
Abstract
Background/Objectives:
Sleep disorders are one of the most common difficulties facing older people. Meditative movement interventions (MMIs), a new category of exercise integrating physical activity and meditation (e.g., t'ai chi, yoga, and qigong), may benefit older people with sleep problems. This systematic review synthesized the evidence on the effect of MMIs on older people's quality of sleep.
Methods:
PubMed, EMBASE, CINAHL, PsycINFO, Scopus, the Cochrane Library, the China Science and Technology Journal Database (CSTJ) and the China National Knowledge Infrastructure (CNKI) were searched—from 1950 to March 2014—for randomized controlled trials. Articles were screened and selected by two researchers. Data were extracted from the included studies using specified forms. The same researchers independently evaluated the quality of each article. A meta-analysis was conducted to examine the pooled effect of MMI on sleep quality compared with the control groups.
Results:
Fourteen of 1049 studies were included, involving 1225 participants. Interventions included t'ai chi, yoga, qigong, and multicomponent MMI and lasted 12–24 weeks. Ten studies had a low risk of bias. The interventions resulted in significantly better sleep quality scores than either active therapy or usual care/wait-list controls (standardized mean difference, −0.70;95% confidence interval, −0.96 to −0.43). Subgroup analyses revealed that the effect of MMI on sleep quality was not influenced by the type or duration of the intervention. However, pooled results of studies with intervention frequency of fewer than 3 times per week did not show a positive effect on sleep quality. Lower-quality studies had larger effect sizes than high-quality studies. No adverse events were reported.
Conclusion:
The current review demonstrated that MMI had a moderate effect on improving the quality of sleep for older people with sleep complaints. However, the evidence is inconclusive because of the varying study quality and MMI modalities. This study highlights the need for higher-quality randomized, controlled trials and more sufficient fidelity of intervention implementation to confirm the results. It also highlights the need for comparing the effectiveness of MMI on different subgroups of the elderly population.
Introduction
S
Several factors might result in poor sleep quality in the elderly. As people age, the sleep-wake circadian rhythm and hormone secretions become less robust. This is manifested as sleep architecture changes, in particular reduced slow-wave sleep and REM sleep, decreased total sleep time, and increased sleep fragmentation. Decreased health status, psychiatric illness, cognitive disorder status, and various adverse effects from medications or psychological factors (e.g., isolation, bereavement, the stresses of care giving) will also contribute to poor sleep quality in the elderly population. 2,8 In conclusion, these notable age-related changes in sleep architecture and multifactional risk factors implied the high potential for sleep disorders and reduction of sleep quality among elderly adults.
In recent decades, much effort has been directed toward solving this problem for elderly people. The major conventional approaches to the treatment of sleep disorders involve pharmacologic and psychological interventions. The most common intervention for sleep disorders, particularly for insomnia, is pharmacological agents. 11 –13 However, the use of these drugs has the potential to cause many adverse effects, such as potential risks of tolerance, falls, reduced cognitive function, and fractures. 14 –17 Cognitive-behavior therapy, which typically consists of cognitive and behavioral components, is the mainstream of psychological intervention and has significant and long-lasting improvements on sleep patterns. 18 –20 However, despite the positive benefits of cognitive-behavior therapy on sleep patters, many barriers, such as the lack of highly trained therapists, long treatment duration, initial costs, and requirement of literacy, prevent the widespread use of these interventions. 21
Apart from these mainstays of conventional treatment, evidence-based complementary and alternative medicine (CAM) approaches are of interest and becoming increasingly popular. Different CAM approaches have been used for this clinical issue. The major categories of CAM approaches for sleep disorders in older adults include manual therapies (e.g., acupuncture, acupressure, and massage), herbs, natural products (e.g., valerian, melatonin), and mind-body therapies (e.g., meditation, relaxation techniques, yoga, and t'ai chi). 22,23 Among these CAM approaches, meditative movement intervention (MMI), which combines meditative focus with movement, has become an increasingly popular intervention for sleep disorders in Asia and the West. 24
Meditative movement is a newly coined term for this category of intervention. It is defined as some form of movement or body positioning as well as focus on breathing with a cleared or calm state of mind. It not only comprises implementation of “energy in the body” but also develops the “rested mind,” a deeply physical and mental relaxation. 24 T'ai chi, qigong, and yoga are the more common formats of meditative movement. T'ai chi and qigong are closely related; both are based on the common theory and philosophy of Traditional Chinese Medicine and originate in the martial arts of China. They incorporate body movement, breath, and attention training together and have a potential positive effect on alleviating disease symptoms and maintaining health. 25 –27 Yoga, as a mind-body approach, is based on ancient Indian traditions and contains mindfulness, meditation, postures, and breathing exercises to achieve a balance of the physical and the emotional. 28 Additionally, some less familiar methods, such as sign-chi-do, neuromuscular integrative action, and eurhythmy, have been developed in Western cultures. However, few scientific studies have evaluated these methods, and none have focused on sleep.
MMI has positive effects on a wide range of mental and physical health parameters. Research has consistently found that meditative movement has a positive effect on cardiorespiratory fitness, physical function, and symptoms of depression and anxiety. 27,29 Meanwhile, MMI has been widely used to cope with sleep problems, and the possible underlying mechanism in promoting sleep may come from these two aspects. On the one hand, physical activity has benefits for sleep and body recuperation through energy expenditure, raising body temperature, and increasing endorphin secretion. 30,31 On the other hand, meditation-induced relaxation might help to change the dysfunctional pre-sleep interpreting process and disrupt rumination and worry, which may contribute to the alleviation of sleep complaints. 27,29
In the past decades, previous systematic and narrative reviews have concluded that yoga and t'ai chi programs can improve self-reported sleep quality in the adult population, especially in prolonging sleep duration and giving a better feeling of being rested in the morning. 23,32 However, the findings of these reviews were based on the general adult population rather than older people, and no Chinese literature was included. More recently, a systematic review assessed the effect of yoga on sleep quality and depression in the elderly. 33 It included only three randomized controlled trials (RCTs) with sleep quality as the outcome and demonstrated the significant long-term effects of yoga on improving sleep quality in this population. However, because of the limited number of trials, the small sample sizes of these trials, and the focus on only one type of MMI, the total effect of MMI on sleep is still unclear. In addition, because those studies were published, new evidence from additional randomized trials has become available. Therefore, the current study aimed to update and synthesize the evidence and to assess the effects of meditative movement on improving sleep quality and physical outcomes in elderly people with sleep disorders.
Methods
Types of studies
RCTs comparing meditative movement intervention with at least one control group were included.
Types of participants
Adults over 60 years of age (mean age) with poor sleep quality documented by standardized subjective measures (e.g., the Pittsburgh Sleep Quality index 34 ), objective measures (e.g., polysomnography, actigraphy), or sleep diary who were diagnosed as having insomnia by standard criteria 35 –37 or with a complaint of sleep difficulties were included. Insomnia associated with other medical conditions was also included. Other sleep disorders, such as sleep apnea, periodic leg movement, or REM behavior disorder were excluded because they usually require medical treatment.
Types of interventions
All forms of MMIs were included, but MMI as part of a multicomponent intervention was excluded because it would be difficult to separate the effects of MMI from those of the additional modalities. Studies with breathing therapy alone were also excluded because they do not have an element of movement. Studies comparing MMI to a control condition (no intervention, usual care, routine care, or wait-list control) or active alternative intervention were included. Studies with multiple-armed, separate meta-analyses were conducted to carry out different comparisons.
Types of outcomes measures
The outcome included sleep-related quality as measured by standardized scales or objective measurements.
Electronic searches
The following databases were searched: PubMed (1950–March 2014), EMBASE (1980 to March 2014), Cochrane Library resources (Issue 3 of 12, March 2014), PsycINFO (1967 to March 2014), Scopus (1996 to March 2014), CINAHL (1982 to March 2014), the China Science and Technology Journal Database (CSTJ) (1989 to March 2014) and the China National Knowledge Infrastructure (CNKI) (1990 to March 2014). Each database was searched using keywords for sleep disorder (sleep disorder, insomnia, sleep complaints, sleep disturbance, sleep quality) and for meditative movement (meditati*, tai ji, yoga, qigong, neuromuscular integrative action, sign-chi-do, eurythmy). The reference lists of original studies and reviews were screened to identify additional articles, and the website of the National Center for Complementary and Alternative Medicine and Google Scholar were searched for further studies.
Study selection and data extraction
Two reviewers (Wu and Lan) independently screened the titles and abstracts retrieved from the search for identification of the relevant studies. The full-text copies of these studies were then obtained and independently assessed on the basis of criteria for inclusion. Data were extracted by using predesigned data extraction forms based on the extraction form of the Cochrane Collaboration and revised to ensure that they were suitable for this review. 38 The following data on the studies were collected: study design, setting, inclusion and exclusion criteria, participant description, intervention description, control, outcomes, findings, compliance, and reported adverse effects (Table 1). One reviewer Wu) extracted the data, while the other (Lan) verified its accuracy. Any disagreements about study selection or data extraction were discussed with a third reviewer (Kwong) for a final decision. If necessary, the authors of the included studies were contacted for additional information.
NR, not reported; PSQI, Pittsburgh Sleep Quality Index.
Assessment of risk of bias in included studies
Two reviewers assessed the risk of bias of the included studies independently, using the risk of bias assessment tool proposed by the Cochrane Back Review Group. 39 This assessment tool is considered suitable for nonpharmaceutical intervention studies. The tool comprises 12 assessment criteria with 5 domains on selection bias (3 items), performance bias (4 items), attrition bias (2 items), reporting bias (1 item), and detection bias (2 items). Each item was rated as 1, indicating low risk of bias, or 0, indicating unclear or high risk of bias. Total scores of 6 or above indicate a low risk of bias, while a score of less than 6 indicates some risk of bias.
Statistical analysis
RevMan 5.2 software of the Cochrane Collaboration (Oxford, United Kingdom) was used for data analysis. Intervention effects were defined as the standardized mean difference (SMD) and a 95% confidence interval (CI) of the post-intervention score. An SMD greater than 0.8 was considered a large effect size, an SMD of 0.5–0.8 a moderate effect size, and an SMD of 0.2–0.5 a small effect size. 40 A test of heterogeneity was used for each outcome using a chi-square test and I 2 statistic. An I 2 value greater than 50% indicated significant heterogeneity across studies. If no significant heterogeneity was detected, a fixed-effect model was calculated. If significant heterogeneity was observed, a random-effect model was used. Subgroup analyses stratified by type, frequency and duration of intervention, study quality, and different control groups were performed to look for explanations for the heterogeneity. In addition, sensitivity analysis was performed to explore the influence of individual studies by excluding each study in turn. Publication bias was assessed by using funnel plots when more than 10 studies were included in a meta-analysis. 38
Results
Search results
One thousand and forty-eight references were retrieved from the electronic search of databases, and one additional record was retrieved based on the reference lists of the original identified articles. After exclusion of duplicates, 471 references were screened and 393 references removed because they were not RCTs, participants were not elderly with sleep problems, and/or the intervention was not an MMI. Of 56 full-text articles assessed for eligibility, 14 were eligible and included for further review. Twelve studies had sufficient data to be included in the meta-analysis for quantitative comparison (Fig. 1).
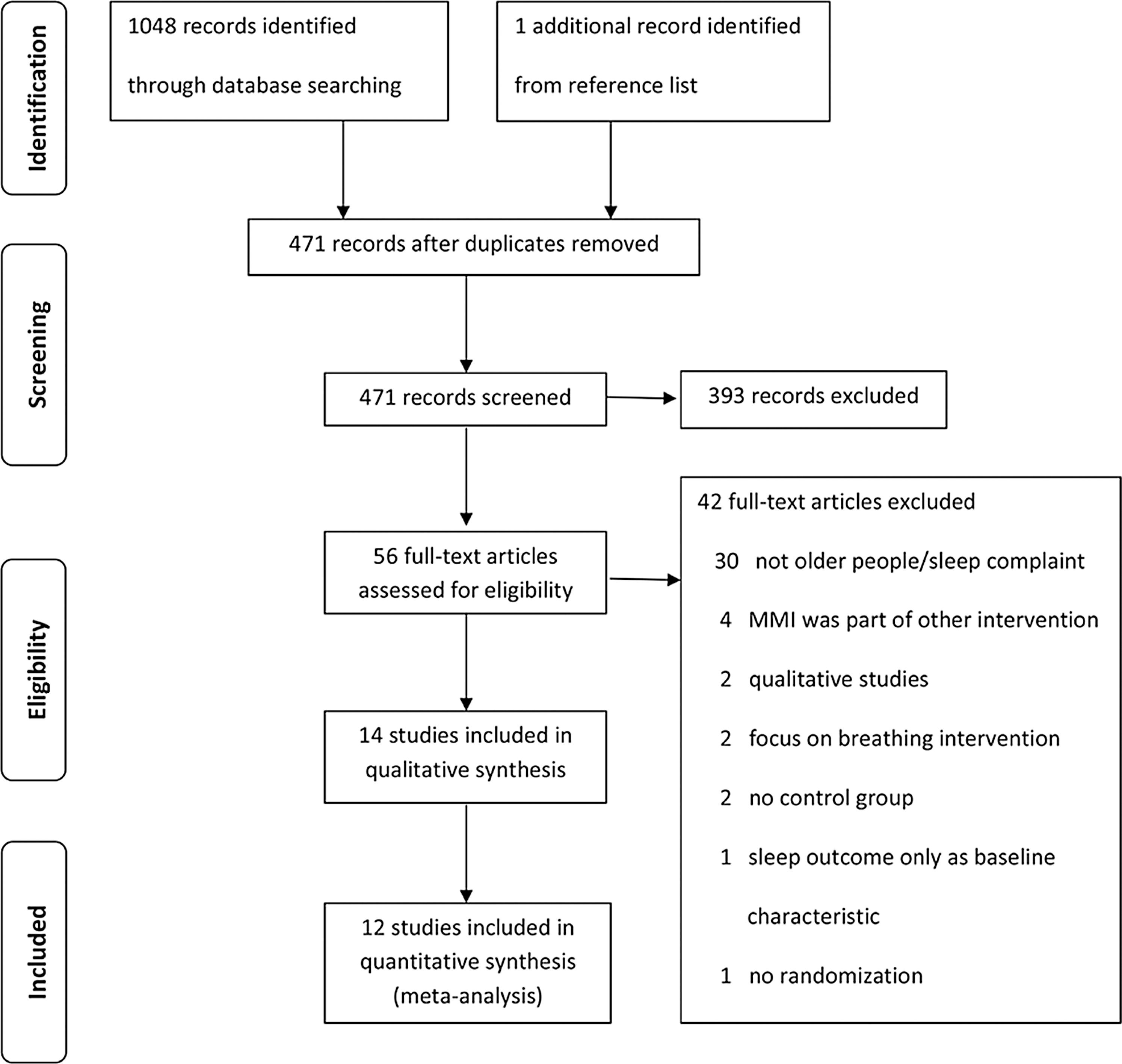
Flowchart of trial selection process. MMI, meditative movement intervention.
Characteristics of included studies
The characteristics of the included studies are presented in Table 1. Fourteen trials with 1225 participants were included. 41 –54 The studies were performed in the United States, 44,47,48,51,52 China, 43,54 Taiwan, 41,42 India, 45,49 Japan, 53 Iran, 46 and Germany. 50 The mean age of participants was 70.35 years. The participants were recruited from the community, 41 –43,47,50,52,54 long-term residential homes for the elderly, 45,46,49 outpatient departments of a rehabilitation facility/hospital, 51,52,53 and multi-resources, including the community seniors' center and a physician's office. 44,48 Ten studies were conducted among the general elderly population, 41 –50 3 were conducted among older patients after stroke, 51 –53 and 1 was conducted among older people with diabetes mellitus. 54
Among the 14 included studies, 9 applied t'ai chi, 1 used qigong, 1 applied t'ai chi and qigong, and 3 studies used yoga. The duration of the overall interventions ranged from 12 to 24 weeks. The duration per session varied, with a range of 20–70 minutes, and most studies included interventions lasting 60 minutes/session. 43 –45,48 –52 The frequency of the intervention also varied widely, ranging from once a week to twice a day. Most interventions were performed three times a week. 41,42,44,46 –48,51,52,54 The intervention was carried out in facilities 45,46,49,51,52,53 or in the community, 41,43,44,47,48,50,54 or practiced at home. 42 Four of the included studies provided the intervention in group format. 41,46,48,51 Nine of the included studies stated that the intervention was provided by a qualified instructor with certification or considerable teaching experience. 41,42,44,46 –48,51,52,54
Eleven of 14 included studies were designed with 2-arm RCTs, and 3 studies used a 3-arm study design. 44,49,52 Nine RCTs compared MMI to no specific treatment, including usual care or a wait-list control. 41,42,44 –46,49 –52 Six RCTs compared MMI to active therapy, including walking, low-impact exercise, sleep hygiene education, or Ayurveda. 43,44,47 –49,53,54
All RCTs assessed sleep quality using subjective, self-rating instruments, including the Pittsburgh Sleep Quality Index (PSQI), the sleep disturbance subscale of PSQI, or the Sleep Rating Questionnaire. None of the studies examined sleep outcomes using objective measurements. Fourteen studies examined the post-intervention effects of MMI, and only 1 study, with a 9-week follow-up, evaluated the lasting effects of MMI after intervention. 47
Risk of bias of included studies
The mean score for risk of bias of the included studies was 6.5. Ten RCTs were classified as having a low risk of bias, and the remaining 4 were classified as having some risk of bias (Table 2). Adequate allocation concealment was reported only in 7 RCTs, whose scores for risk of bias were more than 6. 41,45,47 –49,51,52 Nine RCTs reported the details of a random generation method, 41 –43,45,47 –49,51,52 but only 1 of them was a study with a risk of bias lower than 6. None of the studies involved blinded providers or participants. Only 6 RCTs with risk of bias score greater than 6 reported blinding outcome assessors. 41,48,49,51 –53 None of the studies with risk of bias scores lower than 6 used intention-to-treat analysis. Only 8 studies report participants' attendance rate. 41,42,44,47,48,50 –52 No authors responded to attempts to contact them regarding missing information required for the assessment of risk of bias; as a result some items remained “unclear.”
MMI and sleep quality
Twelve studies were included in the meta-analysis, showing that the experimental group had better sleep quality than the control group (SMD, −0.70 [95% CI, −0.96 to −0.43]; p<0.001) using a random-effect model. However, statistical heterogeneity existed among these trials (I 2 =70%; chi-square=36.20; p<0.001) (Fig. 2). The other 2 studies could not be pooled; they also revealed that MMI could significantly reduce sleep disturbance, increase sleep duration, decrease time needed to fall asleep, and improve the feeling of being rested. 44,49 Four studies examined safety issues and did not report any adverse effects from MMI, 41,47,48,51 and other studies did not mention safety examinations.
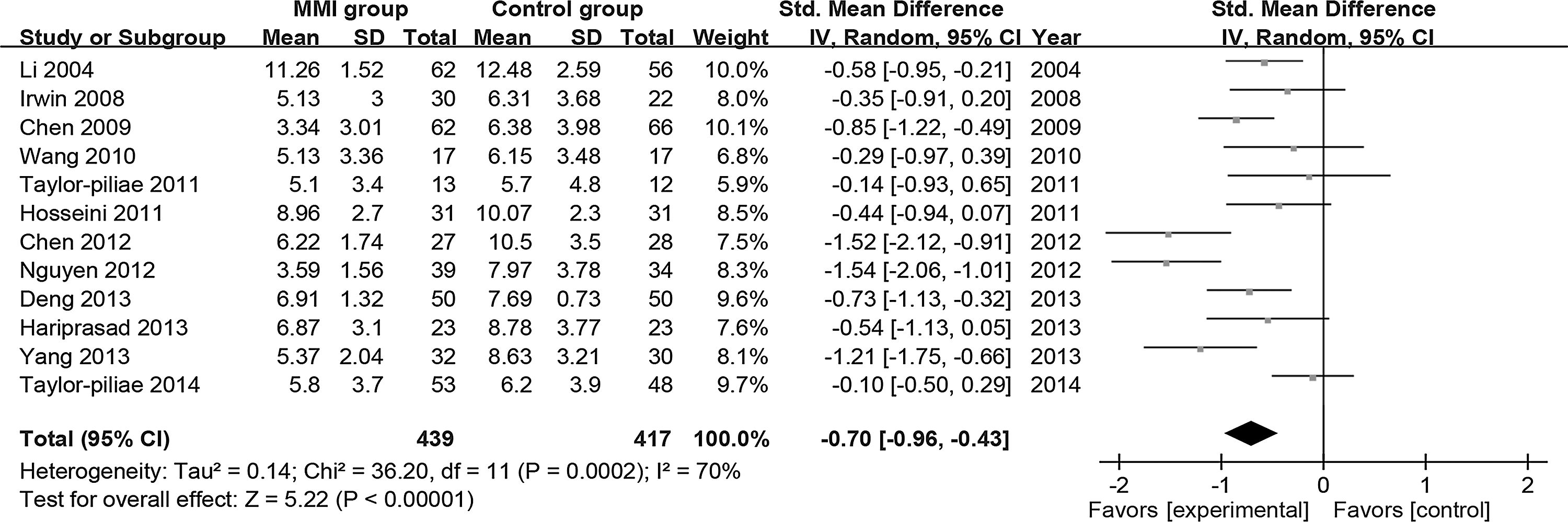
Forest plots of effect estimates of MMI versus controls on sleep quality outcomes at final treatment. CI, confidence interval; SD, standard deviation; Std, standardized.
Subgroup and sensitivity analysis
In the subgroup analysis comparing the pooled results to control group, a relevant pooled effect on the post-intervention PSQI global scores was found in most subgroups, except for the studies with intervention frequency fewer than 3 times a week (Table 3). In comparing the pooled results among subgroup comparisons, no significant difference was found in terms of types of MMIs, duration of intervention, or types of controls. However, a significant subgroup difference was found in the study quality. Studies with some risk of bias reported a mean SMD twice as high as that in studies with a low risk of bias (−1.13 versus −0.54; p=0.04). Studies with frequency greater than 3 times per week seemed to produce a higher effect in terms of pooled SMD (−-0.82) than those with frequency of 3 times per week (−0.57), although the subgroup difference was not statistically significant. In addition, sensitivity analysis revealed that exclusion of any single study did not materially alter the overall SMD, with a range from −0.62 (95% CI, −0.86 to −0.38) to −0.76 (95% CI, −1.01 to −0.51).
One study with a multicomponent intervention was not included in subgroup analysis.
CI, confidence interval; SMD, standardized mean difference.
Risk of bias across studies
The slightly asymmetrical shape of the funnel plot indicated that potential publication bias might be present, which may have influenced the results of this review (Fig. 3).
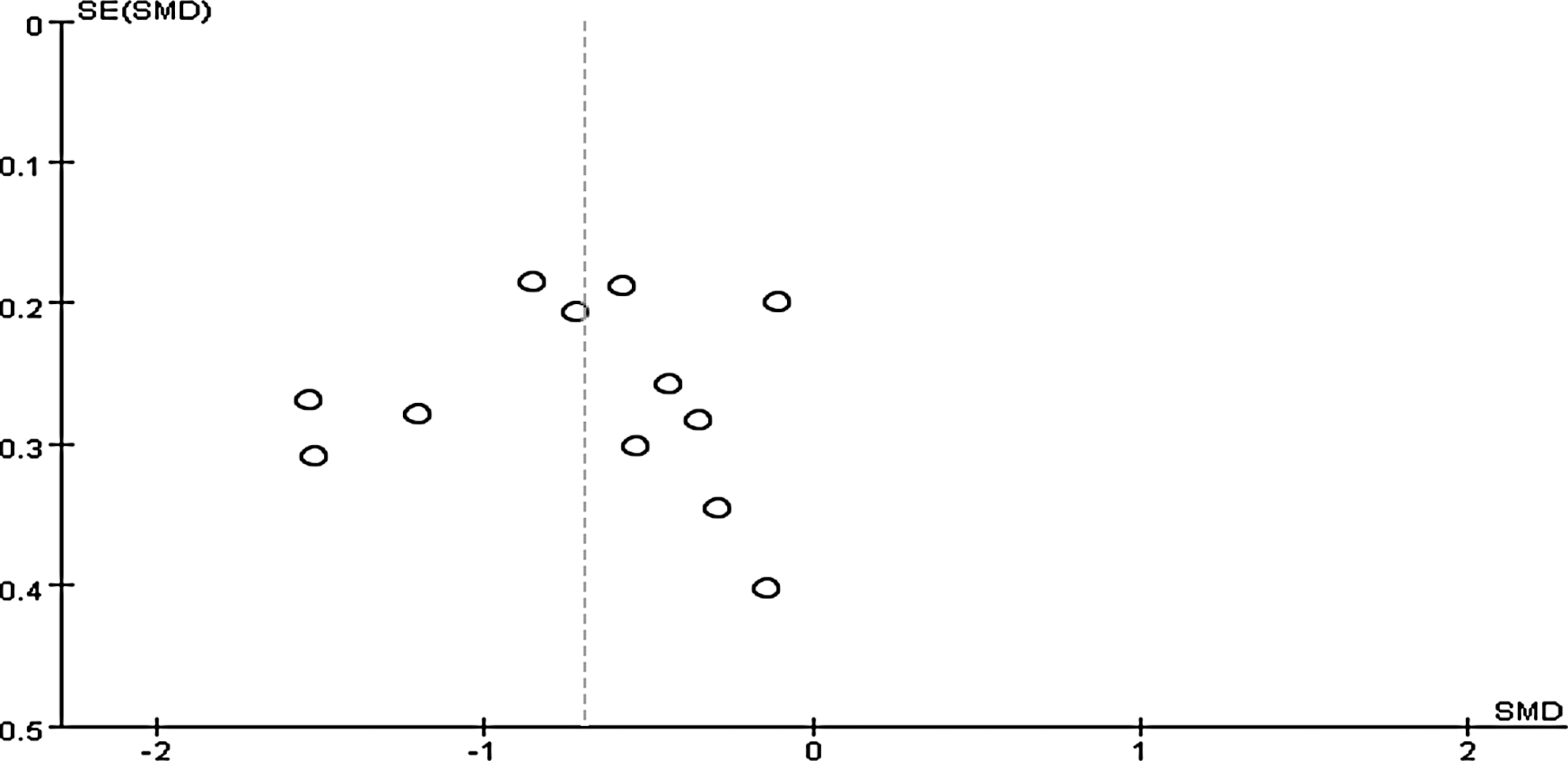
Funnel plots of estimate of publication bias. SE, standard error; SMD, standardized mean difference.
Discussion
This systematic review and meta-analysis showed some convincing evidence that MMI can be beneficial for sleep quality in elderly people with sleep complaints. The pooled effects of MMI on sleep quality were clinically relevant when compared with either active therapies or usual care/wait-list controls. Improvement in sleep quality was consistently found in different types of MMI. No adverse events were reported among the included studies. This implies that MMI may be considered as an effective treatment for improving sleep quality.
However, because of the diversity of the interventions studied, it is impossible to draw definite conclusions on the effectiveness of a particular MMI. There was a wide range of intervention durations and frequency among the included studies. The type of MMI also varied. For instance, t'ai chi has various styles, and each style of t'ai chi also has different versions, with different forms and postures. Hence, it is difficult to pinpoint which intervention characteristics (type, duration, intensity, or format) are most effective based on analysis of the results. In addition, evidence from the current review suggests that the effectiveness of MMI is likely to be influenced by intervention frequency. Subgroup analysis revealed that practicing an MMI fewer than 3 times a week did not improve sleep quality for older adults. This indicates that to improve sleep quality, elderly people should perform MMI at least 3 times per week. The subgroup analysis also indicated that studies involving an intervention more than 3 times a week had a larger effect size than those that conducted the intervention only 3 times a week. It seems that the higher the frequency of practicing MMI, the more positive the effect on sleep quality. This is consistent with the World Health Organization physical activity guideline for elderly people. 55 Previous studies also found that high-frequency exercise had a more positive effect on reducing fracture risk, sarcopenia, and coronary heart disease risk in the elderly than low-frequency exercise. 56 However, because the sessions studied were of varying durations, it is impossible to draw conclusions as to the “minimum effective dose” of MMI.
The quality of the studies included in the review varied. Subgroup analysis revealed that the observed effect size of MMI was significantly influenced by the study quality. Low-quality studies in the current review reported a significantly larger effect size than did those of higher quality. There is a strong possibility that low-quality studies reduce the ability to draw conclusions about the true effect of MMI based on the evidence. The effect of low-quality studies on results may partially be explained in terms of the following tentative conclusions.
First, the defect of study design in the low-quality studies resulted in higher selection, attrition, and detection biases than in high-quality studies. For example, the selection bias was higher in the lower-quality studies because they made less use of random sequence generation and allocation concealment. Only one low-quality study described the specific methods of random sequence generation, although all of them claimed to have used randomization methods. It is unclear whether their methods of randomization were reliable. Problems in sequence generation might have led to some studies not being truly randomized. This may have resulted in lack of comparability between experimental and control groups and affected the accuracy of the results. None of the low-quality studies ensured allocation concealment, which means that the researchers in these studies might have known the group assignments of each participant. This could have led to the potential exclusion of certain participants or the allocation of some participants to a specific group based on research purposes, and therefore to overestimation of the intervention effect compared with studies with adequate allocation concealment. Previous studies indicated that in the absence of allocation concealment, intervention effect estimates could be exaggerated by up to 30%–40%. 57
The attrition bias was also higher in the low-quality studies. Two of the low-quality studies reported high dropout rates ranging from 17% to 26%, while the other two did not describe the dropout rates; this may have led to unclear information on withdrawal. Moreover, none of these studies used intention-to-treat analyses to handle the missing data. The participants who withdrew from the studies may have done so partially because of lack of satisfaction with the effectiveness of the intervention. Hence, excluding the data from participants who withdrew could also result in overestimating the treatment effect. Compared with the high-quality studies, low-quality studies seemed to produce higher detection bias. None of the low-quality studies reported assessor blinding. In view of the characteristics of the interventions and ethical issues, it is difficult to blind participants and personnel to behavioral interventions such as MMI. Therefore, blinding the assessors is important to reduce risk of bias, especially when all outcomes are subjective outcome measurements. A lack of blinded assessors might produce observer bias because assessors will usually trend to the results they intended when collecting the outcome data.
Second, the integrity of the intervention, especially implementation fidelity, may also be an important issue for consideration. Implementation fidelity refers to the degree to which an intervention is delivered as intended. 58 Appropriate evaluation of the implementation fidelity could help to determine the true effect of the intervention. Adherence is the essential measurement of implementation fidelity. However, most low-quality studies did not examine the adherence rates of MMI, so it was unclear whether the participants had received the required intervention sessions. In addition, some of the low-quality studies failed to describe the qualifications of the intervention provider or a clear protocol for the intervention. 43,53 This might result in difficulty evaluating the quality of the intervention delivery. In a word, the fidelity of the intervention implementation seems unclear in the low-quality studies. The accuracy of the results found here may be reduced if these studies did not fully implement MMI.
In contrast, implementation fidelity seems better in high-quality studies than in low-quality ones. Most high-quality studies reported not only acceptable compliance of participants, clear intervention procedures, and qualified intervention providers but also several additional measures used to achieve higher fidelity. For example, one study used an additional prerecorded tape to guide the intervention process to ensure intervention consistency across the study sites and among the instructors. 41 Two studies examined participant responsiveness using performance recordings or daily practice diaries, which could motivate them to continue performing the MMI. 42,47
Third, none of the low-quality studies reported study power analysis. Hence, it is impossible to identify whether the samples used were large enough to achieve the sufficient study power. Insufficient sample size would result in difficulty detecting significant between-group differences, which might in turn lead to the conclusion that the interventions are not effective when in fact they are effective (type II error), thus limiting the precision of the results in this review.
The results of the current review are roughly in line with those of previous research. Some systematic and narrative reviews in the literature are related to the effects of different types of MMI on sleep. 23,32,33 Consistent positive effects of MMI were found among these reviews. T'ai chi and yoga proved efficient in improving self-reported sleep and reducing insomnia in general adult and elderly populations. However, as these prior reviews only examined a few studies or a single type of MMI and involved both elderly populations and the general adults population, their findings might not be convincing enough to permit conclusions regarding the general positive effect of MMI on older adults with sleep disorders. In contrast, this review pooled meta-analysis data from previous RCTs of different kinds of MMIs on the treatment of sleep disorders in older adults, providing more clear evidence of their effects on sleep quality in the elderly population.
Further, compared with other treatment modalities, the effect size of MMI on improving self-reported sleep quality was similar. In a systematic review on exercise for middle-aged and older adults with sleep problems, sleep quality was increased, with an SMD of 0.47 (95% CI, 0.08–0.86), 30 which was similar to the effect size of MMI in the current review. In another systematic review on behavioral interventions for middle-aged and older adults with insomnia, the results of a meta-analysis revealed that behavioral intervention significantly improves sleep quality, with an SMD of 0.60 (95% CI, 0.19–1.01). 59 This was also similar to the results of the current review, confirming the evidence of this review and suggesting that MMI has a similar effect on improving sleep quality among these interventions.
Limitations
This systematic review and meta-analysis has some limitations. First, the current study only includes studies published in English or Chinese, which may limit the generalizability of the findings. Second, all of the included studies used subjective outcome measures that were easily influenced. This may reduce the accuracy of the current findings. Third, in subgroup analysis, the number of studies and individuals included was relatively small. They may be insufficiently robust for determining the actual effects. Finally, there was substantial heterogeneity in this review. The major reasons for this, including study quality and frequency of intervention, were reported through subgroup analysis; however, the severity of the sleep complaints and health status of participants were not considered, which may have increased the heterogeneity.
Implications
Even with these limitations, this systematic review summarized current evidence for MMI on sleep, with implications for practice and research. The participants of the current review were recruited from a variety of settings and countries, including older people in general, stroke survivors, and diabetic older patients. The results seem to apply to most elderly people with sleep problems in clinical practice. However, the findings suggest that sufficient frequency of MMI is important to its effectiveness. Hence, it is necessary to develop suitable strategies to motivate older people to practice MMI sufficiently frequently. The finding suggests that future studies need to identify more rigorous RCT designs, have sufficient implementation fidelity to examine the genuine effectiveness of MMI, and adopt both subjective and objective outcome measures to evaluate the effects of MMI on sleep quality. Finally, older people with various chronic diseases and health status are likely to experience a different effect of MMI on sleep quality, so it would be worthwhile to investigate the effectiveness of MMI on different subgroups of the elderly, such as the depressed elderly and frail elderly.
Conclusions
In sum, this systematic review provided evidence that MMI can be effective in improving sleep quality for older people with sleep complaints. However, the effectiveness of MMI seems to be influenced by practice frequency. The effect size of MMI differed between low- and high-quality studies. Future research should include RCTs with more rigorous methods and higher implementation fidelity to confirm the accuracy effect size of MMI. Future studies are also needed to evaluate the effectiveness of MMI among different populations.
Footnotes
Acknowledgments
This work was supported by The Hong Kong Polytechnic University Joint Supervision Scheme with the Chinese Mainland, Taiwan, and Macao Universities (G-UB62).
Author Disclosure Statement
No competing financial interests exist.