
Abstract
Objective:
Cat's claw (Uncaria tomentosa) is a native Amazon plant that exhibits anti-inflammatory and antitumor properties. We wanted to assess its activity for symptom management of terminal cancer patients.
Methods:
This prospective phase II study assessed the effects of a 100-mg dose of a dry extract of U. tomentosa three times per day in patients with advanced solid tumors who had no further therapeutic options and a life expectancy of at least 2 months. The European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ C30) and Functional Assessment of Chronic Illness Therapy - Fatigue questionnaires were used to assess the participants' quality of life, the Hospital Anxiety and Depression Scale questionnaire was used to assess anxiety and depression, and the Pittsburgh Sleep Quality Index was used to assess sleep quality. In addition, several biochemical and inflammatory parameters were analyzed.
Results:
Fifty-one volunteers were recruited. Their median age was 64 (range, 33–85) years, and 47% of patients were female. More than 65% of patients had scores on the Karnofsky Performance Scale of 80% or less. Treatment improved the patients' overall quality of life (p=0.0411) and social functioning (p=0.0341), as assessed by the EORTC QLQ C-30, and reduced fatigue (p=0.0496) according to the Chalder Fatigue Questionnaire. None of the biochemical or inflammatory parameters assessed (interleukin-1 and -6, C-reactive protein, tumor necrosis factor-α, erythrocyte sedimentation rate, and α-1-acid glycoprotein) changed significantly. No tumor response was detected according to the Response Evaluation Criteria In Solid Tumors; however, the disease stabilized for more than 8 months in four participants. The medication was well tolerated by most patients.
Conclusion:
Use of cat's claw might be beneficial in patients with advanced cancer by improving their quality of life and reducing fatigue. The mechanism of action does not seem to be related to the anti-inflammatory properties of this plant.
Introduction
U
U. tomentosa was used as a medicinal plant by the ancient Incas, who conveyed their knowledge to other Peruvian natives. It has been used ever since for the treatment of several diseases, such as osteoarthritis, cancer, viral infections, gastric ulcers, and menstrual disorders. 1
U. tomentosa contains a variety of bioactive secondary metabolites, including tetra- and pentacyclic oxindole alkaloids (POAs), glycosides, polyoxygenated triterpenes, and procyanidins. 2,3 Most investigators attribute the biological effects of this plant to the POAs, an assumption that has been corroborated by studies of several such alkaloids that indicated their antioxidant, immunomodulatory, and antineoplastic properties. 4
Initially, the POAs were associated with increases in phagocytosis. 5 Later studies described its effective inhibition of growth in leukemia, 6 –8 glioma, neuroblastoma, 9 and medullary thyroid carcinoma cells, 10 partly because of apoptosis induction. Alternatively, the anti-inflammatory and antineoplastic effects of U. tomentosa could be due to its reduction of the expression of transcription factor nuclear factor κ light-chain enhancer of activated B cells (NF-κB), 11,12 an effect that, in turn, regulates the expression of tumor necrosis factor-α (TNF-α). By reducing the expression of NF-κB, U. tomentosa also reduces the TNF-α levels and intensifies its anti-inflammatory action. 11,13
Some studies have shown that other compounds present in U. tomentosa may also be related to its therapeutic actions. For instance, quinovic acid glycosides can inhibit viral infections, 14 and procyanidins exhibit antioxidant, anti-inflammatory, and antiviral properties. 15 Furthermore, some extracts and fractions of U. tomentosa exhibit a substantial antimutagenic protective action, which is associated with its antioxidant potential. 16,17 The pharmacologic activity of this plant might also be derived from the synergic action of its various components.
The aim of the present study was to assess the efficacy and safety of a dry extract of U. tomentosa on individuals who had solid tumors with no further therapeutic options. This study also investigated the possible correlation between the extract's clinical effects and changes in inflammatory parameters.
Materials and Methods
Study design
The design was a prospective, single-center, open-label phase II study. The sample set was designed to include 50 individuals with solid tumors who had no further therapeutic options according to the combined assessment of the patient's attending physician and the investigator. The recruitment and clinical follow-up of the patients were conducted at the School of Medicine of the ABC Foundation-associated hospitals. The trial is registered with ClinicalTrials.gov (NCT02045719).
Inclusion and exclusion criteria
The study included individuals 18 years of age and older who had solid tumors and no other curative therapeutic options (as established by their attending physician). Included patients also had expected life expectancy of at least 2 months, creatinine levels up to twice the upper limit of normal (ULN), alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels up to twice the ULN, and direct bilirubin levels up to 1.5 times the ULN. In patients with pre-existing liver disease, the ALT, AST, and direct bilirubin levels could be up to 2.5 times the ULN. To assess the tumor response, the participants' diseases had to be measurable according to Response Evaluation Criteria In Solid Tumors (RECIST). 18
The study was approved by the Faculdade de Medicina da Fundação ABC Ethics Committee (the institutional review board).
The study excluded pregnant and breastfeeding women, as well as individuals receiving chemotherapy or other tumor-targeting antineoplastic treatments, except for antalgic radiotherapy. Also excluded were individuals with severe kidney or liver failure or known hypersensitivity to the components of the medication used, as well as those with a history of emotional disorders that could interfere with the data collection.
The criteria for study discontinuation were as follows: grade III and IV adverse events according to the Common Terminology Criteria for Adverse Events, the need to use prohibited concomitant medication, nonadherence to the treatment (use of less of 80% of the prescribed medication during the study period), protocol violation, the presence of comorbidities, and administrative reasons.
After patients signed the informed consent forms, their clinical histories were thoroughly reviewed and they underwent a complete physical examination. At the same time, biological samples were collected for laboratory tests, which were aimed at identifying any possible disorders that might preclude participation in the study.
The results of a diagnostic imaging test performed within the previous 30 days were required before beginning the medication. The study protocol established five patient visits in addition to the one scheduled for screening. The screening visit occurred 1 week before (T=−1) the first study visit (T=0) and the other visits happened at every 2 weeks up to week 8. Each visit included a clinical interview, a physical examination, application of specific questionnaires, and blood sampling. The quality-of-life questionnaires used were the European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ, C-30, version 3), 19 the Functional Assessment of Chronic Illness Therapy - Fatigue (FACIT-F, version 4), 20 the Hospital Anxiety and Depression Scale (HADS), 21 and the Chalder fatigue scale. 22 The quality of sleep was assessed by using the Brazilian version of the Pittsburgh Sleep Quality Index (PSQI-BR). 23 After 8 weeks of the study, the tumor response was evaluated according to RECIST. 18 Overall survival and progression-free survival were also assessed for all patients at study end in December 2013. Statistical software package Prism, version 6d, was used for all statistical calculations (GraphPad Software, La Jolla, CA).
The blood and biochemical profiles were assessed every 2 weeks to detect signs of kidney or liver toxicity. In cases of measurable disease, imaging tests were performed after the end of the treatment to investigate changes, according to RECIST 1.1. 18 The blood samples were also used to assess the inflammatory parameters interleukin (IL)-1, IL-6, C-reactive protein (CRP), TNF-α, erythrocyte sedimentation rate (ESR), and α-1-acid glycoprotein (see below). At the end of the 8 weeks, the investigator decided which participants would continue in the study or be dismissed on the basis of their RECIST results, tolerance of treatment, and clinical benefits. Toxicities were assessed according to the Common Terminology Criteria for Adverse Events version 4 scale. 24
Medication
The medication given was a dry extract of U. tomentosa (Wild.) DC in 100-mg tablets, which had standardized total alkaloid contents corresponding to 5.0%±0.5% of mitraphylline, as measured by chromatography, and was produced by the Herbarium Laboratory (São Paulo, Brazil). The extract derived from U. tomentosa root bark. The drug regimen consisted of one tablet taken three times per day, every day, as indicated in the package insert. Were the volunteers to miss a dose for any reason, they were instructed not to increase the amount of medication on the following day. When possible adverse effects occurred, drug intake was reduced to twice per day; if the symptoms remained the medication was fully discontinued.
The participants' adherence to treatment was assessed at each visit according to an examination of the returned packages. For that purpose, the participants were instructed at study onset to take the drug packages to all visits, including the empty packages. The packages were sent to the pharmacy, which then provided the medication needed until the following visit.
Laboratory tests
Approximately 20.0 mL of whole blood was collected from all participants at each visit. The sampled blood was distributed among tubes with and without the anticoagulant ethylenediaminetetraacetic acid (EDTA). The tubes containing EDTA were used in a complete blood count using a flow cytometer, ABX Pentra 120 (HORIBA, Kyoto, Japan). The results were confirmed on blood smear slides with Leishman staining. The ESR at 1 hour was assessed by the Wintrobe method. The blood in the tubes without EDTA was used for biochemical tests. The creatinine, AST, ALT, alkaline phosphatase, γ-glutamyl transpeptidase (GGT), and total and fractioned bilirubin levels were assessed by an automated enzymatic-colorimetric analysis obtained from ELItech (Puteaux, France) using a Flexor EL200 spectrophotometer. The TNF-α, IL-1, IL-6, and CRP levels were assessed via a competitive immunoassay obtained from Siemens (Erlangen, Germany) by chemiluminescence reading using an Immulite 1000 luminometer. All tests were performed twice, according to the good practices for clinical tests adopted by the Laboratory of Clinical Tests of the School of Medicine of ABC.
Results
Study population
Fifty individuals were recruited between October 2012 and September 2013. One individual showed no measurable disease. Although his inclusion was a protocol violation, his corresponding data were considered in analysis of demographic characteristics, quality of life, and survival. One additional participant was then included. Therefore, the total sample included 51 participants.
The overall and demographic characteristics of the participants are described in Table 1. The median age was 64 years (range, 33–85 years), the distribution of men and women was almost equal (53% and 47%, respectively), and most patients were white (74.5%). Colon cancer was the most prevalent neoplasm, followed by breast and lung cancers (19.6%, 15.3%, and 13.7%, respectively). Remarkably, the score on the Karnofsky Performance Status Scale was 80% or less for most participants.
Unless otherwise noted, values are the number (percentage) of patients.
KPS, Karnofsky Performance Scale.
Quality of life
During the study, the average overall quality of life (p=0.0411) and social functioning (p=0.0341) improved, as assessed by the EORTC QLQ C-30. Figure 1 shows that fatigue, as assessed by the Chalder scale, also improved (p=0.0496). The remaining symptoms, including insomnia, pain, and lack of appetite, did not improve (data not shown). Body weight did not change significantly throughout the treatment course (Fig. 2A).

Scores for overall health status, physical functioning, role functioning, and social functioning scales of the The European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire during the 8-week treatment period. The p-values correspond to comparisons of the scores before and after treatment. The figure also depicts the scores on the Brazilian version of the Pittsburgh Sleep Quality Index (PSQI-BR), Hospital Anxiety and Depression Scale (HADS), Functional Assessment of Chronic Illness Therapy - Fatigue (FACIT-F), and Chalder fatigue scale. Error bars correspond to 95% confidence intervals; p-values were considered to denote statistically significant differences if less than 0.05.
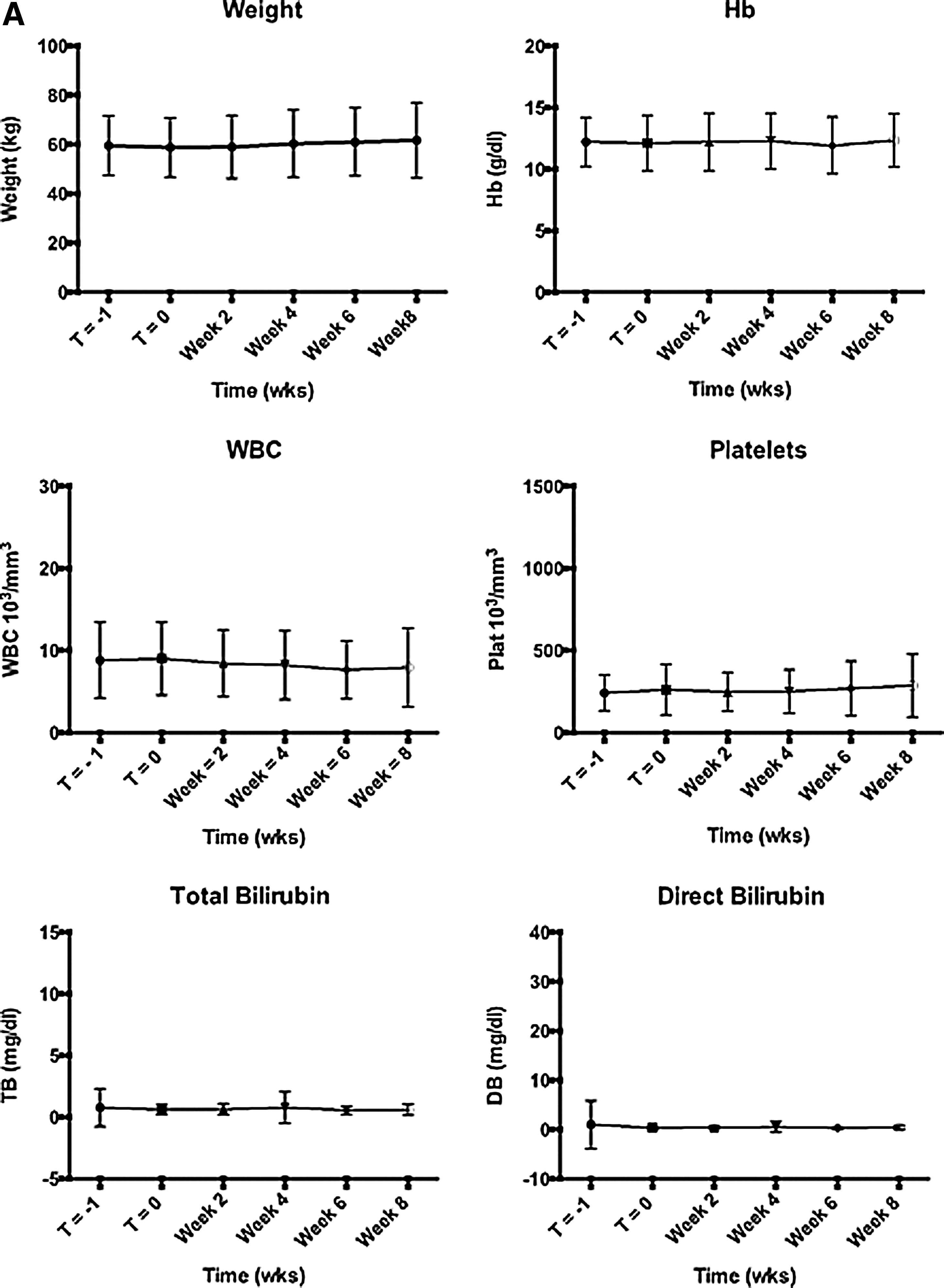
Variation in body weight and blood work results during the 8-week treatment period.
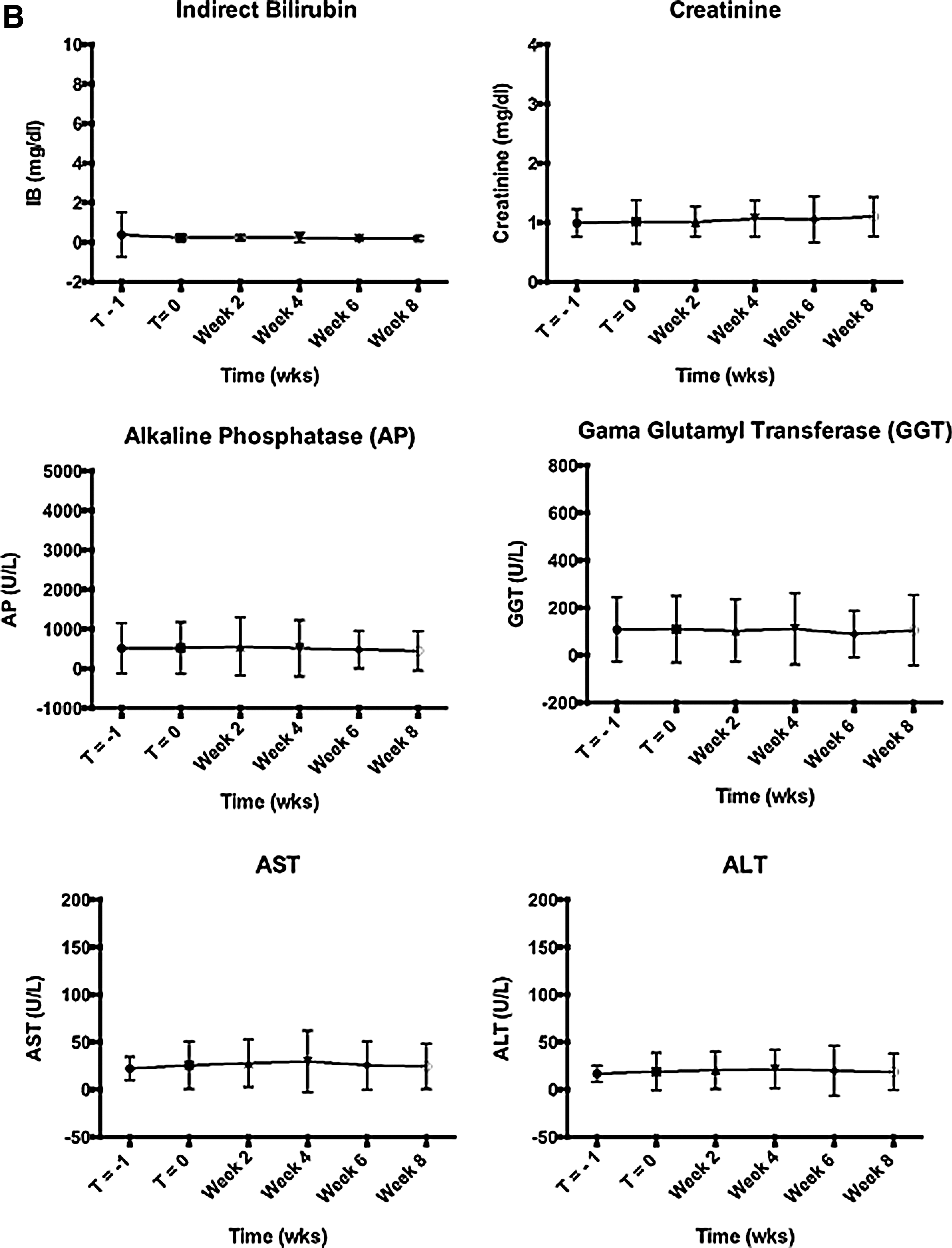
Blood parameters
Laboratory test results (complete blood count, kidney function, ALT, AST, ALP, and GGT, bilirubin) (Fig. 2B) and assessed inflammatory parameters (CRP, ESR, and α-1-acid glycoprotein), cytokines (IL-1, IL-6, and TNF-α) did not change (Fig. 3).
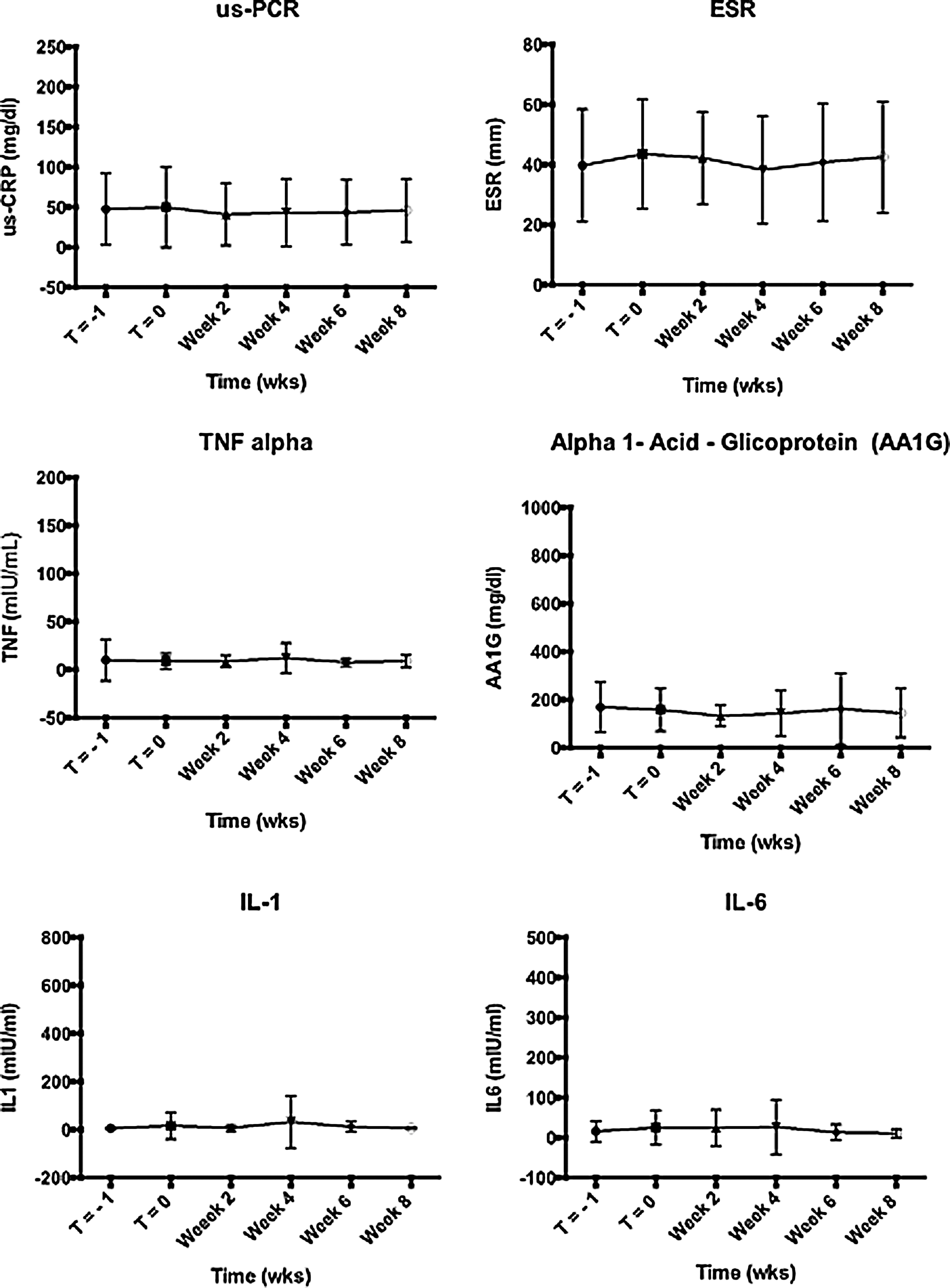
Variation in inflammatory parameters during the 8-week treatment: erythrocyte sedimentation rate (ESR); ultrasensitive C-reactive protein (us-CRP), tumor necrosis factor-α; interleukin-1, interleukin-6, and α-1-acid glycoprotein. Error bars correspond to 95% confidence intervals; p-values were considered to denote statistically significant differences if less than 0.05.
Adverse events
Few grade 3 or 4 adverse events occurred. One female participant exhibited grade 3 epigastric pain in week 6 of the treatment, but she partially improved after a dose reduction. Thus, that patient was withdrawn from the study at week 8 of treatment. One male patient exhibited grade 3 diarrhea in week 8, which improved after a 10-day interruption in the medication; that participant was also withdrawn from the study. One male patient with esophageal cancer exhibited grade 3 vomiting in week 3, which did not improve after discontinuation of the medication; thus, that participant withdrew from the study. Nevertheless, no association between the investigated drug and that adverse symptoms could be established because vomiting did not occur only after eating; it could have been due to the progression of the disease as a function of the primary tumor's location.
Grade 3 increases in alkaline phosphatase and GGT occurred in two and three participants, respectively. One of those participants also exhibited increased liver enzymes and biliary tract enzymes during the study, but those increases were within the thresholds established by the protocol. Only by the end of week 8 did the enzyme increase exceed the indicated thresholds; at that time, abdominal pain also appeared. The medication was then discontinued, and the patient's condition was investigated. The initial diagnostic tests (computed tomography, magnetic resonance cholangiography, upper gastrointestinal endoscopy, and Doppler ultrasonography of the portal vein) showed no abnormalities. The patient's attending physician established that the condition was due to disease progression. Three months later, imaging tests revealed the presence of secondary liver lesions, making the probability of a relationship between those adverse effects and the investigated medication lower as the diagnosis of disease progression was confirmed.
During the study period two participants developed sepsis, which had a pulmonary source in one case and a urinary tract source in the other. Both cases improved after a short hospital stay and intravenous antibiotic treatment.
One participant with colon cancer and peritoneal carcinomatosis exhibited a grade 4 partial bowel obstruction on day 15 that was due to peritoneal carcinomatosis and not judged by the investigators to be due to U. tomentosa. The patient was not considered a surgical candidate and subsequently died.
Table 2 describes all of the adverse events exhibited by the patients.
AST, aspartate aminotransferase; ALT, alanine aminotransferase; AP, alkaline phosphatase; GGT, γ-glutamyltransferase.
Overall and progression-free survival
No tumor response to the medication was identified, according to RECIST. Nevertheless, four patients (8% of the included participants) are still using the medication as of this writing, and their diseases have remained stable for more than 8 months. Those participants include one man with a neuroendocrine carcinoma of the sacrum who has been using the investigated medication for 15 months, three women with neuroendocrine carcinoma of the pancreas (two of whom also had colon and lung adenocarcinoma, respectively) who have remained stable for 12, 9, and 8 months, respectively.
The overall and progression-free survival rates of the patients are depicted in Figure 4.

Overall and progression-free survival curves.
Discussion
The anti-inflammatory properties of U. tomentosa are well known, and its beneficial effects in the treatment of chronic inflammatory diseases, such as osteoarthritis and rheumatoid arthritis, have been demonstrated in phase II studies conducted in humans. 25,26
The antineoplastic action of U. tomentosa has also been widely investigated. Several studies using variable methods and regimens of administration were conducted with tumor cell lines both in vivo and in vitro, and they exhibited promising results. 10,27,28 It is believed that the mechanisms involved in the antineoplastic effects of this plant include apoptosis induction in tumor cells 28 and a reduction in NF-κB levels. 13
Because of the above-mentioned anti-inflammatory and antitumor actions of U. tomentosa, this study assessed its effect on individuals with advanced cancers who had no further treatment options. In addition to the plant's possible antitumor action, its anti-inflammatory properties might relieve several of the symptoms exhibited by the targeted population; many of the issues that appear in advanced cancer seem to be due to the accompanying inflammation. 29,30
Two clinical studies of U. tomentosa have already been published. In the first, individuals with colon cancer 31 underwent adjuvant or palliative chemotherapy using FOLFOX (fluorouracil, oxaliplatin, and leucovorin). In the second, patients with breast cancer 32 received adjuvant chemotherapy with FAC (fluorouracil, doxorubicin and cyclophosphamide). In the former study, U. tomentosa showed no beneficial effect on the patients' symptoms; 31 in the second study, however, chemotherapy-induced neutropenia decreased in the group treated with U. tomentosa. In both studies, the dose of U. tomentosa was the same as that used in the current study. No other studies have assessed the effects of U. tomentosa in patients with advanced cancer, and no curative therapeutic options are available.
The participants in the current study had improved overall quality of life, reduced fatigue, and stabilized body weight. In some cases, disease appeared to have stabilized, although no objective evidence of a tumor response was found. Other studies showed a reduction in TNF-α levels 13,33 and increases in IL-1 and IL-6 levels, 34 but these results were not found in the current study. In addition, this study showed no evidence of a reduction in other inflammatory parameters, such as ESR, CRP, and α-1-acid glycoprotein. Therefore, the beneficial effects of U. tomentosa found in the present study might not have been due to its anti-inflammatory actions. The possibility of a placebo effect cannot be ruled out because this was not a controlled study. Future placebo-controlled studies with similar populations might clarify that issue.
The use of U. tomentosa seems to have been safe in the assessed population; few grade 3 and 4 adverse events appeared to be caused by the drug.
In conclusion, the phytotherapeutic agent U. tomentosa (cat's claw) improved the quality of life for individuals with solid tumors and no curative therapeutic options. Specifically, it improved their overall and social well-being and reduced fatigue, which is a common symptom in this population. Placebo-controlled studies are needed to confirm these findings, to assess more thoroughly the antineoplastic action of U. tomentosa, and to improve understanding of its effect on patient survival.
Footnotes
Author Disclosure Statement
No competing financial interests exist.