
Abstract
Background:
Acute viral tonsillitis is an upper respiratory tract infection prevalent in school-aged children. Because this condition is self-limiting, conventional treatment options are usually palliative. Homeopathic remedies are a useful alternative to conventional medications in acute uncomplicated upper respiratory tract infections in children, offering earlier symptom resolution, cost-effectiveness, and fewer adverse effects. This study aimed to determine the efficacy of a homeopathic complex on the symptoms of acute viral tonsillitis in African children in South Africa.
Methods:
This was a randomized, double-blind, placebo-controlled, 6-day pilot study. Thirty children, age 6 to 12 years, with acute viral tonsillitis were recruited from a primary school in Gauteng, South Africa. Participants took two tablets of the medication four times daily. The treatment group received lactose tablets medicated with the homeopathic complex (Atropa belladonna D4, Calcarea phosphoricum D4, Hepar sulphuris D4, Kalium bichromat D4, Kalium muriaticum D4, Mercurius protoiodid D10, and Mercurius biniodid D10). The placebo consisted of the unmedicated vehicle only. The Wong-Baker FACES Pain Rating Scale measured pain intensity, and a Symptom Grading Scale assessed changes in tonsillitis signs and symptoms.
Results:
The treatment group had a statistically significant improvement in the following symptoms compared with the placebo group: pain associated with tonsillitis, pain on swallowing, erythema and inflammation of the pharynx, and tonsil size.
Conclusion:
The homeopathic complex used in this study exhibited significant anti-inflammatory and pain-relieving qualities in children with acute viral tonsillitis. No patients reported any adverse effects. These preliminary findings are promising; however, the sample size was small and therefore a definitive conclusion cannot be reached. A larger, more inclusive research study should be undertaken to verify the findings of this study.
Introduction
A
Homeopathy is a holistic system of medicine that aims to assist the body's own healing mechanisms. 8 Clinical trials have shown homeopathic treatment to be effective in preventing and treating upper respiratory tract infection in children, 9 –12 and suggest that it may provide an alternative treatment option to conventional drugs for children with acute uncomplicated infections. 13 These studies also found that homeopathic treatment is associated with fewer adverse effects, is more cost-effective, and induces earlier symptom resolution compared with conventional medicines. 12,13 Individualized homeopathic treatment involves the use of a single remedy to treat the totality of the symptoms of a patient, 14 whereas a complex is the combination of well-indicated remedies for a specific condition combined into one vehicle. 13,14 The homeopathic complex used in this study is commercially available in the South African market under the trade name Tonzolyt® and is marketed for the treatment of acute or chronic tonsillitis and pharyngitis. 15 It includes the following remedies: Atropa belladonna D4, Calcarea phosphoricum D4, Hepar sulphuris D4, Kalium bichromat (potassium dichromate) D4, Kalium muriaticum D4, Mercurius protoiodid D10, and Mercurius biniodid D10. The D (or Decimal) potency is created by diluting the crude substance in a 1:10 ratio (i.e., 1 part solute in 10 parts solvent, usually ethanol-water solution); each dilution is followed by succussions (vigorous shaking against a hard surface). 13 No research has yet addressed the efficacy of this complex in the treatment of acute viral tonsillitis in children.
Materials and Methods
This research study was approved by the Faculty of Health Sciences Higher Degrees Committee (HDC49/02-2011) and Academic Ethics Committee (AEC51/02-2011), who report to the National Health Research Ethics Council in South Africa. Participation in this study was subject to informed and signed consent from the parents or guardians, as well as the child's assent. Participants were free to withdraw from the study at any stage.
Research sample
Thirty participants, male and female, with acute viral tonsillitis, aged 6–12 years, were recruited from a primary school in Gauteng, South Africa, by means of purposive sampling. Participants had to be experiencing symptoms of viral tonsillitis (sore throat, pain on swallowing, erythema and/or edema of the tonsils, and enlarged or tender tonsillar and cervical lymph nodes), tonsillitis of recent onset (i.e., ≤2 days), and possible presence of exudates on the pharynx and tonsils. Any participant with a positive ARST result; diphtheria; otitis media; lymphadenopathy, except for the tonsillar and cervical lymph nodes; tonsillectomy; a medical history of rheumatic fever or glomerular nephritis; malabsorption syndrome; diseases that compromise breathing stridor (e.g., bronchitis, bronchopneumonia, or very enlarged tonsils); temperature >39°C; or HIV/AIDS were excluded from the study. Also excluded were any participants using long-term medication, immune stimulants (including homeopathic or herbal remedies), and/or antibiotic treatment during the previous 14 days or analgesic, antipyretic, or cold medications (e.g., decongestant, antihistamine, antitussive or throat lozenges) within the previous 8 hours.
Research design and procedure
This was a 6-day, double-blind, placebo-controlled pilot study with daily follow-up assessments. All children received a letter at the school and were instructed to give the letter to their parents or guardians. The letter informed them of the study and invited them to attend a meeting set up by the researcher to answer questions pertaining to the study. Attached to the letter was an information form, a participant profile form, and a consent form. Parents or guardians and teachers were requested to refer children reporting a sore throat or tonsillitis to the researcher. All consultations took place at the school in a private setting. At the first consultation, the researcher collected the signed consent form, and written or verbal assent was obtained from the child. The researcher assessed the participants' suitability for the study according to the inclusion and exclusion criteria. Any participant presenting with symptoms from the exclusion criteria would have been referred to his or her health care provider for treatment. The researcher took each participants' case, followed by a physical examination, which included vital signs (heart rate, respiratory rate, and temperature), and an ear, nose, throat, and chest examination. If a participant demonstrated symptoms suggestive of group A streptococcal tonsillitis, an ARST would have been performed, to confirm this diagnosis, and they would have been excluded from the study.
Participants were divided into two groups, with 15 in the treatment group and 15 in the placebo group. The homeopathic complex and placebo were manufactured and sold by a registered homeopathic pharmaceutical company that assured quality control of medication preparation. Assignment to medication or placebo was randomized by an outside party using the simple random sampling method, and the participants received one bottle containing 48 tablets of the homeopathic complex medicated onto lactose tablets or unmedicated lactose tablets. The placebo was similar in appearance and taste and was labeled in the same manner as the treatment medication. Each participant was given instructions to dissolve two tablets four times a day under their tongue (after breakfast, lunch, and supper and before bedtime), and the first dose was administered by the researcher. Each child received an information leaflet detailing the dosage and storage instructions. The participants attended daily follow-up assessments for 5 days. The researcher was granted permission and access to use the school premises for follow-up consultations both during the week and on the weekends. At each consultation, participants completed the Wong-Baker FACES Pain Rating Scale and a Symptom Grading Scale (SGS), under the supervision of the researcher, and a relevant physical examination was performed.
The Wong-Baker FACES Pain Rating Scale was used to measure pain associated with tonsillitis. This recognized, valid, and reliable tool is used for assessing pain, especially in children aged 4–7 years or older; young patients may not yet be adept with numeric scales but are able to easily relate their pain to facial expressions. 16 The SGS was used to grade tonsillar hypertrophy and erythema/inflammation of the pharynx. The researcher also determined the presence of associated ear pain and pain on swallowing using the SGS.
Statistical analysis
Because of the small sample size, nonparametric tests were used (SPSS software, version 18.0; SPSS, Inc., Cary, NC), namely the Mann-Whitney U test (to compare the results between groups) and the Friedman and Cochran tests (for intragroup analysis). For the purposes of this study, a p-value <0.05 was considered to represent a statistically significant difference. To measure the strength of the relationship between two variables in the placebo and treatment groups, the r or effect size was calculated. 17 For the Mann-Whitney test, r=z/square root of (N), where z is the statistic from the Mann-Whitney test and N is the combined sample size of the two groups. To interpret the r value, the following criteria were used: 1=small effect (0.01–0.2 or 1%), 3=medium effect (0.06–0.5 or 6%), and 5=large effect (0.138–0.8 or 13.8%). 18
Results
Thirty participants were recruited for this study. They all met the inclusion criteria, and all 30 completed the study. No participants were excluded, referred to a health care provider, or withdrew from the study. No participants presented with tonsillitis suspected of being caused by group A streptococcus (high temperature [>39°C] and presence of profuse exudates on the pharynx or tonsils); therefore, the ARST was not carried out. The study took place between October 2011 and March 2012, during the spring/summer.
Demographic analysis
With regard to gender distribution, 46.7% of the treatment group and 26.7% of the placebo group were male. All participants were African, were 6–12 years of age, and were distributed across this age range. The mean age for the placebo group was 8.07 years (mean rank, 14.93) and for the treatment group was 8.33 years (mean rank, 16.07). Age did not significantly differ between the placebo and the treatment groups (U=104.000; p=0.744; z=−0.358). Table 1 demonstrates the demographic data and initial baseline readings of the participants.
Values expressed with a plus/minus sign are the mean±standard deviation. All other values are the number (percentage) of patients.
Data obtained from the Wong-Baker FACES Pain Rating Scale.
Data obtained from the Symptom Grading Scale.
Wong-Baker FACES Pain Rating Scale: pain associated with tonsillitis
Intra-group analysis
Pain was relatively high at day 1 for both the placebo and treatment groups, with the placebo group averaging 6.40±2.4 (standard deviation [SD]) and the treatment group averaging 5.87±3.07 (Fig. 1). By day 6 the average pain rating for the treatment group was 1.6±2.03. According to the Friedman test, this decrease in average pain rating by day 6 was highly statistically significant (chi-square=32.6; p<0.001; df=5). By day 6 the average pain rating for the placebo group was 5.2±3.0). This apparent difference in average pain rating was not statistically significant (chi-square=9.5; p=0.091; df=5).
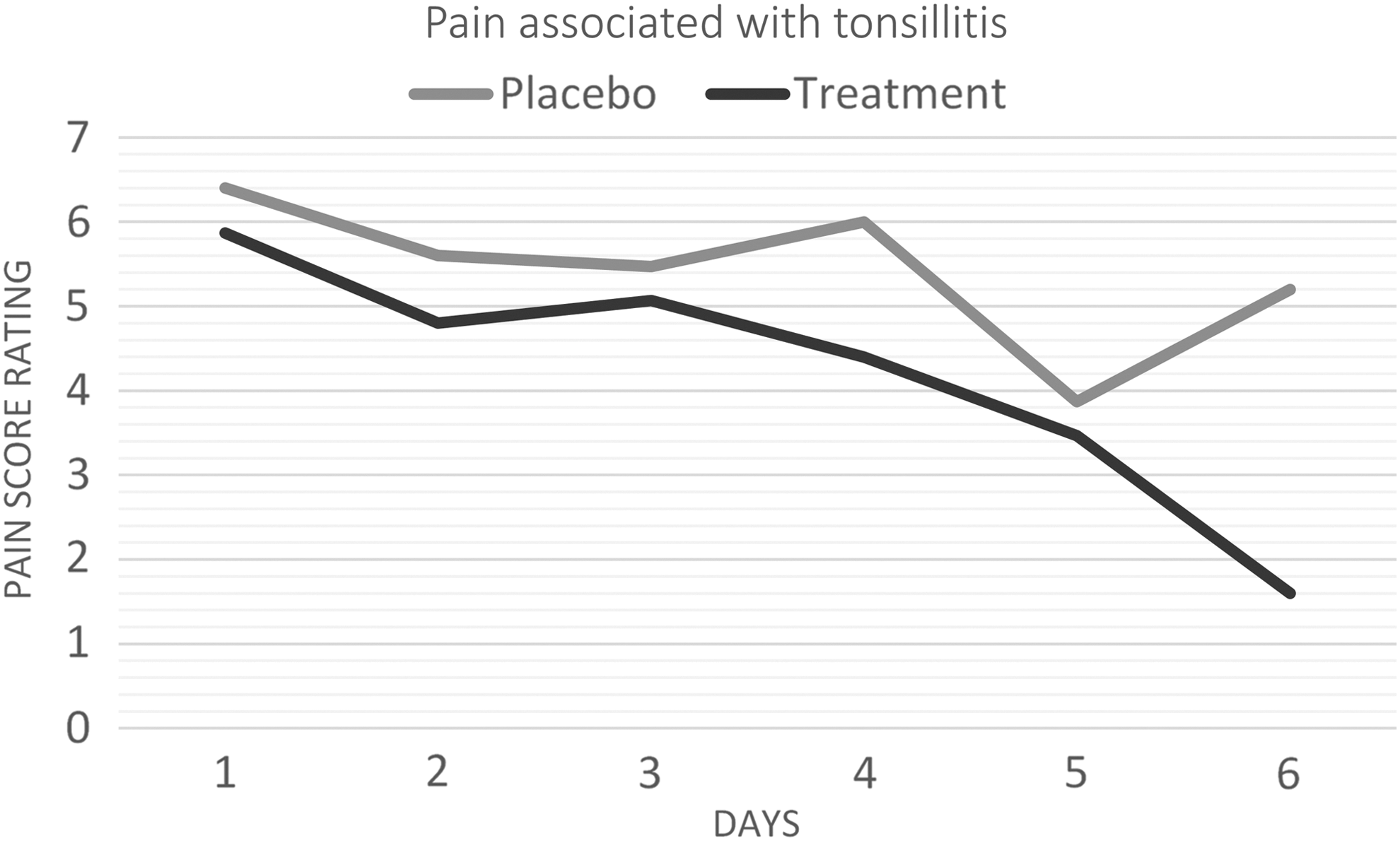
The mean score rating for pain associated with tonsillitis.
Intergroup analysis
Average pain rating did not differ between groups at day 1 (U=101.500; p=0.653; z=−0.468), indicating that the two groups were similar at the start of the study. By day 6, there was a statistically significant difference in average pain rating between the treatment and placebo groups (U=38.000; p=0.001; z=−3.175). This difference had a large effect size (r=0.8).
SGS: erythema/inflammation of the pharynx
The red/inflamed pharynx was measured in ordinal categories: absent (code 0), slightly red (code 2), red (code 4), very red (code 6), severely red (code 8), and extremely red (code 10).
Intragroup analysis
According to Figure 2, mean values for the degree of inflammation of the pharynx at day 1 were 4.53±2.07 and 4.0±1.85 for placebo and treatment groups, respectively. Both groups showed a statistically significant decrease by day 6, with the treatment group decreasing to 0.67±0.98 (chi-square=39.3; p<0.001; df=5), and the placebo group decreasing to 1.87±1.07 (chi-square=27.4; p=0.001; df=5).

The mean score rating for red/inflamed pharynx.
Intergroup analysis
Although degree of inflammation of the pharynx did not significantly differ at day 1 (U=94.5; p=0.433; z=−0.784), indicating that the two groups were similar, by day 6 there was a statistically significant difference in favor of the treatment group (U=62.500; p=0.037; z=−2.322). This difference had a large effect size (r=0.6).
Tonsil size
Tonsil size was measured as ordinal categories: absent (code 0), small (code 2), average (code 4), moderate enlarged (code 6), and severely enlarged (code 8).
Intragroup analysis
Average tonsil size was similar for the placebo (mean score, 5.20±1.265) and treatment (mean score, 5.33±1.45) groups at day 1 (Fig. 3). Both groups showed a statistically significant decrease in average tonsil size by day 6, with the treatment group decreasing to a score of 2.00±1.07 (chi-square=55.2; p<0.001; df=5) and the placebo group decreasing to a score of 4.27±1.83 (chi-square=20.1; p=0.001; df=5).
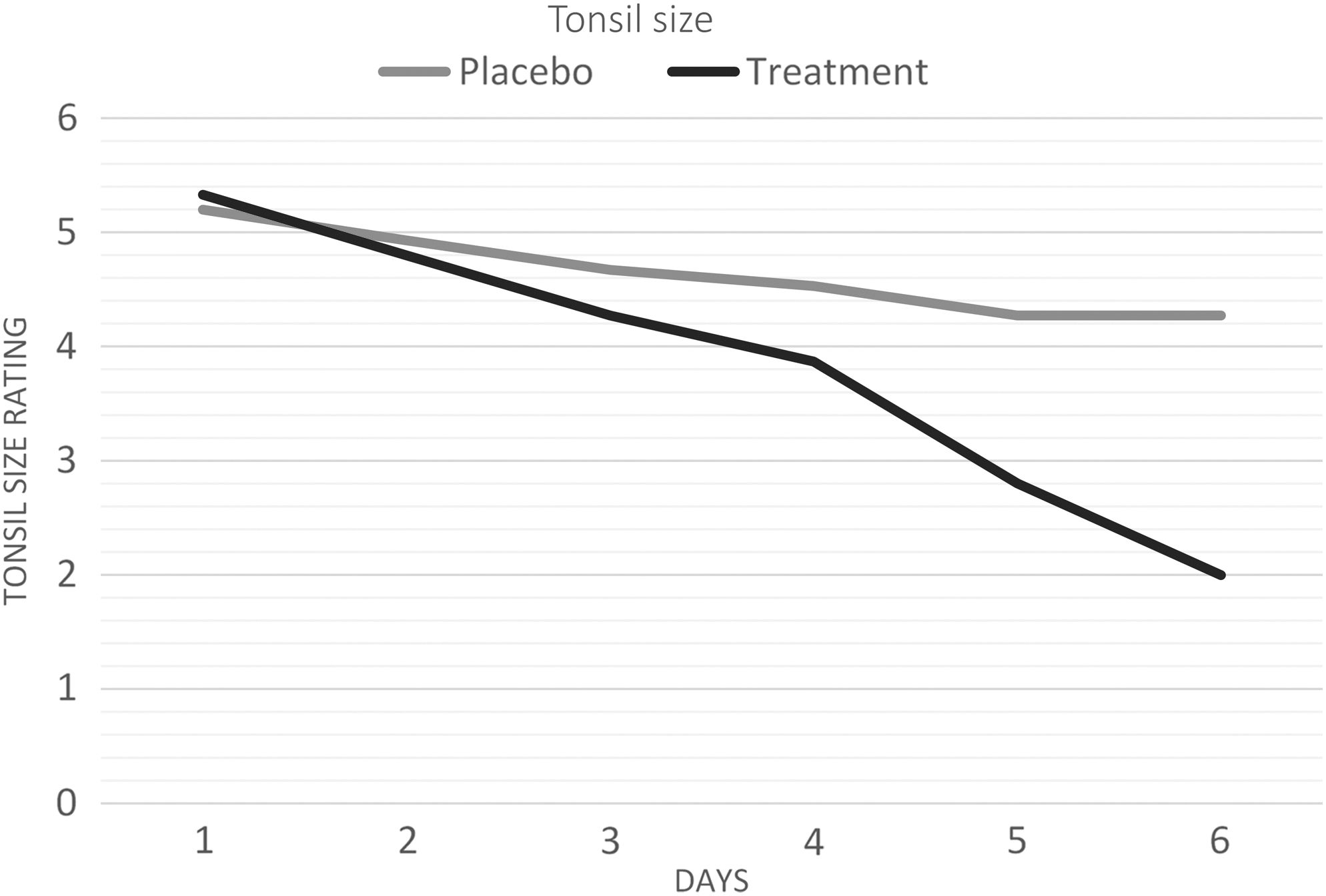
The mean score rating for tonsil size.
Intergroup analysis
While average tonsil size did not significantly differ at day 1 (U=108.500; p=0.870; z=−0.184), by day 6 of the study, the difference in the mean tonsil size was statistically significant in favor of the treatment group (U=35.000; p=0.001; z=−3.404) and of a large effect size (r=0.6).
Pain on swallowing
Pain on swallowing was measured by using dichotomous categories: pain (code 1) and no pain (code 2); therefore, the Cochran Q test was used for statistical inference.
Intragroup analysis
Both the placebo (n=14 [93.3%]) and treatment (n=13 [86.7%]) groups had a large number of participants with pain at day 1 (Fig. 4). By day 6, the treatment group had shown a statistically significant decrease in the number of participants with pain on swallowing (n=2) (Q=27.3; p<0.001; df=5). In contrast, although the number of participants experiencing pain on swallowing in the placebo group had decreased to 10 by day 6, this apparent decrease was not statistically significant (Q=7.647; p=0.177; df=5).
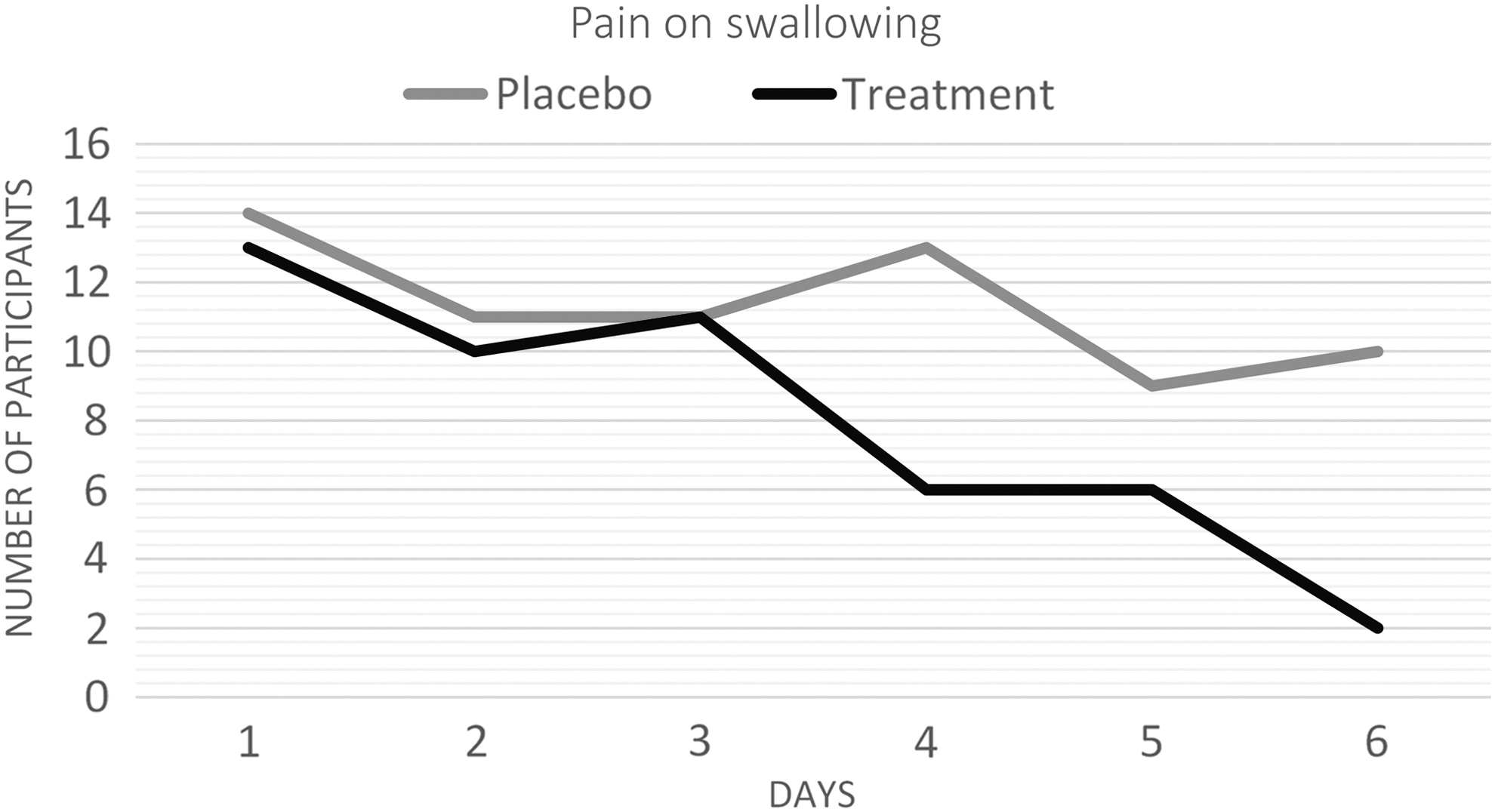
The number of participants experiencing pain on swallowing.
Referred ear pain
Ear pain was measured by using dichotomous categories: pain (code 1) and no pain (code 2); therefore, the Cochran Q test was used for statistical inference.
A few participants in both the placebo (n=4 [26.7%]) and the treatment (n=5 [33.3%]) groups reported ear pain at day 1 (Fig. 5). Although the number of participants with ear pain dropped from 5 to 1 in the treatment group, this did not constitute a statistically significant change (Q=8.095; p=0.151; df=5). In contrast, in the placebo group, the number of participants with ear pain increased from 4 to 10, which indicates a statistically significant deterioration in this symptom (Q=11.420; p=0.044; df=5).
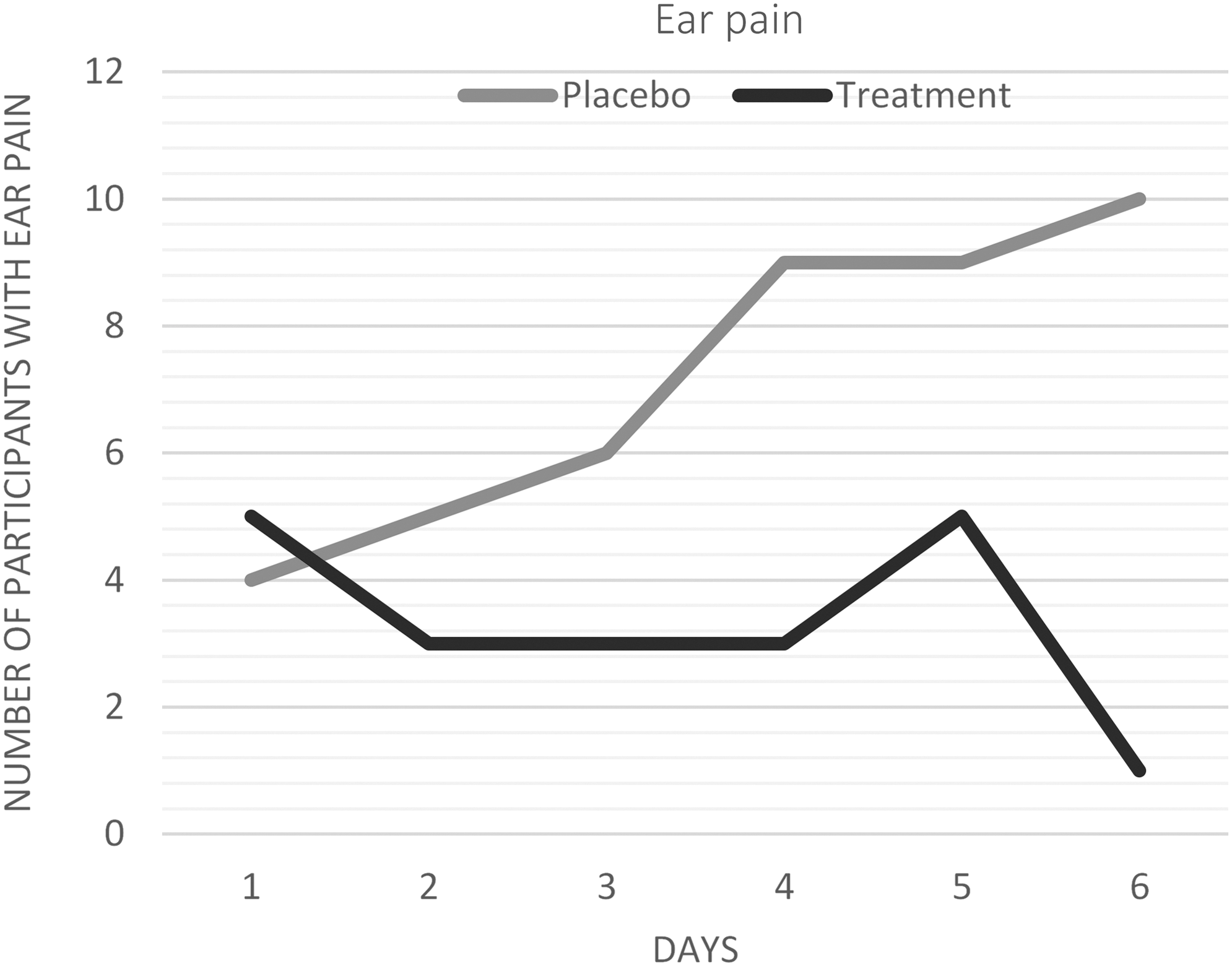
The number of participants experiencing referred ear pain.
Vital signs
Temperature, respiratory rate, and heart rate were measured at each consultation and provide objective parameters of measurement.
Temperature
Normal reference range auricular temperature readings for this age group are between 35.8°C and 38°C. 19 The mean temperature readings for both groups were similar at the start of the study (Table 1) and within normal range, with the exception of one participant in the treatment group with a temperature of 39°C. By day 2, however, this participant's temperature had decreased to 37.8°C. The Friedman test revealed no statistically significant change over time for the treatment group, decreasing from a mean reading of 37.3°C to 36.9°C (SD, 0.3283) (chi-square=9.091, p=0.105; df=5). The placebo group showed a statistically significant decrease over time from 37.3°C to 36.7°C (standard deviation, 0.6278) (chi-square=11.595; p=0.041; df=5). The Mann-Whitney test, however, revealed no statistically significant difference between the groups on day 1 (U=108.000; p=0.851; z=−0.187) or day 6 (U=87.500; p=0.296; z=−1.045).
Respiratory rate (RR)
The normal reference range for RR in this age group is 18 to 30 breaths/min. 20 The mean RRs for both groups were similar at the start of the study (Table 1) and were within normal range. The Friedman test revealed no statistically significant change over time for either group, with the treatment group increasing slightly from a mean reading of 20 to 21 breaths/min (standard deviation, 2.236) (chi-square=6.166; p=0.290; df=5), and the placebo group decreasing slightly from 21 to 20 breaths/minute (standard deviation, 2.849) (chi-square=5.809; p=0.325; df=5). The Mann-Whitney test also revealed no statistically significant difference between the groups on day 1 (U=82.500; p=0.210; z=−1.254) or day 6 (U=103.000; p=0.690; z=−0.399).
Heart rate (HR)
The normal reference range for HR in this age group is 70 to 120 beats/min. 21 The mean HRs for both groups were similar at the start of the study (Table 1) and were within normal range. The Friedman test revealed no statistically significant change over time for the placebo group, with the mean reading increasing slightly from 83.93 to 86.40 beats/min (standard deviation, 9.417) (chi-square=7.404; p=0.192; df=5), while the treatment group showed a statistically significant increase from 82.67 to 87.33 beats/min (standard deviation, 8.409) (chi-square=13.185; p=0.022; df=5). The Mann-Whitney test, however, revealed no statistically significant difference between the groups on day 1 (U=107.00; p=0.818; z=−0.230) or day 6 (U=92.000; p=0388; z=−0.864).
Discussion
The purpose of this study was to determine the efficacy of a homeopathic complex (Tonzolyt®) in the treatment of the symptoms of acute viral tonsillitis in children attending a primary school in Gauteng, South Africa. The remedies in this complex are clinically indicated for acute tonsillitis and its associated signs and symptoms. A. belladonna is indicated for inflammation of the tonsils that is worse for touch of the throat and worse on the right-hand side. It is also used to treat fever, where the patient experiences a dry mouth and a lack of thirst. C. phosphoricum is indicated for tonsillar edema with burning pain that is worse for swallowing. K. bichromat is used to treat tonsillitis with sharp pains that radiate to the ears. Throat symptoms are usually accompanied by pseudomembranous deposits on the tonsils and soft palate. K. muriaticum is used for tonsillitis accompanied by enlarged submaxillary and cervical lymph nodes and pain on swallowing. M. protoiodid is indicated for tonsillar pain on the right side with swelling of the cervical lymph nodes, while M. biniodid is for left-sided tonsillar pain with fever. 21
The symptoms and signs of acute viral tonsillitis (namely pain associated with tonsillitis, erythema/inflammation of the pharynx, and tonsil size) showed a statistically significant improvement over the 6-day study period. Analysis between groups showed that the homeopathic complex outperformed placebo, with a large effect size. The associated symptom of pain on swallowing also significantly improved over time, while the placebo group did not. With regard to ear pain, although the number of participants in the treatment group with ear pain dropped from 5 to 1, this did not constitute a statistically significant change because of the small sample size. In contrast, in the placebo group, the number of participants with ear pain actually increased from 4 to 10, which was a statistically significant change. During the follow-up consultations, the participant's ears were checked daily to eliminate the possibility of pathology, such as otitis media, as a cause for ear pain. Because the ear pain was not being caused by ear-associated pathology, the likely cause was referred pain from the pharynx. Most participants did not present with pyrexia or abnormal heart or respiratory rates, and therefore these variables were unlikely to change over time. None of the participants reported using antipyretics or any other treatment (conventional or otherwise) for the duration of the study.
The statistical analysis showed that the tonsillitis symptoms in the treatment group improved between day 5 and day 6, after the commencement of the treatment, while those in the placebo group showed less improvement. Viral tonsillitis typically lasts for 7 days. 2 The results of this study suggest that using this homeopathic complex may reduce the duration of acute viral tonsillitis by up to 2 days.
The homeopathic complex used in this study consisted of remedies in a very low potency, in repeated doses, which may have had a more physiologic effect on the body than higher potencies. Other potencies of these remedies may produce different effects in children with tonsillitis, and this could be explored in future studies.
Internal validity of the study was maintained because of the randomized, double-blind, placebo-controlled design. A few limitations may have affected the results of this study. Most studies indicate that female children are more prone to tonsillitis than are males. 22 This variable was not controlled for in the study, and therefore it is difficult to assess the effect it may have had on the results. The sample size used in this study was small, and a larger sample group could yield more statistically reliable results. The population used was taken from a single source and demographic group. Future studies could include children from other ethnic groups; other studies could also choose one gender to study or place participants into matched pairs to eliminate this possible confounding variable. The complex was well tolerated, and no adverse effects were reported by any of the participants. The complex used in this study could provide a possible treatment option for children with acute viral tonsillitis.
Conclusion
This small pilot study concludes that the homeopathic complex used in this study significantly reduced common signs and symptoms associated with acute viral tonsillitis in African children, relieving pain and reducing throat inflammation and tonsil size. The complex was well tolerated, and no adverse effects were reported. Although the results are promising, further research is warranted before any definitive conclusions can be drawn.
Footnotes
Acknowledgments
The authors would like to thank Dr. Richard Devey for his assistance with the statistical analysis.
Author Disclosure Statement
No competing financial interests exist.