
Abstract
Introduction:
T'ai chi chuan is a beneficial exercise of improving health and function. Biomechanical insights of t'ai chi chuan are less understood.
Objectives:
To study t'ai chi gait (TCG), a common form of t'ai chi chuan in order to quantify external knee adduction moment (EKAM) as a key indicator of mechanical loading of the medial compartment of the knee compared with normal walking (NW).
Design:
A quantitative biomechanics approach to determine peak EKAM for NW and TCG.
Results:
There were a tri-modal pattern of EKAM during TCG and a bimodal pattern of EKAM during normal walking. In addition, subsequent analysis showed a 25%–47% reduction in peak EKAM during double support phases of TCG compared with NW; the peak EKAM of TCG during single-limb support phase showed significantly higher magnitude than the other two double-support phases.
Conclusion:
These results indicate that t'ai chi chuan might be a beneficial intervention for reducing the medial mechanical load at the knee joint, particularly during the first double-support phases of TCG, but the special consideration of higher peak EKAM of single-limb support phase is needed during regular t'ai chi chuan practice.
Introduction
T'
One of the most studied components of TCC training has involved the musculoskeletal system. Research has demonstrated improvements in many neuromuscular components associated with quiet standing and gait; 6 –8 improved strength, balance, and flexibility; 9 –11 and reduced probability of falling among the elderly. 12,13 However, a limited number of studies have examined lower-extremity joint kinetics comparing t'ai chi gait (TCG) and normal walking (NW). 5,6,14 TCG is the most common form derived from TCC with gait-like movement patterns. Analysis of joint kinetics during TCG and NW in healthy young and elderly t'ai chi chuan practitioners showed larger peak shear forces in the ankle, knee, and hip joints and larger peak moments in the knee and hip joints during TCG. 5 Although this finding has implications for exercise and specific types of patients, additional measurements that quantitatively characterize joint loading patterns could be meaningful, particularly when NW and TCG are being examined.
In this case, examining a local joint factor involving knee joint loading measured as the mechanical factor of external knee adduction moment (EKAM) could be important. 15,16 EKAM, a surrogate indicator of medial knee load, is determined by the product of the ground reaction force and frontal plane lever arm length. 17 During NW, approximately 70% of knee joint loading passes through the medial compartment. An elevated EKAM is strongly correlated to the presence of degenerative knee joint osteoarthritis (OA), radiographic OA disease severity, and rate of OA progression. 17
Treatment strategies to reduce medial knee load, including gait modification, benefit patients with knee OA. 18 Some gait modification strategies reported include walking with increased toe-out angle, lateral trunk lean, and the use of gait aids. 18 Weight-bearing activities that reduce EKAM could be beneficial to people with degenerative joint disease by reducing pain and allowing increased exercise participation. The presence of EKAM and its magnitude have been reported in studies evaluating walking. 18 Other studies have reported elevated EKAM during walking in people with knee OA. 19,20 To what degree or magnitude EKAM is present during TCG is unknown. An important initial step in quantifying EKAM during TCG is to make comparisons with NW. By doing so, findings will lay the biomechanical foundation to examine the effectiveness of TCG in treating knee OA. The study hypothesis was that knee peak EKAM would be significantly lower during TCG when compared with NW.
Materials and Methods
Participants
Ten healthy volunteers were recruited to participate in the study: five men and five women (mean age, 58.4 ± 13.1 years; height, 1.73 ± 0.08 m; weight, 73.5 ± 18.5 kg). Inclusion criteria included a minimum of 2 years' experience in performing t'ai chi chuan (TCC) and knowledge of the 24 simplified yang style forms of TCC. Exclusion criteria included history of musculoskeletal and/or neurologic pain or injury to either lower extremity. Persons with cardiopulmonary limitations were also excluded from participating. In compliance with study procedures approved by an institutional review board, each participant read and signed an informed consent document before data collection.
Instrumentation
An infra-red motion analysis system with seven high-speed cameras (VICON, Oxford, United Kingdom) was used to record both TCG and NW. The sampling rate was set at 100 Hz. The cameras were set up along a 3-m (width) × 10 m (length) walkway so that all of the markers on the participant could be viewed during all calibration and motion trials. Before data collection, the cameras were dynamically calibrated by using an L-frame 500-mm wand.
Two force plates (Advanced Mechanical Technology Inc., Watertown, MA) embedded in the walkway were used to record ground reaction forces (GRF) at 1000 Hz during the stance phase of each gait. The two force plates were synchronized with the VICON cameras so that the coordinates of each marker and GRF were simultaneously collected on a desktop computer by using Nexus software (VICON).
Data collection procedures
Participants wore shorts and were barefoot for all static calibration and motion trials. Reflective markers (semispherical, 15-mm diameter) were attached bilaterally to various bony landmarks of the body. These included the anterior and posterior superior iliac spines and the tops of the iliac crests of the pelvis, the greater trochanters and medial and lateral epicondyles of the femur, the medial tibial and lateral fibular malleoli of the shank, the calcaneus, the first and fifth metatarsal heads, the sternum, and the acromion processes. In addition, clusters of three markers were attached to the lateral thighs and shanks for reference locations (Fig. 1). A static calibration trial was collected at the beginning of the motion trials. Participants were asked to stand quietly in an anatomically neutral position with their feet spread apart at shoulder-width and their shoulders slightly abducted for 5 seconds. Participants then performed four trials each for the NW and TCG.
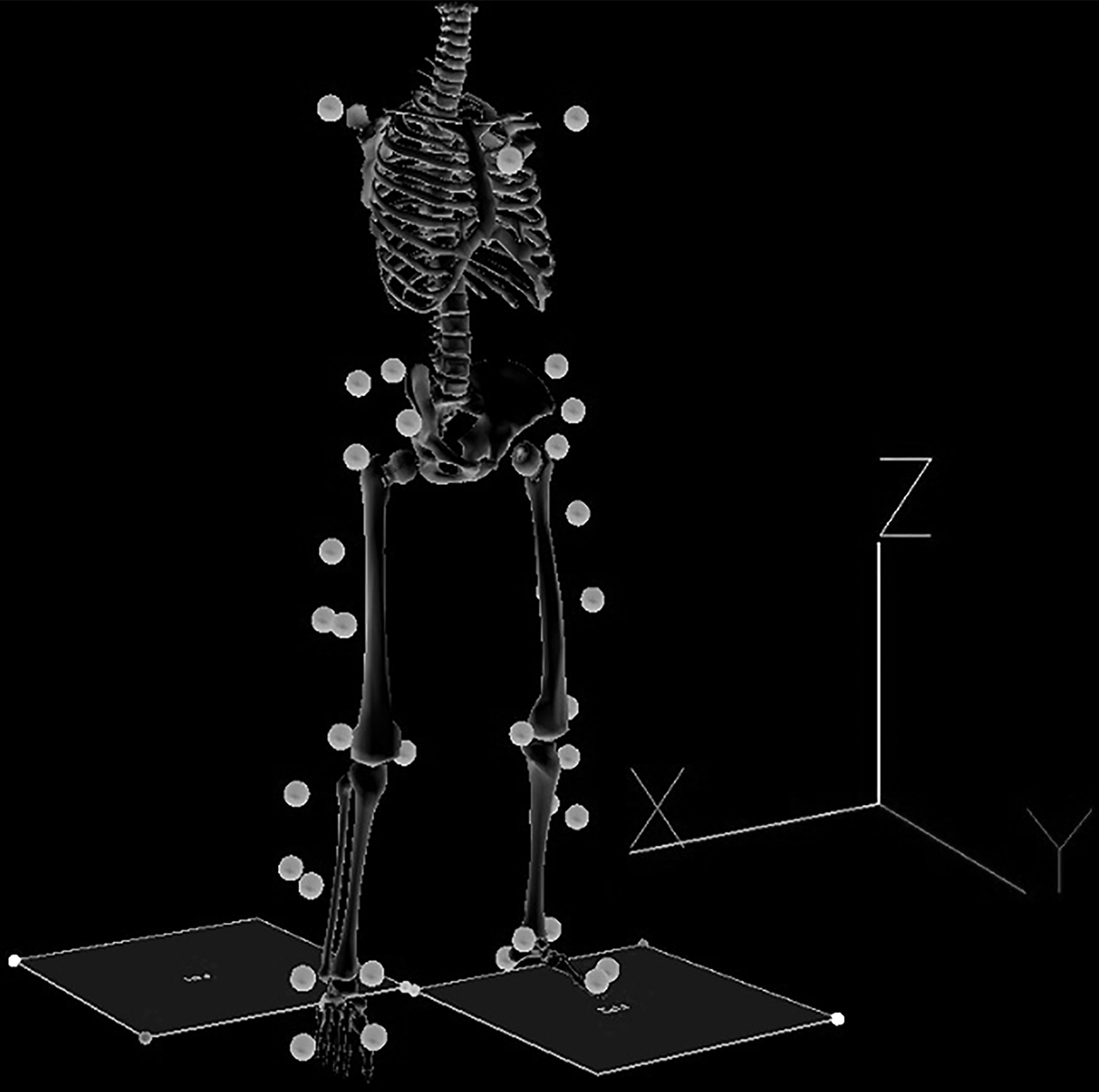
Experimental setup and marker placement on lower extremity.
For the NW motion trial, the participant began at a designated starting line and walked naturally at a self-determined speed so that the right foot fully contacted the first force plate and the left foot fully contacted the second force plate. The TCG motion trial began with the participant standing in a common TCC stance with knees slightly bent and arms slightly raised forward in a curved position, with palms angled inward and held at the level of the abdomen. 21 TCG was performed as a series of uninterrupted forward steps and strides, with unique gait phases that included single support, double support, and swing (Fig. 2). 6 TCG as one particular aspect of TCC was compared with NW to study EKAM because both are a means of bipedal forward locomotion that incorporate distinct phases of gait.

Illustration of t'ai chi gait phases.
Data analysis
Three-dimensional marker data were collected and filtered with a Butterworth low-pass filter (6-Hz cutoff). Right-handed local segmental and lab coordinate systems were constructed so that the x-axis was directed laterally to the right, the y-axis was directed anteriorly, and the z-axis was directed superiorly (Fig. 1).
Three-dimensional segmental Euler angles (x-y-z sequence) were computed on the basis of the rotation matrix between global and local coordinate systems of each segment. Consequently, joint angular displacement, velocity, and segmental angular velocity were derived from three-dimensional Euler angles. 22 A traditional inverse dynamics approach was used to compute EKAM with the derived kinematic and ground reaction force data. 22 The dependent variable, peak EKAM, was determined for the entire stance phase of NW gait and of TCG. Paired Student t-tests were perfomed using SPSS software (SPSS version 22, Armonk, NY, USA) to compare peak EKAM of the entire stance phase of NW to the entire stance phase of TCG. The level of significance was set a priori at p = 0.05 for all analyses.
Results
No significant (p = 0.501) peak EKAM difference was found for the entire stance phase between NW (0.313 ± 0.036 N · m/kg) and TCG (0.367 ± 0.097 N · m/kg), but the magnitude of peak EKAM during TCG was higher than that during NW. The EKAM of TCG showed a tri-modal pattern, with three peaks during the entire stance phase (Fig. 3). During the entire stance phase of TCG, the first peak EKAM occurred at double-support phase I, the second peak EKAM (the highest one) always occurred at the single-limb support phase, and the third peak EKAM occurred at the double-support phase II. Because of the distinct pattern of EKAM during TCG, the peak EKAM of the entire stance phase of TCG may or may not reflect the nature of medial loading response of knee joint during TCG.
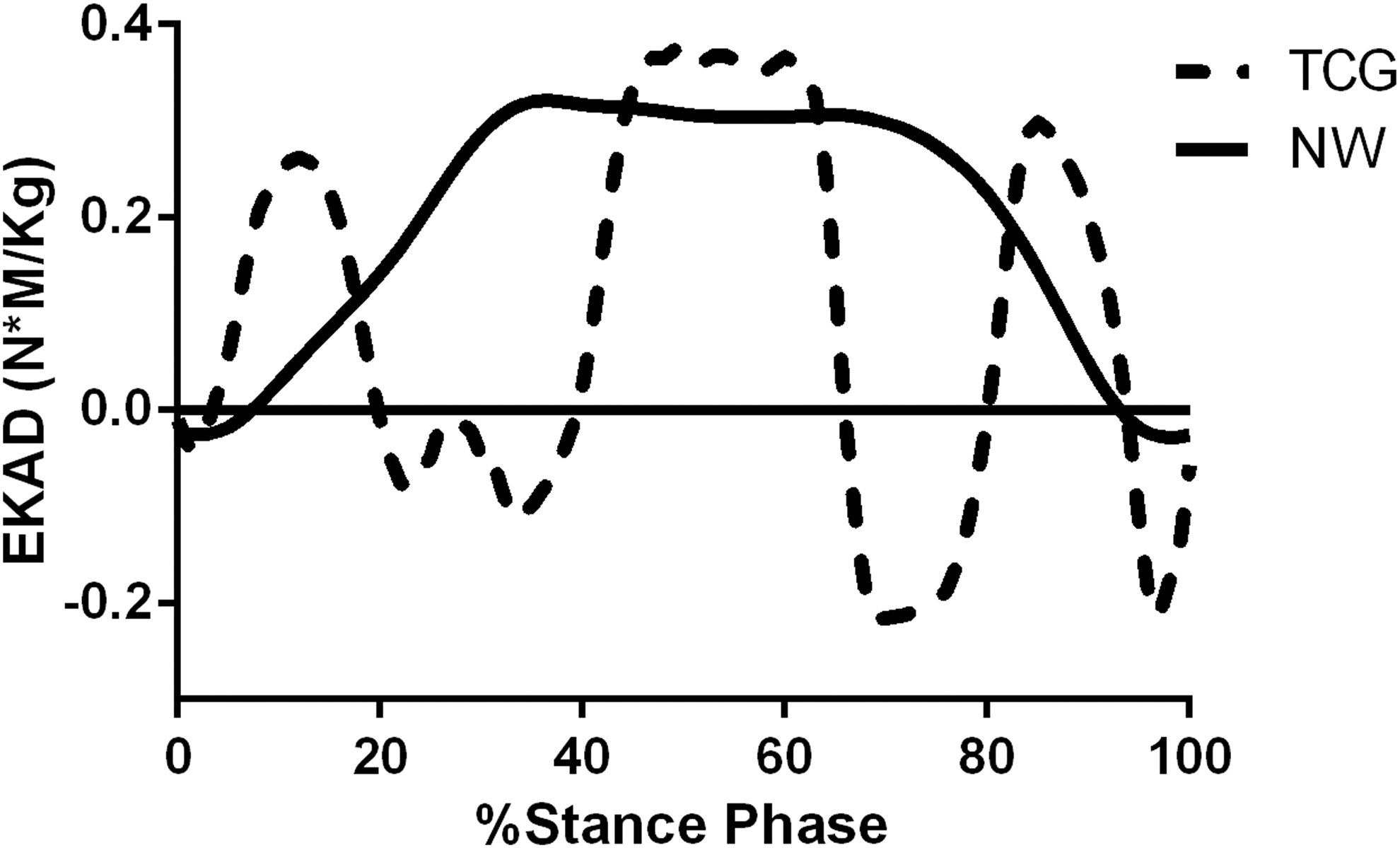
Single representative time series data of external knee adduction moment (EKAM) during stance phase of t'ai chi gait (TCG) and normal walking (NW). Positive values indicate external adduction moment; negative values indicate external abduction moment.
Subsequent comparisons of TCG during double-support phase I and double-support phase II were made to the entire NW stance phase and TCG single-limb support phase by using peak EKAM measurements. Peak EKAM was significantly (p = 0.024) reduced by 47% between the NW stance phase (0.313 ± 0.036 N · m/kg) and the TCG double-support phase I (0.165 ± 0.077 N · m/kg) (Fig. 4). Peak EKAM showed no significant difference (p = 0.351) between NW stance phase (0.313 ± 0.036 N · m/kg) and TCG double-support phase II (0.234 ± 0.099 N · m/kg). Although not significantly different, the peak EKAM of TCG double-support II was approximately 25% lower. Peak EKAM showed a significant difference (p = 0.001) between TCG single-limb support phase (0.367 ± 0.097 N · m/kg) and the other two double-support phases (double support phase I: 0.165 ± 0.077 N · m/kg; double-support phase I: 0.234 ± 0.099 N · m/kg) (Fig. 4).
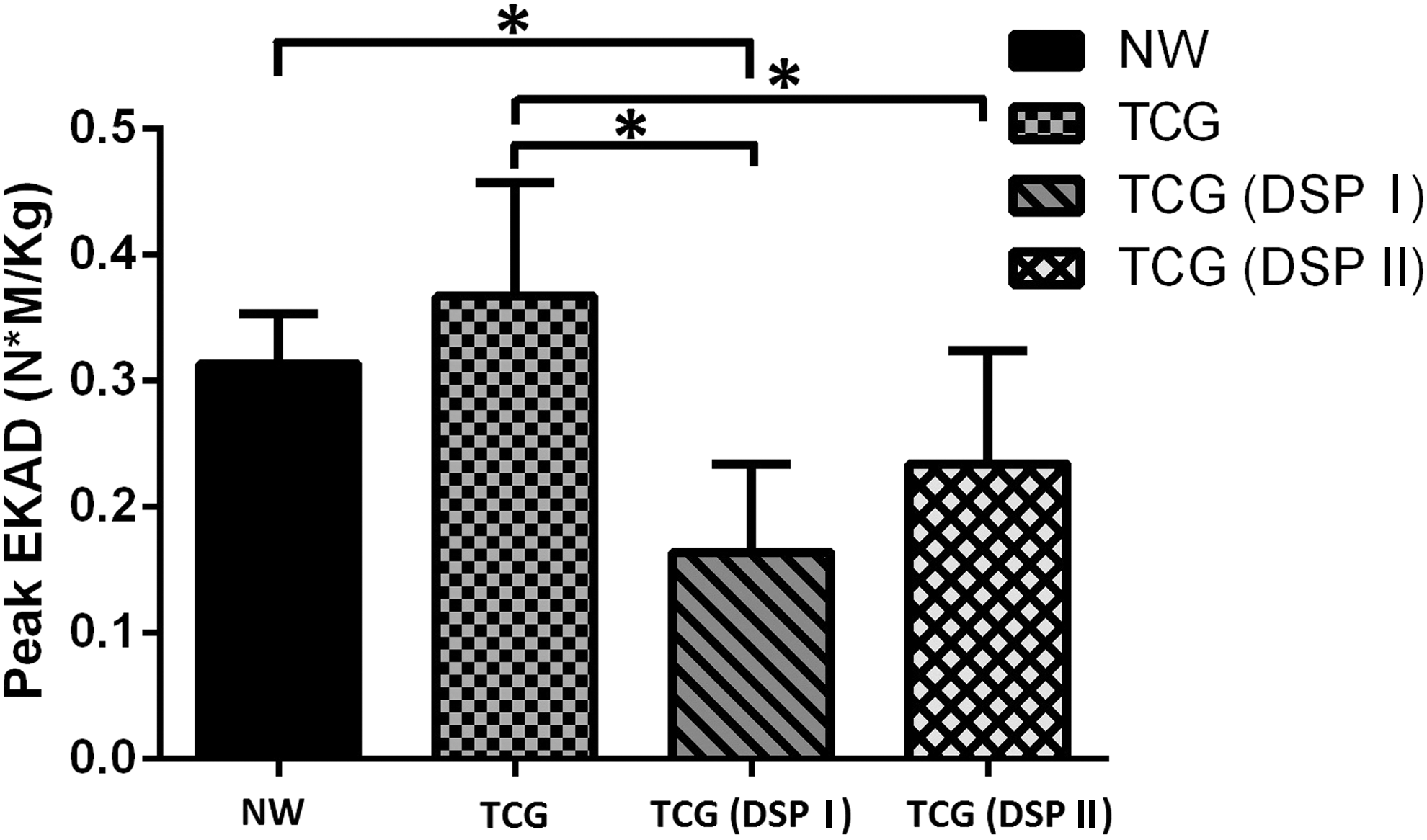
Bar plots of peak EKAM during NW and TCG, TCG double-support phase I (DSP I), and TCG double-support phase II (DSP II).
Discussion
This study examined TCG (one particular aspect of TCC leg movement) and NW because both are a means of bipedal forward locomotion. 5 The external adduction moment was studied because it has received significant attention in the investigation of medial compartment loading of the knee joint. 15 –17 The susceptibility of the medial compartment to knee pathology, such as OA development, may relate to greater load distribution to the medial than the lateral compartment, even in healthy knees during gait. 23 An understanding of this biomechanical characteristic could be important to understanding TCG as an important and essential step for individuals and clinicians who might choose to participate in or prescribe this form of exercise.
Results showed that TCG and NW exert different effects on dynamic knee load at varying points across the gait cycle. The hypothesis that the knee's peak EKAM would be significantly lower during TCG than during NW was not supported by the results of the entire stance phase. Surprisingly, the subsequent analysis showed significant peak EKAM reduction in the double-support phase I during TCG relative to the stance phase of NW because TCG involves more weight-shifting. Study of gait modification strategies show that increased toe-out consistently reduces late-stance EKAM. 18,24,25 This effect is likely due to a lateral shift in the center of pressure, which consequently reduces the EKAM lever arm; this would be most pronounced after mid-stance as the body progresses over the mid-foot. 26 An increased step width associated with TCG may also have contributed to reduction in peak EKAM. Increasing step width alters EKAM by lateralizing the center of pressure during foot contact, thus sequentially reducing the EKAM lever arm. 27 Thus, changes in the ground reaction force origin and vector positioning from the medial side of the knee joint to the lateral side likely reduced the EKAM lever arm. 17 Although TCG was performed at a slower speed than NW, the current results showed that speed difference did not affect the magnitude of the ground reaction force (GRF) with similar peak magnitude of GRF during TCG and NW (Fig. 5).
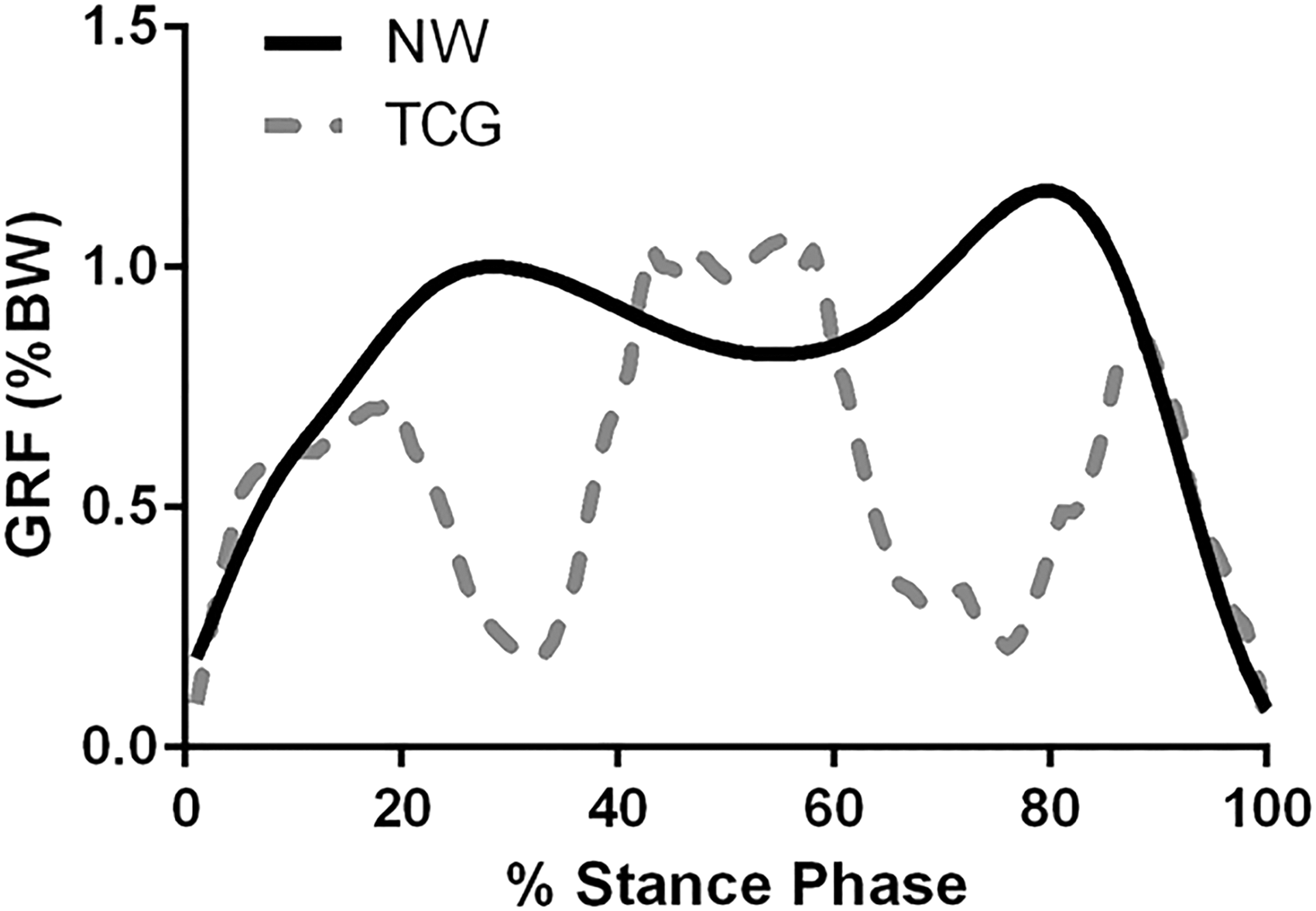
Time series of ground reaction force (GRF) normalized by body weight (BW) during stance phase of TCG and NW.
The results were supported by a recent study showing that the performance of TCG at slower speeds did not affect the peak amplitude of joint forces, moment, or GRF. 5 This suggests that the reduction of EKAM during TCC could be mainly contributed by EKAM lever arm. This reduction in EKAM illustrates an additional and beneficial exercise component of TCG that is critical in the reduction of peak EKAM during double-support phases I and II. In addition, although not analyzed statistically in this study, the frontal plane mechanical knee joint loading during the entire stance phase showed that the external knee abduction moment (EKABM) in TCG (0.249 ± 0.028 N · m/kg) was calculated and found to be greater than the external knee abduction moment in NW (0.067 ± 0.013 N · m/kg).
The external knee adduction moment during the stance phase was characterized by a tri-modal pattern during TCG. No significant difference was found between NW and TCG in peak EKAM during the entire stance phase, but the magnitude of the peak EKAM of TCG was actually higher than that of NW, particularly during single-limb support phase; the peak EKAM of TCG during the single-limb support phase was significantly higher than during the other two double-support phases. These findings indicate that the reduction of EKAM during TCG cannot last for the entire stance phase. It appears that TCG might be a feasible therapeutic intervention for producing less EKAM because of the reduction of peak EKAM during the double-support phases (i.e., stance phases I and II). However, the highest EAKM consistently demonstrated during the second peak EKAM value occurring during single-limb support phase draws great attention to the premise that regular t'ai chi practice does require higher mechanical demand of net muscular moment at the medial compartment of the knee joint. This could potentially indicate a biomechanical risk for detrimental effects on knee joint. Therefore, modification of peak EKAM during single-limb support phase of TCG would be much needed to reduce mechanical load of knee joint during TCC.
Limitations of this study include participants with experience performing yang-style TCC. The results of this study cannot be extrapolated to other forms of t'ai chi or individuals with different experience performing t'ai chi or nonpractitioners. Although EKAM is a surrogate indicator of medial loading response at the knee, the results lay the foundation of TCC mechanism of medial knee joint loading response as the first attempt, it would be helpful to estimate muscle forces around knee joint and how these muscle forces contributes to EKAM in the future studies.
Conclusion
In conclusion, this is the first study to demonstrate that peak EKAM was significantly lower for the TCG double-support phase I when compared with NW. This finding provides evidence of medial knee joint loading pattern of TCG. Whether this reduction would translate into clinically meaningful improvements for individuals with medial knee joint pathology is unknown. Future studies should examine the effects of TCG on the knee adduction moment, pain, and function in people with medial knee pathology.
Footnotes
Acknowledgments
This study was supported by University Faculty Development Council Research Grant (W. Liu, principal investigator). The authors thank Deana Rumble for her assistance with data collection.
Author Disclosure Statement
No competing financial interests exist.