
Abstract
Objective:
To explore how contraindications to the use of acupuncture during pregnancy are managed in clinical practice.
Design:
Acupuncturists' views on their management of threatened miscarriage were sought by using a mixed-methods design involving a self-completed questionnaire and semi-structured interviews. An online survey was distributed through the Australian and New Zealand acupuncture associations requesting practitioners' to access an online link to a questionnaire hosted by Survey Monkey. This questionnaire examined acupuncturist's views on safety and the use of Traditional Chinese Medicine treatment modalities. Descriptive and bivariate statistics were used to analyze data. Thirteen participants were purposefully selected from the survey responses to further explore treatment management. These interviews were recorded via Skype, transcribed, and analyzed by using thematic analysis.
Results:
Of 370 respondents, 214 (58%) had treated women for threatened miscarriage within the previous year. Approximately half (58%) had treated four or fewer women, while a minority (14%) had treated 15 or more. The use of abdominal and blood invigorating points reflected diverse treatment strategies within acupuncture textbooks. While the majority avoided acupuncture points traditionally cautioned against in pregnancy, 13% would use LI 4, 22% would use SP 6, and 31% would use BL 32. Two safety themes emerged: “Well I'm safe because…justifying diverse approaches” and “A limited knowledge base—sorting it out for yourself,” illustrating how practitioners justified safe practice and had difficulty obtaining trustworthy treatment knowledge.
Conclusion:
Practitioners demonstrated interest in treating threatened miscarriage. All practitioners saw themselves as providing safe treatment. Those using historically contraindicated points justified their use on the basis of personal opinion, advice from trusted others, and clinical experience with a small number of women. In treating at-risk pregnancies, these justifications may be inadequate. Further research exploring the views of practitioners who are experienced in this specialized area would inform clinical practice for this common complication of early pregnancy.
Introduction
T
The evidence to date fails to support Western medical interventions or lifestyle changes as improving birthing outcomes, 5 –8 resulting in medical monitoring with a “watchful waiting” approach. Acupuncture is increasingly being sought in conjunction with Western medical care for pregnancy-related concerns, such as nausea and vomiting, back and pelvic pain, and labor preparation. 9 Acupuncture has been identified as a safe treatment during pregnancy, with no reported adverse events related to miscarriage or premature labor in the literature. 10,11 However, there are conflicting safety recommendations within acupuncture texts; specific acupuncture points are contraindicated for use at any time during pregnancy (Table 1). 12 –15 These points, traditionally used to stimulate labour, are cautioned against due to concerns they may stimulate miscarriage in early pregnancy or premature labor in later pregnancy. 16 However, an argument has been made that these historical concepts no longer apply and these points are no longer contraindicated at any time in pregnancy. 17,18 Although no high-quality studies demonstrate the safety or effectiveness of acupuncture for threatened miscarriage, 16 acupuncture texts recommend treatment for bleeding in early pregnancy. 19 –23 However, these texts feature conflicting recommendations for safe treatment. Because of concerns about stimulating miscarriage, acupuncture points for invigorating blood are cautioned against in early pregnancy, but some texts recommend their use. 21,22 In addition, while lower abdominal points are recommended, different types of stimulation are considered safer: moxibustion only 21,22 or needles only. 19 Although conflicting treatment recommendations can be found within many areas of Traditional Chinese Medicine (TCM), within this speciality field of treating women with at risk pregnancies, these conflicting safety recommendations may create uncertainty regarding safe clinical practice for acupuncturists.
With a growing interest from women seeking acupuncture during pregnancy 9,24 and a willingness from Western health practitioners to refer pregnant women, 25 acupuncture may provide an alternative treatment option to watchful waiting. It is not known whether treatment contraindications within the literature influence clinical practice. The aim of this study was to explore acupuncturists' views on treatment for threatened miscarriage and how contraindications to the use of acupuncture during pregnancy are managed in clinical practice.
Materials and Methods
This was a mixed-methods study in which the most appropriate research methods (quantitative or qualitative) were used to investigate the research question. This study used a sequential design. An online survey was administered, with participants subsequently invited to leave their contact details if they were interested to participate in an interview. was approved by The University of Western Sydney Human Research and Ethics Committee approved this study (H8935).
Survey details
An anonymous, web-based, self-completed questionnaire was distributed to practitioners in Australia and New Zealand. The survey was developed by the authors (D.B. and C.S.) and piloted by 11 acupuncturists involved in women's health, with no significant changes required. All participants were asked whether they had treated threatened miscarriage in the past year, about any safety concerns they may have regarding acupuncture, and questions describing their clinical experience and style of acupuncture practice. For practitioners treating threatened miscarriage, further questions explored conflicting recommendations within acupuncture texts, specifically acupuncture points they would avoid and whether and how they used abdominal and blood invigorating points. The survey required less than 20 minutes to complete.
The survey was distributed between April and May 2011. Because it was not possible to identify practitioners involved in this specialized area of clinical practice, convenience sampling was used. A generic invitation to participate in the survey was sought from acupuncturists belonging to the main professional acupuncture bodies: the Australian Acupuncture & Chinese Medicine Association (AACMA), Australian Traditional Medicine Society (ATMS), Acupuncture Association of Australia (ACUPAA), New Zealand Register of Acupuncturists (NZRA), New Zealand Chinese Medicine and Acupuncture Society (NZCMAS), and the New Zealand Acupuncture Standards Authority Inc. (NZASA). The professional associations were responsible for distributing the survey. An email invitation was sent to members with links to the questionnaire accessed through the Internet provider Survey Monkey (
Interviews
Semi-structured interviews were conducted by a researcher (D.B.) using a topic guide of seven questions to explore participants' experiences of providing care. Examples of these questions included the following: Can you tell me about any points you do not use in the treatment of threatened miscarriage and why? When treating blood stagnation, what specific needling and/or moxibustion techniques do you use and why?
These interviews typically lasted 1 hour, were conducted through the online medium of Skype, were recorded on the researcher's computer, then transcribed and analyzed using thematic analysis. Thematic analysis is widely used as a foundation in qualitative analysis to formally evaluate and code the data. 26
Data analysis
Data were collected in the form of an Excel spreadsheet and exported to SPSS software (IBM, Chicago, IL), version 9.1, for analysis. Demographic data was analyzed using descriptive statistics for characteristics of survey respondents, with frequencies and percentages. Cross-tabulations were generated and chi-square tests undertaken to determine patterns of use for contraindicated points with sociodemographic characteristics. The conventional 0.05 level of significance was used to test for statistical differences.
To analyze thematic data, the researcher became familiar with the data; generated initial codes; searched for themes; and reviewed, defined, and named these themes. 26 The number of interviews required to achieve saturation was determined when new information produced little or no change in data collection and analysis. 27 To reduce possible researcher bias, NVivo 9 (QSR International, Melbourne, Australia) was used. This allowed coding categories to be sent to the second and third authors for comparison and verification. In searching for, reviewing, and defining themes, a thematic “map” of the analysis was produced, generating clear definitions and names for each theme. 26 Two authors (H.D. and C.S.) provided critical feedback and reflection as the themes developed.
Results
A total of 370 replies were received from 3151 invitations, a response rate of 11.7%. Three hundred and five participants provided demographic information. The majority were female (197 [64.6%]), practicing in Australia (223 [73.1%]), and selected their main style of acupuncture as “eight principals” (204 [66.9%]) (Table 2). Approximately half had been in practice for less than 10 years (173 [57.6%]) and held a bachelor's degree as their highest acupuncture qualification (166 [54.4%]).
More than one answer possible.
CAM, complementary and alternative medicine.
Of the initial 370 responders, 214 (57.8%) had treated women for threatened miscarriage in the past year and 156 (42.2%) stating that they had not. Among those not treating threatened miscarriage in the past year, 15 supplied no further information and were excluded from further analysis. Further analysis on this group was restricted to 141 participants. For participants who had treated women within the past year, 50 supplied no further information and were excluded, leaving 164 participants actively treating threatened miscarriage for further analysis. Although slightly more than half (95 [57.9%]) of the participants had treated four or fewer women in the previous year, a minority (23 [14.0%]) had treated 15 or more women.
Quantitative Findings
Patterns of use for practitioners treating threatened miscarriage
A range of TCM modalities were used. The most common was acupuncture (152 [92.6%]), followed by moxibustion (111 [67.6%]), Chinese herbal medicine (101 [67.0%]), TCM lifestyle advice (103 [62.8%]), and TCM dietary advice (84 [51.2%]). Other modalities (9.1%) included qigong, tuning forks, heat lamps, relaxation techniques, and Western herbal supplements.
When asked about acupuncture points they would avoid when treating threatened miscarriage, most of the 164 practitioners answering this question selected points that were cautioned against because of their historical use for stimulation of labor; however, some practitioners did not select these contraindicated points. While 143 (87.2%) selected LI 4 as a point they would avoid, 21 (12.8%) did not (Fig. 1). In addition, 36 (22%) would not avoid SP 6 and 42 (25.6%) would not avoid GB 21. Practitioners would also not avoid using BL 31, BL 32, BL 33, or BL 60 (n=51–71 [31.1%–44.5%]). In addition, 5 (3%) indicated that they did not view any point as contraindicated when treating threatened miscarriage. Practitioners also avoided acupuncture points that were not historically associated with stimulating labor: KI 6, hua tuo jia ji points, SP 3, LU 7, and BL 63 (n=16–34 [9.7%–20.7%]), with 33 (20.1%) also nominating one or more of the following: KI 1, KI 3, ST 36, LV 3, GV 20, GB 20, GB 34, SP 1, HT 9, and SP 10.

Contraindicated acupuncture points that the participants would not avoid (n=164).
The practitioner's style of practice and experience was associated with the use of contraindicated points (Table 3). Medical acupuncturists were more likely to use the contraindicated points GB 21 (p=0.002), LI 4 (p=0.058), and SP 6 (p=0.056) (the latter two approaching statistical significance). Practitioners with 10 or more years of clinical practice were also significantly more likely to use the contraindicated points LI 4 (p=0.002), SP 6 (p=0.001), GB 21 (p=0.012), and BL 60 (p=0.001).
p<0.05.
TCM theory has treatment concepts to resolve bleeding that may apply to treating threatened miscarriage. These relate to the use of abdominal points and points to invigorate blood. Lower abdominal points were avoided by 53 respondents (32.3%), while 58 (35.9%) used moxibustion or acupuncture; however, 24 (14.6%) would use only acupuncture while 17 (10.4%) would use only moxibustion (Fig. 2). For the use of points to invigorate blood, practitioners were divided, with 79 (48.2%) stating that they did not use these points while 71 (43.3%) did use these points (Fig. 3).
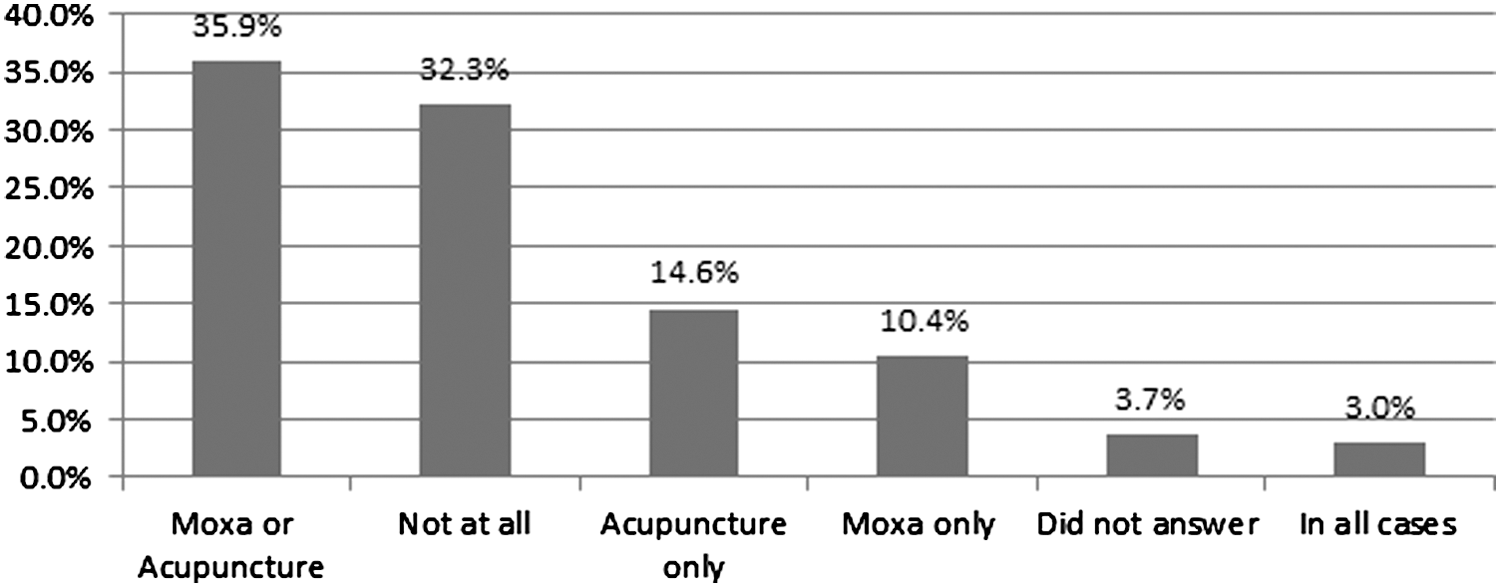
Use of moxibustion or acupuncture on abdominal points (n=164). Moxa, moxibustion.
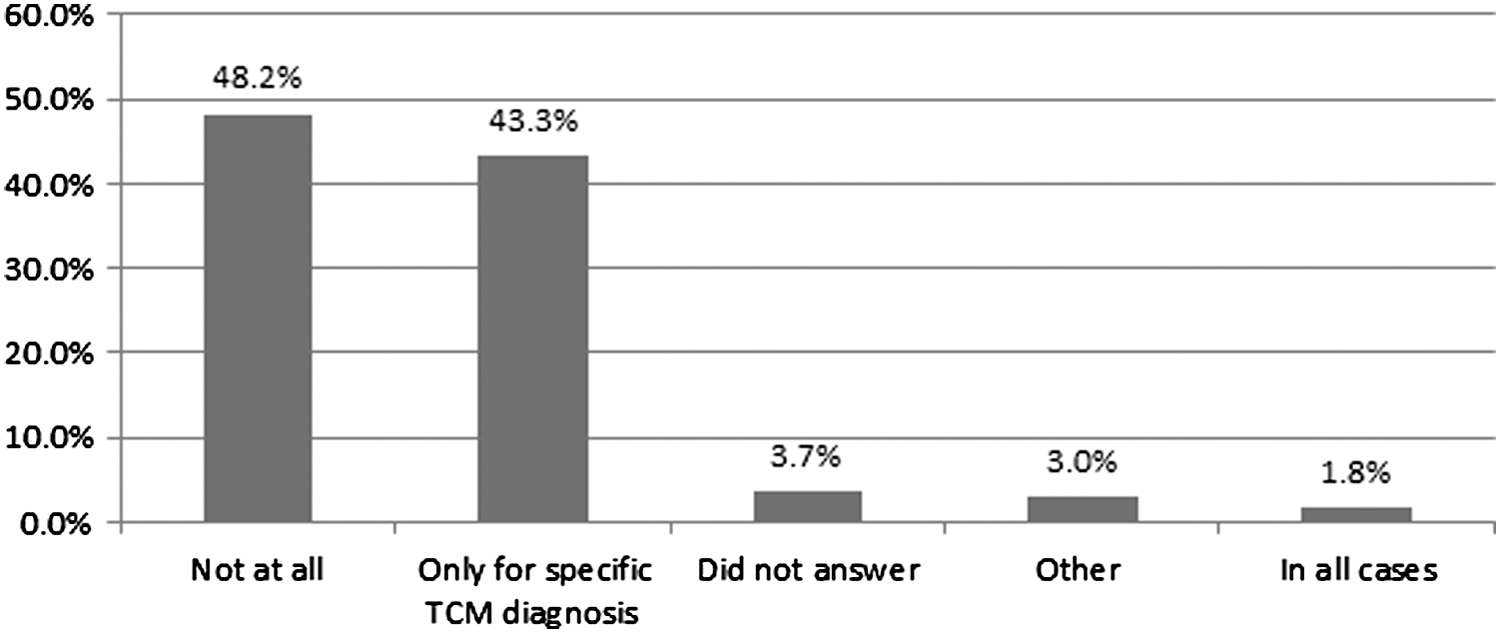
Use of acupuncture points for moving or invigorating blood (n=164). TCM, Traditional Chinese Medicine.
When asked whether they had any safety concerns about treating threatened miscarriage, a minority (20 [12.2%]) of those treating expressed concerns that “other” inexperienced practitioners may stimulate miscarriage through inappropriate treatment. For those practitioners not treating threatened miscarriage, only a minority (28 [19.9%]) had safety concerns. These concerns focused on delivering an incorrect treatment that may stimulate miscarriage or being held responsible for an inevitable miscarriage.
Qualitative findings
Of the 58 participants who provided contact details, 10 were excluded because of incomplete information, 10 because they did not have more than 6 years of clinical experience, and 14 because they had treated fewer than five women in the previous year. Therefore, 24 practitioners were eligible. Thirteen were then purposefully selected to further explore specific aspects of their clinical practice, specifically their use or avoidance of contraindicated points, abdominal points, and points that acted to invigorate blood. Six of these practitioners stated that they would not avoid contraindicated points, 8 used abdominal points, and 11 used blood invigorating points. All practitioners had at least 6 years of clinical experience, and 4 had been in practice for over 20 years. Eleven were practicing in Australia and 12 were female. Two safety themes emerged: “Well, I'm safe because…acupuncturists' justifying diverse approaches” and “a limited knowledge base—sorting it out for yourself.” Together, these reflected acupuncturists' views on the challenges of providing safe care for women in this specialist area of practice.
“Well I'm safe because…acupuncturists' justifying diverse approaches”
All practitioners viewed themselves as providing safe treatment. Practitioners who refrained from using contraindicated points expressed how they respected historical knowledge, while practitioners using these points expressed how they were safe because of their needling techniques: I don't really see that there would be a problem…I think in the earlier books they are talking about thick needles and really strong technique. Not the fine needles that we have these days. (P7, 20 years' experience) LI 4 and SP 6, obviously I never, never, never, never. But I have used LI 4 on its own. What I'll do is just leave it on for a couple of minutes and take it out. (P5, 7 years' experience)
Participants' personal experiences (and those of trusted others) reinforced their viewpoint, justifying either use or avoidance of these points: I do actually know of people who have tried to abort and were utterly unsuccessful. I've heard [name of acupuncture teacher] talk about it, he knows of people who've tried. In China it's been tried…that gives you feedback that even if you try really hard to induce a miscarriage, it's not usually successful. (P10, 20 years' experience) I had a girlfriend who found that she was pregnant and she said I don't want to have this baby. I said, well let's just do some acupuncture and see what happens. Whether or not it would have happened anyway, she did miscarry. (P6, 6 years' experience)
Practitioners also expressed how women and Western medical practitioners had safety concerns about the use of Chinese herbs. The majority limited their use of herbs in clinical practice to accommodate these concerns: I had quite a few obstetricians referring and they generally didn't like any of their clients having herbs. So generally if a client was under an obstetrician, I just wouldn't do herbs. (P2, 20 years' experience)
“A limited knowledge base—sorting it out for yourself.”
This theme reflects how participants had difficulty sourcing knowledge they saw as useful: “You can try and do research but then you are left with not a hell of a lot” (P10, 20 years' experience). In part this was due to the conflicting information: There's a lot of rumor around all of this—things that you should and shouldn't do in pregnancy. I think it leaves people a little bit afraid of what to do. (P6, 6 years' experience)
The advice of experienced practitioners was valued over textbooks, with some practitioners deliberately seeking out those they saw as having valuable experience: I've found that the most useful information has not been in textbooks, it's been from talking to practitioners who've been in practice for 15,20 years plus. (P6, 6 years' experience)
Others felt that clinical practice added to their knowledge over time. While practitioners did not discuss any formal follow-up, they spoke of gaining confidence through observing their treatment results, focusing on the physical and emotional changes rather than measuring success through ongoing pregnancies: If I have a woman smiling by the time she walks out, feeling more hopeful because she's been absolutely beside herself when she walked in, I think that's a measure of success in itself. If the bleeding has slowed or it's stopped…then you're looking at those symptoms as well. (P5, 7 years' experience) They feel that their abdomen is light and warm so that there's no more sensations of grabbing, pulling discomfort…so they feel calm and they feel supported. (P2, 20 years' experience)
Discussion
The findings from the survey demonstrated that acupuncturists were interested in and actively treating threatened miscarriage. Participants perceived themselves as providing safe treatment despite using diverse modalities, and some used points contraindicated because of their traditional use for stimulating labor. Some practitioners also considered commonly used points with no historical use for stimulating labor as contraindicated. The interviews further illustrated how practitioners perceived that there was limited information available from acupuncture texts and how those using historically contraindicated points justified safe practice according to personal opinion, advice from trusted others, and clinical experience.
Acupuncturists are treating a wide range of pregnancy-related conditions. 28 To date, the adverse effects of using acupuncture in pregnancy are predominantly minor events related to bruising and pain at the needle site. 10 It may be that concerns about historically contraindicated points stimulating miscarriage and premature labor can be dismissed as irrelevant. 17,18 However, a finding from this study highlighted practitioner experience of pregnancy loss following the use of these contraindicated points and that acupuncturists experienced in treating threatened miscarriage (those treating more than 10 women in the past year) were not more likely to use these historically contraindicated points. Within the interviews, practitioners using contraindicated points discussed the use of LI 4, SP 6, BL 32, GB 21, and BL 60 for calming women and treating back pain. They also discussed how these points were used unsuccessfully in China to induce abortion.
However, literature from China discusses how contraindicated points are used to stimulate first-trimester abortion. Although these treatments may not reflect Western clinical practice, with strong stimulation over several consecutive days, a reported 75.5% success rate for inducing spontaneous abortion is worthy of consideration. 29 It is also reported that combining acupuncture with medication results in accelerated cervix dilatation and fetal sac release compared with using medication alone. 30 Although these articles from China lack rigor, they may indicate that caution is required with use of these points in early pregnancy. An argument has also been made that historically contraindicated points are safe because they demonstrate no adverse outcomes in early pregnancy for rats. 17,31,32 However, because rats are not considered a good model for understanding early pregnancy responses in women, 33 this argument may not be valid. A further argument for the use of historically contraindicated points is that avoiding these points limits clinical practice. 17 Certainly these points have been used in clinical studies when treating pregnant women, with LI 4, BL 32, BL 33, and BL 60 used for back pain, 34 LI 4 for heartburn, 35 GB 21 for insomnia, 36 and LI 4 and GB 21 for headache. 37 However, in all of these studies treatment was administered only after 12 gestational weeks. Physiology of early pregnancy differs in that it requires a low oxygen environment until 8–10 gestational weeks and does not protect against uterine contractions as seen in the second trimester. 38,39 This may mean that the use of these points after 12 gestational weeks is not transferable to early pregnancy. While acupuncture texts recommend a range of treatment options for the treatment of back and pelvic pain, heartburn, and headaches in pregnancy, these texts do not include these contraindicated points. 19 –23 It is therefore questionable that avoiding these points would detrimentally affect clinical practice.
The survey found that practitioners with Western medical acupuncture training were more likely to use GB 21, LI 4, and SP 6. Although this finding was limited to a small number of participants, this may reflect this particular style of acupuncture practice, with recommendations from Western medical acupuncturists that historically contraindicated points are not relevant during pregnancy. 17,18 It was interesting that while recommendations for the use of SP 6 with moxibustion during pregnancy can be found within Japanese-style acupuncture, 40 participants in the survey practicing this style were not more likely to use acupuncture on this point. This finding again is limited by the small number of participants but may reflect their perception that moxibustion and acupuncture have different energetic effects.
A review to identify adverse events with use of acupuncture during pregnancy found that these events were often poorly reported. 10 When interviewed, practitioners using historically contraindicated points justified how their treatment was safe, but without acknowledging how adverse events relating to miscarriage would be difficult to detect because of the small number of women they saw. This may be relevant as approximately half of those surveyed had treated four women or fewer.
To date no high-quality studies have detailed the use of acupuncture for threatened miscarriage. 16 The finding that practitioners were interested in treating threatened miscarriage but found it difficult to obtain trustworthy treatment information has implications for clinical practice. Practitioners identified a preference for their own clinical experience and those of experienced practitioners over textbook information. Future relevant practitioner research could explore experience-based knowledge, using the Delphi consultation process 41 with experienced practitioners to explore these practice concerns and make recommendations that would be viewed as valuable by acupuncturists in clinical practice. It may also be relevant that although practitioners in the survey selected Chinese herbal medicine as a treatment modality, practitioners interviewed discussed how they limited their use of these herbs because of safety concerns from women and Western medical practitioners. Further research may be able to clarify how these herbs are used in clinical practice.
Strengths and limitations
The use of mixed methods allowed for in-depth exploration of the data arising from the survey. Online technology for the survey and interviews also made it possible to eliminate postage costs and access experienced practitioners for interviews. The use of Skype to interview participants may have influenced participants' willingness to be interviewed; however, because 48 practitioners expressed interest in participating using this technology it did not appear to be a barrier. Limitations of the survey included the low response rate, recall bias, and a self-selecting sample. The low response rate significantly limits the validity of data from this study. This response rate may reflect pregnancy care as a specialized area of acupuncture practice and mirrors the 11% response rate from a survey among Australian and New Zealand acupuncturists treating women's health conditions. 28 It may be that practitioners not involved in the specialized area of pregnancy care chose not to respond. Despite the low response rate, the demographics mirror those of practitioners surveyed in Australia, 42 with more female than male practitioners, over 50% practicing for less than 10 years, and over 50% having a bachelor's qualification, suggesting that this survey was representative and allowed valuable practitioner information to be collected in this specialized area of practice for the first time.
Conclusions
These findings indicate an interest among acupuncturists in treating threatened miscarriage, although practitioners identified difficulties in obtaining trustworthy treatment knowledge. All practitioners considered their treatment safe; however, treatment rationales for those using historically contraindicated points were not based on TCM theory, pregnancy physiology, or current research, but rather on personal opinion, advice from trusted others, and clinical experience with a small number of women. In treating at-risk pregnancies these justifications may be inadequate. Further research exploring the experiences of practitioners who have experience in this specialized area would inform clinical practice for this common complication of early pregnancy.
Footnotes
Acknowledgments
The authors wish to thank all those registered acupuncturists in Australia and New Zealand who participated in this survey and interviews. We also acknowledge Judy James and Jazz Tyrril (AACMA), Paddy McBride and Lesley Haiselden (NZRA), Matthew Boylan (ATMS), Leonie McMahon (ACUPAA), Dr. Joan Campbell (NZASA), and Stephen Xu (NZCMAS) for their assistance in distributing this survey to their members.
Author Disclosure Statement
No competing financial relationships exist.