (Yigansan) has neuroprotective effects and rescues dopaminergic neurons from 1-methyl-4-phenylpyridine/1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MTPT) toxicity, possibly via the PI3K/Akt pathway. 19 Ukgansan (Yigansan) is also effective against neuroleptic-induced dyskinesia in patients with schizophrenia. 20 Moreover, it was reported that Ukgansan (Yigansan) was effective to control extrapyramidal symptoms in senile patients with Lewy body disease, especially dyskinesia. 21 Ukgansan (Yigansan) also affects age-related anxiety, enhancing serotonergic and dopaminergic transmission. 22 Thus, we could assume that Ukgansan (Yigansan) also would be effective against DIP in our cases.
There is some evidence of the effectiveness of Dangguijakyaksan (Danguishuoyaosan). It has neuroprotective effects in dopaminergic neurons against 6-hydroxydopamine (6-OHDA)–induced toxicity through antioxidant and anti–mitochondrial-mediated apoptotic activities. 23 Dangguijakyaksan (Danguishuoyaosan) showed behavior recovery and dopamine neuron protection against MPTP-induced toxicity via antiapoptotic activities. 24 Regarding individual herbal plants, there have been several reports of effects in parkinsonism models. Paeoniflorin, the major active component of Paeoniae radix Alba, attenuated neuroinflammation and dopaminergic neurodegeneration in the MPTP model of PD by activation of an adenosine A1 receptor. 25 Uncaria rhynchophylla Hook possesses neuroprotective activity on dopaminergic neurons against 6-OHDA–induced toxicity through antioxidative and antiapoptotic activities in PD models. 26 Angelica gigas Radix has neuroprotective effects by its anti-inflammatory activities. 27 The mechanisms of other herbal drugs in the Parkinson model remain unknown, and further study is needed to clarify the mechanisms and demonstrate the effects of herbal medicines for DIP.
DIP has a variety of symptoms that can affect patients' overall quality of life; therefore, supporting rapid resolution of symptoms is important. In this respect, optimal treatments with active herbal medications may be more helpful than observation alone in reversing DIP after cessation of the offending drug. In addition, clinicians should always check medication histories in order to minimize the risk of DIP.
This is the first retrospective study to explore an optimal treatment approach for DIP using herbal medicine. However, there are several limitations. The study investigated medical records from an 18-month period, but many patients were not included because of various reasons; thus, the number of cases is small. Moreover, the possibility that the patients who experienced improvement were more likely to visit the clinic consistently could not be excluded.
In conclusion, the present study assessed 21 cases of DIP treated with herbal medicine. The results of this study supported that optimal herbal medicine treatments might be helpful in reversing DIP. This is a small retrospective study but the first report of reversing DIP by using herbal medicine. Further larger, well-controlled studies are needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.