
Abstract
Introduction:
Numerous people with chronic conditions like to use traditional Chinese medicine (TCM) treatment, or integrated treatment of TCM and Western medicine (WM). Our study explored the associations between multiple chronic conditions (MCC) and TCM use and the use of specific types of TCM therapy among adults in Taiwan. In addition, we explored the TCM use of adults with seven common types of chronic conditions.
Methods:
In our study, a national representative sample in 2005 was used. The Chronic Condition Indicator and the Clinical Classifications System created by the U.S. Agency for Healthcare Research and Quality were used to define the number of chronic conditions of adults. Logistic regressions adjusted for demographic characteristics were used to analyze the associations. The frequency of TCM use among adults with different numbers of chronic conditions was quantified.
Results:
TCM use for adults with ≥5 chronic conditions (odds ratio [OR] 1.86) was higher than TCM use for adults with 2–4 chronic conditions (OR 1.51) and TCM use for adults with one chronic condition (OR 1.48). The increase in the OR of the use of Chinese herbs and traumatology manipulative therapy according to the number of chronic conditions was not as substantial as that of acupuncture–moxibustion. The frequency of TCM use exhibited an increasing trend with the increase in the number of chronic conditions (p<.001). Among the seven common types of chronic conditions for adults, TCM use for adults with arthropathy (OR 2.01) was the highest.
Conclusion:
The probability and frequency of TCM use increased as the number of chronic conditions increased. The probability of Chinese herbs use, traumatology manipulative therapy use, and, particularly, acupuncture–moxibustion use increased as the number of chronic conditions increased. We suggest that government policy makers emphasize administering integrated TCM and WM care to people with chronic conditions or MCC.
Introduction
T
The use of complementary and alternative medicine (CAM) is high and has gradually increased in some countries. In the United States, CAM use among adults increased from 33.8% in 1990 to 42.1% in 1997, 6 and 67.7% of these adults had used at least one type of CAM therapy in their lifetime. 7 CAM use is popular among people with chronic conditions. A high percentage of CAM use (63.9%) was observed among adults with chronic conditions in Malaysia. 8 Adults with MCC were more likely to use CAM than those with no or one chronic condition in the United States. 9 Traditional Chinese medicine (TCM) is a type of CAM. The history of TCM use spans more than 2500 years. TCM is popular in Asian countries, 8,10 –12 and TCM therapies, particularly acupuncture, are commonly used in certain Western countries. 13 –15 In Taiwan, the government has implemented the National Health Insurance (NHI) program to cover the healthcare costs of residents since 1995. In 2005, nearly 99% of the population (23 million people) was covered by the NHI program. The NHI program covers WM and TCM costs. Although the major medical system remains WM, residents can choose WM, TCM, or combined WM and TCM to treat their diseases. Using TCM is popular, and approximately 28% and 63% of the insured people used TCM in 2001 and 1996–2001, respectively. 16 In the NHI system, TCM is divided into Chinese herbs, acupuncture–moxibustion, and traumatology manipulative therapy (including tui na, cupping, plaster application, and reset dislocation). Only licensed TCM physicians are reimbursed by the Bureau of NHI.
Patients with chronic conditions like to use TCM in certain countries, particularly Asian countries. Numerous people with chronic conditions like TCM treatment or integrated treatment of TCM and WM. 8,17 Most Chinese people believe that TCM is suitable for treating chronic conditions because of its focus on the causes of diseases. 17 In addition, TCM therapies facilitate relieving the discomfort of chronic diseases, because they enhance the physical energy of patients with chronic conditions and improve their strength. 18 People with more chronic conditions usually have poorer health. The reasons for the use of CAM include poorer health status and the need for personal control in healthcare decisions. 9,19 TCM is the major type of CAM in Taiwan. Hence, we want to explore whether the number of chronic conditions is positively associated with TCM use in Taiwan. Moreover, we knew that people with more chronic conditions usually use more WM medical services and have higher WM medical expenditures. 5,20 Whether people with more chronic conditions exhibit a higher frequency of TCM use in Taiwan has not been confirmed. The results can serve as a reference in integrating WM and TCM to treat people with chronic conditions or MCC in Taiwan.
Therefore, we explored the associations between MCC and TCM use and the use of specific types of TCM therapy (Chinese herbs, acupuncture–moxibustion, and traumatology manipulative therapy) among adults enrolled in the NHI in Taiwan. This study also explored the TCM use of adult patients with seven common chronic conditions, namely, cancer, diabetes, hypertension, heart disease, stroke, chronic obstructive pulmonary disease (COPD) or asthma, and arthropathy, which are highly prevalent in Taiwan, and treatment for these conditions is costly in Taiwan. 21
Methods
Data sources
Our study used the Longitudinal Health Insurance Database 2005 (LHID 2005), which is a part of the National Health Insurance Research Database (NHIRD) released by the National Health Research Institutes in 2007. The NHIRD was established for academic research. To ensure privacy, the identities of patients, institutions, and physicians were scrambled cryptographically in the NHIRD. The LHID 2005 contains claims data on 1 million people who were randomly sampled from the insured people enrolled in the NHI program in 2005. The LHID 2005 is a representative database. No statistically significant difference in age, gender, and insurance amount of the insured people was observed between the LHID 2005 and the original NHI 2005 database. 22 The LHID 2005 provides numerous data, such as information on each patient's gender, date of birth, insurance amount, and geographic area of residence; diagnoses; department of visit; medical cost; medication prescribed; and item of treatment.
Study sample
People aged <18 years (n=205,523), those for whom data on demographic characteristics (age, gender, insurance amount, geographic region) were incomplete (n=33), and those who were not continuously enrolled in the NHI program in 2005 (n=44,948) were excluded. A total of 749,496 enrollees were subjected to analysis of the associations between MCC and TCM use and the use of specific types of TCM therapy (Chinese herbs, acupuncture–moxibustion, and traumatology manipulative therapy) in 2005.
Operational definition of chronic conditions
We used the Chronic Condition Indicator (CCI) created by the U.S. Agency for Healthcare Research and Quality (AHRQ) to categorize the ICD-9-CM diagnosis codes into two categories: chronic and nonchronic. A chronic condition is defined as a condition that lasts 12 months or longer and results in functional limitations or requires ongoing medical care. The CCI was created to facilitate health service research on diagnoses conducted using administrative data. 23 To determine the number of chronic conditions per person, we adopted the following procedures. First, we excluded nonchronic ICD-9-CM diagnoses in ambulatory and inpatient WM care visits covered by NHI using CCI. Second, we used the Clinical Classifications System (CCS), which was also created by AHRQ, to aggregate the chronic ICD-9-CM codes into mutually exclusive clinical categories. 24 Third, a person who had a chronic condition at three or more ambulatory care visits or at least one inpatient care visit was defined as having a chronic condition in our study. Finally, we counted the number of chronic conditions per person. In addition, seven common chronic conditions, namely, cancer, diabetes, hypertension, heart disease, stroke, COPD or asthma, and arthropathy, were identified from CCS category in our study (Appendix Table A1). 24
Measures
Independent variables
Demographic characteristics, including age, gender, socioeconomic status (SES), region of residence, and urbanicity, were obtained from the NHI database. Age was classified into six categories: 18–29, 30–39, 40–49, 50–64, 65–74, and ≥75 years. We used the insured wage (amount) as a proxy for the SES. The insurance premiums of family dependents were attached to the head of the family. We classified people with a well-defined monthly wage into three categories: <US$640, US$640–1,279, and ≥US$1,280, and those without a well-defined monthly wage were classified into two categories: farmers and fishermen, and others, including veterans, low-income people, and those enrolled in the NHI through local government offices. 25 Region of residence was classified into four categories: Northern Taiwan, Central Taiwan, Southern Taiwan, and Eastern Taiwan. Urbanicity was classified into three categories: urban, suburban, and rural. 26
The number of chronic conditions per person in 2005 was classified into four categories: 0, 1, 2–4, and ≥5. In addition, the patients were divided into groups according to whether they had chronic conditions and whether they had MCC in 2005. Furthermore, the patients were classified according to whether they had cancer, diabetes, hypertension, heart disease, stroke, COPD or asthma, arthropathy, other chronic conditions, and nonchronic conditions in 2005.
Dependent variables
People who had used TCM, Chinese herbs, acupuncture–moxibustion, or traumatology manipulative therapy at least once in 2005 were considered users of these treatments. The mean frequency of TCM use among adults with different number of chronic conditions in 2005 was determined.
Statistical analysis
Differences in the use of TCM, Chinese herbs, acupuncture–moxibustion, or traumatology manipulative therapy elicited by each independent variable were assessed using a χ 2-test. The p-values were estimated. Logistic regressions adjusted for demographic characteristics were used to analyze the associations between MCC and TCM use and the use of specific types of TCM therapy. Adjusted odds ratio (OR) were estimated. Differences and linearity in the mean frequency of TCM use by people with different number of chronic conditions were assessed using an ANOVA with a linearity test. All statistical tests were two-sided and the significance level was set at 0.05. SAS Version 9.2 (SAS Institute Inc., Cary, NC) was used to manage and analyze the data.
Results
To study the association between MCC and TCM use among adults, we used adult (n=749,496) users of NHI-covered services in 2005 as our study sample. Table 1 shows the characteristics of TCM use among adults. A total of 231,106 (30.8%) adults used TCM among adults in 2005. The results regarding the associations between MCC and TCM use are listed in Table 2. Logistic regressions adjusted for the demographic characteristics of adults, including age, gender, insured amount, region of residence, and urbanicity, were used to produce the results shown in Table 2. TCM use for adults with chronic conditions (OR 1.52, 95% confidence interval [CI] 1.51–1.54) was higher than that for adults without chronic conditions.
COPD, chronic obstructive pulmonary disease; SES, socioeconomic status; TCM, traditional Chinese medicine.
Association studies were adjusted for age, gender, SES, geographic region, and urbanicity.
95% CI, 95% confidence interval; OR, odds ratio; SES, socioeconomic status.
TCM use for adults with MCC (OR 1.43, 95% CI 1.41–1.45) was higher than that for adults without MCC. TCM use for adults with ≥5 chronic conditions (OR 1.86, 95% CI 1.81–1.91) was higher than the TCM use for adults with 2–4 chronic conditions (OR 1.51, 95% CI 1.49–1.53) and TCM use for adults with one chronic condition (OR 1.48, 95% CI 1.46–1.50). The OR of TCM use for adults with cancer was 1.41 (95% CI 1.36–1.48), the OR of TCM use for adults with diabetes was 1.29 (95% CI 1.26–1.32), the OR of TCM use for adults with hypertension was 1.34 (95% CI 1.31–1.36), the OR of TCM use for adults with heart disease was 1.50 (95% CI 1.47–1.54), the OR of TCM use for adults with stroke was 1.30 (95% CI 1.25–1.35), the OR of TCM use for adults with COPD or asthma was 1.59 (95% CI 1.54–1.64), the OR of TCM use for adults with arthropathy was 2.01 (95% CI 1.97–2.05), and the OR of TCM use for adults with other types of chronic conditions was 1.56 (95% CI 1.53–1.58). Figure 1 shows the frequency of TCM use by adults according to the number of chronic conditions. A linear increasing trend was found in the frequency of TCM use in relation to the number of chronic conditions (p<.001).
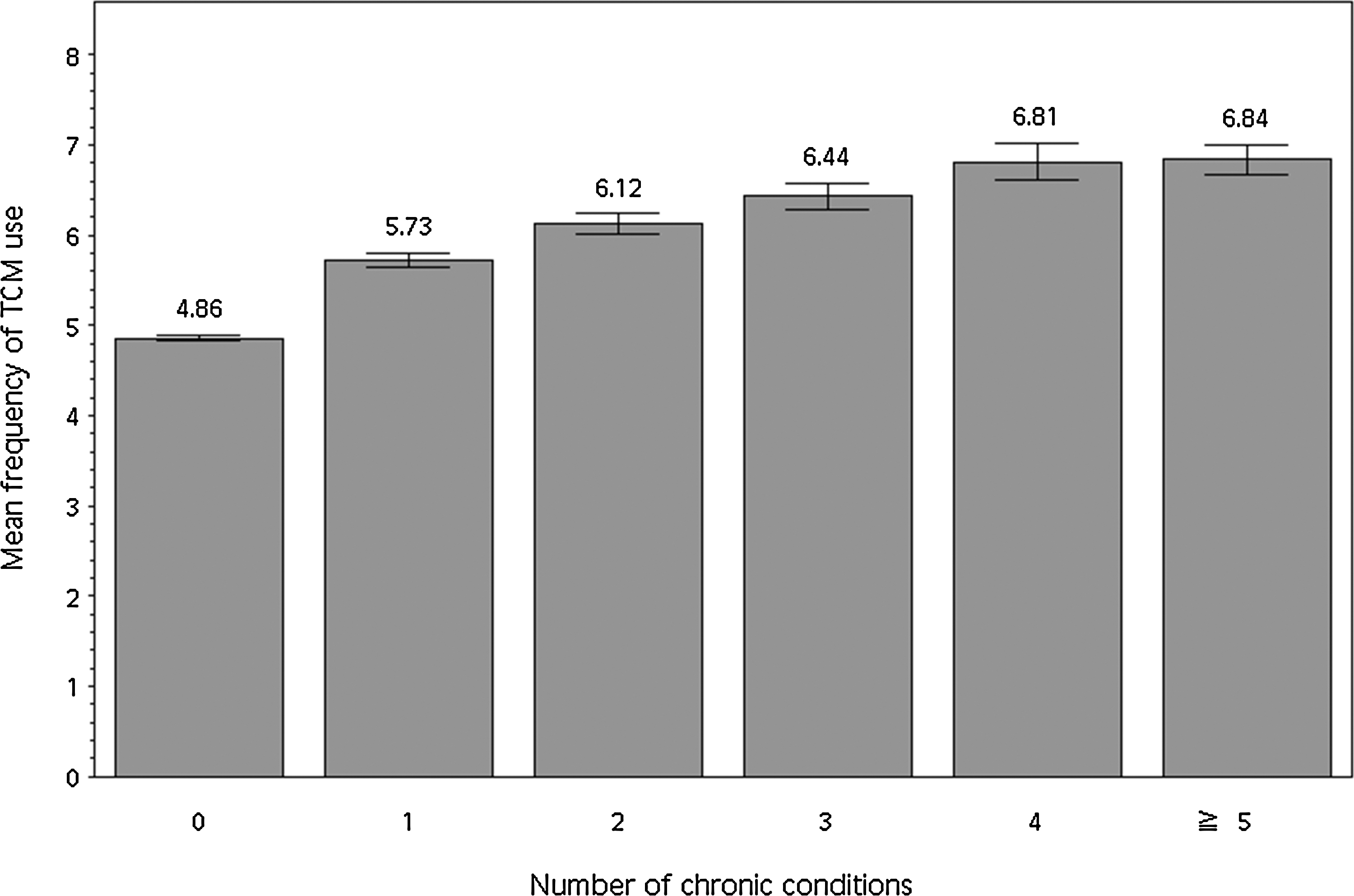
The mean frequency (mean, 95% confidence interval) of traditional Chinese medicine use among adults with different numbers of chronic conditions in 2005.
In addition, we studied the associations between MCC and the use of specific types of TCM therapy among adults. Table 3 shows the characteristics of Chinese herbs use, acupuncture–moxibustion use, and traumatology manipulative therapy use among adults in 2005. Chinese herbs was the most likely to be used type of TCM (24.9%), followed by traumatology manipulative therapy (11.6%) and acupuncture–moxibustion (6.6%), among 749,496 adults in 2005.
The results regarding the associations between MCC and the use of Chinese herbs, acupuncture–moxibustion, and traumatology manipulative therapy are listed in Table 4. Logistic regressions adjusted for the demographic characteristics of adults, including age, gender, insured amount, region of residence, and urbanicity, were used to obtain the results shown in Table 4. The use of Chinese herbs (OR 1.50, 95% CI 1.48–1.52), the use of acupuncture–moxibustion (OR 1.62, 95% CI 1.59–1.65), and the use of traumatology manipulative therapy (OR 1.44, 95% CI 1.42–1.46) for adults with chronic conditions were higher than those for adults without chronic conditions. Similarly, the use of Chinese herbs (OR 1.40, 95% CI 1.38–1.42), the use of acupuncture–moxibustion (OR 1.63, 95% CI 1.59–1.67), and the use of traumatology manipulative therapy (OR 1.38, 95% CI 1.36–1.41) for adults with MCC were higher than those for adults without MCC. Moreover, the OR of the use of Chinese herbs, acupuncture–moxibustion, and traumatology manipulative therapy gradually increased as the number of chronic conditions increased.
Association studies were adjusted for age, gender, SES, geographic region, and urbanicity.
The use of acupuncture–moxibustion for adults with ≥5 chronic conditions (OR 2.36, 95% CI 2.26–2.46) was significantly higher than that for adults with 2–4 chronic conditions (OR 1.67, 95% CI 1.63–1.72) and that for adults with one chronic condition (OR 1.46, 95% CI 1.43–1.50). The use of Chinese herbs for adults with ≥5 chronic conditions (OR 1.76, 95% CI 1.71–1.81) was higher than that for adults with 2–4 chronic conditions (OR 1.49, 95% CI 1.47–1.52) and that for adults with one chronic condition (OR 1.46, 95% CI 1.44–1.49). The use of traumatology manipulative therapy for adults with ≥5 chronic conditions (OR 1.75, 95% CI 1.68–1.81) was higher than that for adults with 2–4 chronic conditions (OR 1.44, 95% CI 1.41–1.48) and that for adults with one chronic condition (OR 1.39, 95% CI 1.36–1.42). The increase in the OR of the use of Chinese herbs and traumatology manipulative therapy according to the number of chronic conditions was not as substantial as that of acupuncture–moxibustion.
Discussion
This study is the first population-based study to explore the association between MCC and TCM use among adults in Taiwan. The results indicated that TCM use by adults with chronic conditions or MCC was higher than that by adults without chronic conditions or without MCC, respectively. Other reports have also indicated that TCM use by adults with chronic conditions was higher than that by adults without chronic conditions. 11,27,28 However, these studies examined only some types of chronic conditions and did not discuss the association between MCC and TCM use. In addition, TCM was more likely to be used and was used at a higher frequency by adults with more chronic conditions in our study. Furthermore, we investigated seven common chronic conditions, namely, cancer, diabetes, hypertension, heart disease, stroke, COPD or asthma, and arthropathy. The results indicated that adults with arthropathy were the most likely to use TCM, followed by those with COPD or asthma, other types of chronic conditions, and heart disease.
Adults with diabetes were the most unlikely to use TCM. We suggest that TCM consultation or therapy incorporate into healthcare programs for people with chronic conditions in WM in Taiwan. In addition, we examined the association between MCC and the use of specific types of TCM therapy (Chinese herbs, acupuncture–moxibustion, and traumatology manipulative therapy). The results indicated that the use of specific types of TCM therapy by adults with chronic conditions or MCC was higher than that by adults without chronic conditions or without MCC, respectively. Moreover, the use of Chinese herbs, traumatology manipulative therapy, and, particularly, acupuncture–moxibustion became more likely as the number of chronic conditions increased. According to our clinical observations, because people with MCC typically must take many Western medications daily, most of them worry about the interaction between additional Chinese herbs and Western medications. These people also worry that the use of additional Chinese herbs will increase the workload of their liver or kidney. Hence, they usually ask TCM physicians for treatment using methods other than Chinese herbs in TCM outpatient services. Although Chinese herbs are natural and beneficial to health, some side effects may still exist. 29
Acupuncture–moxibustion has fewer side effects than Chinese herbs do when the trained physicians administer the treatments carefully. 29 These facts might explain the increased higher OR of acupuncture–moxibustion use compared with OR of Chinese herbs use for people with higher numbers of chronic conditions. However, the suspected causes should be verified.
We excluded people who were not continuously enrolled in the NHI system in 2005 in order to quantify the number of people with chronic conditions accurately. The size of our studied sample was sufficient. We used the CCI and CCS created by the AHRQ and at least three visits in outpatient care or one visit in inpatient care to define chronic condition. Although our method was strict and robust, the number of people with chronic conditions could have been underestimated. TCM use not covered by the NHI program (4% of TCM hospitals and 11% of TCM clinics) 30 could not be determined in this study; thus, TCM use by adults with chronic conditions or MCC in Taiwan was slightly underestimated. Another limitation is that, although we explored the TCM use of adults with seven common chronic conditions, we were not able to determine the TCM use of adults with comorbidities of these chronic conditions in our study. We analyzed the data for only one year, because the number of chronic conditions of an individual may be different in each year. We implemented our studies by analyzing the 2005 data because the sampling population in 2005 was nationally representative, and not for other years. 22 However, we agree that 2005 data are a bit old, and we have added this as one of our limitations.
Conclusions
TCM use (Chinese herbs, acupuncture–moxibustion, and traumatology manipulative therapy) by adults with chronic conditions or MCC was higher than that by adults without chronic conditions or without MCC, respectively. The probability and frequency of TCM use increased as the number of chronic conditions increased. The probability of Chinese herbs use, traumatology manipulative therapy use, and, particularly, acupuncture–moxibustion use increased as the number of chronic conditions increased. Among the seven common types of chronic conditions, adults with arthropathy were the most likely to use TCM, followed by those with COPD or asthma. Adults with diabetes were the most unlikely to use TCM.
Taiwan government officials have recently implemented TCM advanced care plans for patients with certain chronic conditions such as stroke, cancer, childhood asthma, and childhood cerebral palsy. We suggest that government policy makers should further emphasize administering integrated TCM and WM care for people with chronic conditions or MCC. In the future, we will further explore the primary chronic conditions treated by TCM therapy in adults.
Footnotes
Author Disclosure Statement
No competing financial interests exist.