
Abstract
Objectives:
Acupuncture is a form of Traditional Chinese Medicine that has been used to treat a broad range of medical conditions, including dermatologic disorders. This systematic review aims to synthesize the evidence on the use of acupuncture as a primary treatment modality for dermatologic conditions.
Methods:
A systematic search of MEDLINE, EMBASE, and the Cochrane Central Register was performed. Studies were limited to clinical trials, controlled studies, case reports, comparative studies, and systematic reviews published in the English language. Studies involving moxibustion, electroacupuncture, or blood-letting were excluded.
Results:
Twenty-four studies met inclusion criteria. Among these, 16 were randomized controlled trials, 6 were prospective observational studies, and 2 were case reports. Acupuncture was used to treat atopic dermatitis, urticaria, pruritus, acne, chloasma, neurodermatitis, dermatitis herpetiformis, hyperhidrosis, human papillomavirus wart, breast inflammation, and facial elasticity. In 17 of 24 studies, acupuncture showed statistically significant improvements in outcome measurements compared with placebo acupuncture, alternative treatment options, and no intervention.
Conclusions:
Acupuncture improves outcome measures in the treatment of dermatitis, chloasma, pruritus, urticaria, hyperhidrosis, and facial elasticity. Future studies should ideally be double-blinded and standardize the control intervention.
Introduction
A
Acupuncture holds a long history in China, where it continues to be regularly used independently and as an adjunct to modern medicine to treat a broad range of diseases, including dermatologic disorders. Over the past few decades, the interest in acupuncture has expanded to other countries, including the United States, because of the growing popularity of complementary and alternative medicine (CAM). One systematic review estimated the prevalence of CAM use in the general U.S. population to be around 38%. 9 The national prevalence of acupuncture is estimated to be between 0.6% and 1.4%, according to another systemic review. 10 CAM was used specifically to treat dermatologic conditions in 6% of participants in one large national survey, of whom 9.3% used acupuncture. 11
An understanding of the evidence on acupuncture for the treatment of skin disease will be invaluable as dermatologists encounter an increasing number of patients seeking acupuncture as an alternative therapy. This systematic review assessed the results and quality of clinical studies and case reports on the use of acupuncture to treat a variety of dermatologic conditions. This appears to be among the first dedicated reviews to synthesize data focusing on acupuncture as a treatment modality in dermatology.
Methods
Search strategy and study selection
To identify relevant studies that used acupuncture to treat dermatologic conditions, a systematic search of MEDLINE, EMBASE, and the Cochrane Central Register was performed. In MEDLINE, the following Medical Subject Headings were used: acupuncture therapy in combination with (skin diseases or dermatology). In EMBASE, a combination of key words and EMTREE terms for acupuncture therapy and (skin diseases or dermatology) were used. In the Cochrane database, key terms (acupuncture therapy or acupuncture) and (skin diseases or dermatology) were used. All searches were limited to clinical trials, controlled studies, case reports, comparative studies, and systematic reviews published in the English language. Systematic reviews were included to identify additional articles. Articles that used moxibustion, electroacupuncture, or blood-letting as forms of acupuncture were excluded.
The initial search of all databases identified 1255 articles (Fig. 1). Two reviewers manually screened relevant abstracts, yielding 48 articles eligible for inclusion criteria. An additional 4 articles were identified from related articles and citations. Articles were excluded if they were out of scope (i.e., did not evaluate a dermatologic condition or assessed only adverse effects secondary to acupuncture); were reviews; or used moxibustion, blood-letting, or electroacupuncture as primary treatment. Case reports were included given the limited number of controlled studies in English involving acupuncture as a treatment in dermatology. After careful review of each manuscript, 24 were included in this review. 12 –35
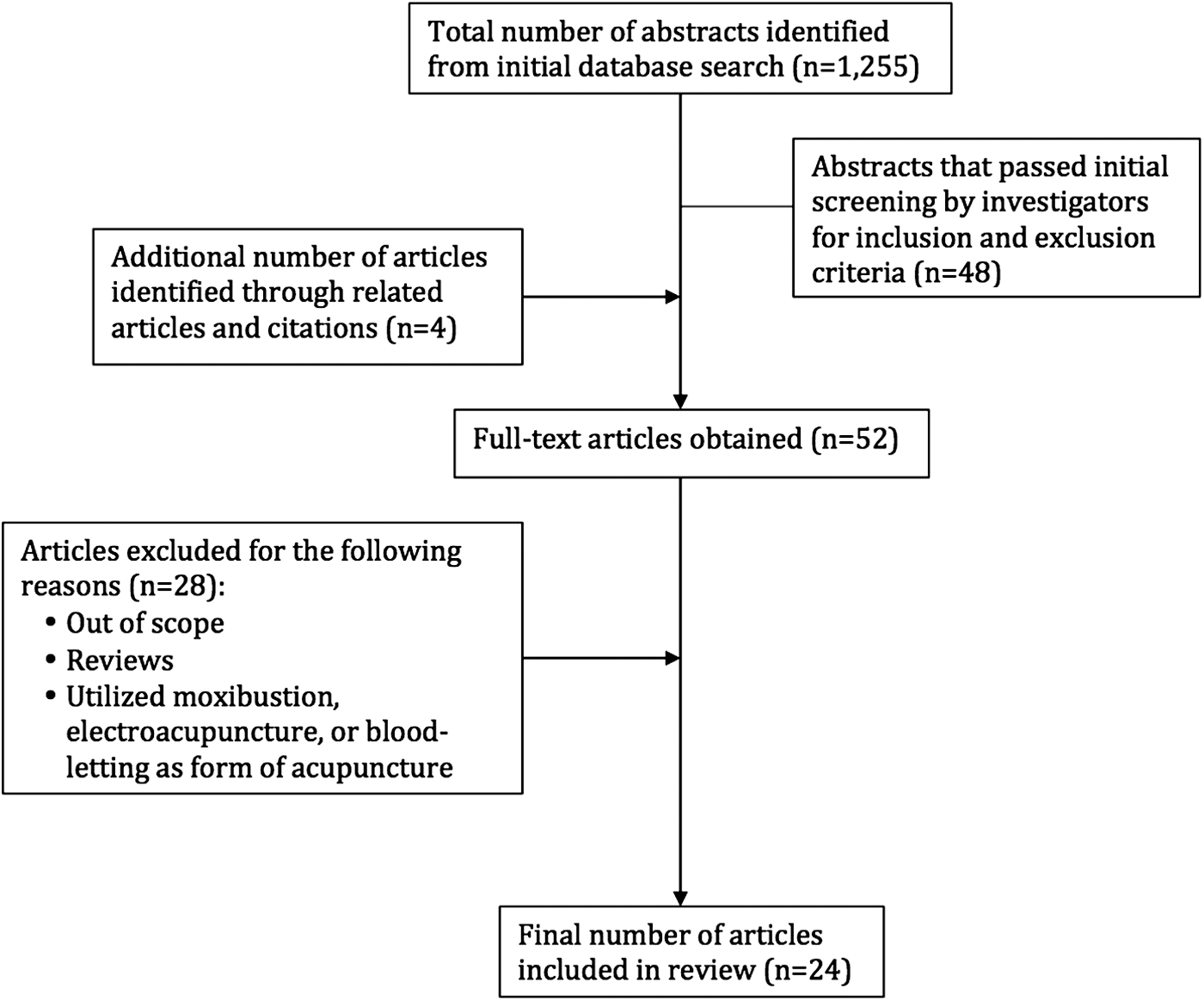
Literature search and study selection.
Data extraction and quality assessment
The following data were extracted from each study (Table 1): (1) study characteristics (author, year, country, and study design); (2) study population (population size, mean or median age); (3) dermatologic condition being treated; (4) acupuncture intervention and control intervention; (5) outcome measurements; and (6) main results and conclusions.
There are 361 classical acupuncture points with Chinese and numeric nomenclature. Both nomenclatures are included in the table as the authors have used them.
Criteria for therapeutic effects of chloasma set by the Professional Board of Dermatology and Venereology of China Association of Combined Chinese and Western Medicine: (1) cure: visible clearance >90%, normal pigmentation, and decreased index of the scoring evaluation after treatment ≥0.8; (2) markedly effective: visible clearance >60%, lighter pigmentation, and decreased index of the scoring evaluation after treatment ≥0.5; (3) effective: visible clearance >30%, lighter pigmentation, and decreased index of the scoring evaluation after treatment ≥0.3;(4) ineffective: visible clearance <30%, no change in pigmentation, and decreased index of the scoring evaluation after treatment <0.3.
AA, acupuncture in anesthesia area; DLQI, Dermatology Life Quality Index; EASI, Eczema Area and Severity Index survey (calculated from the following components: area of involvement, erythema, thickness, excoriations, and lichenification); EIQ, qualitative assessment of itch intensity; HPV, human papillomavirus; IGA, Investigator's Global Assessment (to measure disease severity); NAA, acupuncture in nonanesthesia area; NR, not reported; RCT, randomized controlled trial; SCORAD, clinical tool developed by the European Task Force on Atopic Dermatitis for assessing the extent, severity, and subjective symptoms of atopic dermatitis; VAS, Visual Analogue Scale (to rate level of itch).
The level of evidence was graded on a scale of I–V per guidelines used to evaluate primary research questions. 36 Studies are evaluated on the basis of study type, confidence interval size, randomization, blinding, and adherence. Level I and II studies contain stronger evidence than level III and IV studies, and level V articles are expert opinion papers.
Results
Twenty-four studies were identified. Among these, 16 were randomized controlled trials (RCTs), 6 were prospective observational studies, and 2 were case reports. Studies were conducted in inpatient and outpatient settings in China (n=11), Germany (n=4), Korea (n=2), Taiwan (n=1), the United States (n=2), Israel (n=1), Iran (n=1), Italy (n=1), and Sweden (n=1).
Dermatologic conditions being treated by acupuncture included atopic dermatitis (n=6), urticaria (n=3), pruritus (n=3), acne (n=3), chloasma (n=3), neurodermatitis (n=1), dermatitis herpetiformis (n=1), polyhidrosis (n=1), human papillomavirus (HPV) wart (n=1), breast inflammation (n=1), and facial elasticity (n=1). Three studies had level I evidence, 12 studies had level II evidence, 1 study had level III evidence, and 8 studies had level IV evidence.
Acupuncture resulted in statistically significant improvement of outcome measurements in 17 of 24 studies. Of the 7 studies that found no statistical significance in outcomes, 6 had no control group for calculation of p-values.
Studies on acupuncture and dermatitis, urticaria, and pruritus
Acupuncture was most commonly examined as a treatment for dermatitis, urticaria, and pruritus, with a total of 14 studies involving 559 participants. Treatment response was evaluated by using multiple objective and subjective outcome measures, described at the bottom of Table 1. For atopic dermatitis, the standard outcome measurement was the visual analogue scale (VAS) to evaluate severity of itch. In all 6 studies on atopic dermatitis, mean VAS score was statistically significantly lower in groups treated with acupuncture than in groups treated with placebo acupuncture or no intervention. Mean wheal or flare size was also statistically significantly reduced in acupuncture groups in 3 studies. However, most of these studies had small sample sizes, with 5 studies involving 20 patients or fewer.
Three studies addressed urticaria, including 2 on patients with chronic or refractory urticaria. Compared with placebo acupuncture, acupuncture statistically significantly reduced the rate and duration of urticarial episodes in 1 RCT. 24 Another RCT found that acupuncture resulted in statistically significantly greater clearance of wheals compared with oral antihistamines. 26 One observational study without a comparison group showed complete clearance of wheals in 25.8% of patients treated with acupuncture and prolongation of time between relapses. 25
Acupuncture relieved pruritus secondary to uremia, morphine, or dermatitis herpetiformis in 3 RCTs and 1 case report. 27 –30 In 1 RCT, acupuncture was superior to herbal medicine and oral diphenhydramine plus vitamin C for clearance of rash from neurodermatitis. 31
Studies on acupuncture and acne
One RCT and 2 observational studies (185 participants total) examined the therapeutic effect of acupuncture on clearance of acne lesions. The RCT found no statistically significant difference in clearance between acupuncture and herbal medicine, or between acupuncture and no intervention. 13 The 2 observational studies reported clearance of acne lesions in most study participants, but there were no control groups for comparison. 12,14
Studies on acupuncture and chloasma
Acupuncture therapy for chloasma was performed in 2 RCTs and 1 observational study with a total of 180 patients. Results were mixed. One RCT found statistically significantly greater clearance of chloasma in patients treated with acupuncture plus herbal medicine compared with patients treated with oral vitamin C and E. 15 Another RCT that compared acupuncture alone to oral vitamin C and E plus topical retinoid cream found no difference in chloasma clearance. 16 The observational study found greater than 90% clearance of chloasma and normal skin pigmentation in 40% of patients, and overall therapeutic effect (>30% lesion clearance and lighter skin pigmentation) in 87% of patients. 17
Studies on acupuncture and other dermatologic conditions
Four studies found acupuncture to be effective at treating other dermatologic conditions, including breast inflammation, polyhidrosis, HPV wart, and facial elasticity. A Swedish RCT involving 205 breastfeeding women found that acupuncture statistically significantly alleviated breast erythema, tension, and pain compared with oxytocin spray alone. 32 An observational study in China involving 56 patients with hyperhidrosis found a statistically significant reduction in sweating with acupuncture treatment compared with estazolam, a benzodiazepine derivative. 34 One case report on an HIV-infected patient with a chronic HPV wart resistant to cryotherapy reported clearance of the wart after 58 sessions of acupuncture over 19 months. 33 Finally, a study of 27 women found that acupuncture resulted in statistically significant changes in Moiré topography, suggestive of improvement in facial elasticity. 35
Discussion
This is among the first dedicated reviews to synthesize the evidence on acupuncture as a primary treatment modality for multiple dermatologic conditions. The results of this review support acupuncture as an alternative therapy in dermatology, with 17 of 24 studies showing statistically significant improvement in outcome measures compared with no intervention or other treatment options. Furthermore, in some studies acupuncture improved outcome measures statistically significantly more than placebo acupuncture, suggesting possible merit in the traditional theory of acupoints on meridians. 19,20,22,24
Modern investigations into possible mechanisms of acupuncture have mixed results on the validity of meridians, but consistent across studies is involvement of the autonomic nervous system and hypothalamus-pituitary-adrenal (HPA) axis, recruited via peripheral sensory receptors. 37 –44 Functional magnetic resonance imaging studies on humans found modulation of areas in the central nervous system involved in stress and nociception, such as the hypothalamus, nucleus accumbens, amygdala, hippocampus, and anterior cingulate gyrus. 39,41 –44 The downstream release of endogenous opioids is thought to contribute to subsequent analgesic and antipruritic effects. Furthermore, the pattern of brain activation seen in acupuncture was found to be distinct from that produced by pain from needle prick, which is uncommon during acupuncture. 39,41,43
Evidence also appears to support the role of neuromodulation of the immune system in mediating the pathogeneses of inflammatory and infectious skin conditions, such as acne, dermatitis, urticaria, and HPV. Studies on rats have shown decreased levels of pro-inflammatory cytokines—including tumor necrosis factor-α, interleukin-1β, and interleukin-6—after stimulation with acupuncture. 45 –49 The underlying mechanism of these findings is unclear, but suppression of cytokine synthesis via outputs from the HPA axis has been proposed. 38
The mechanism through which acupuncture may treat chloasma (or melasma) has not been as extensively studied. The disease is seen primarily in women and is thought to be caused by increased stimulation of melanocytes secondary to estrogen and progesterone, ultraviolet light, thyroid dysfunction, and genetic predisposition. 50 –53 Chloasma lesions are also found to have increased expression of vascular endothelial growth factor (VEGF). 54 –56 However, studies on acupuncture and levels of estrogen, progesterone, and VEGF in animal and human studies have not shown consistent results. 57 –62
The findings of this review must be interpreted in the context of the primary literature. There does not appear to be a consistent control group, and studies in this review used multiple comparisons, including no intervention, placebo acupuncture, and oral or topical supplements and medications. Some studies did not have a control group, making it difficult to assess whether improvements in outcomes were attributable to acupuncture or the body's natural response. The frequency and duration of the intervention used in some studies may not be translatable to daily life. For example, it may not be practical for individuals to attend acupuncture sessions multiple times per day or receive treatments that involve multiple months. Outcome measurements also varied across studies, even within the same dermatologic condition. This heterogeneity in outcome measurements did not allow us to pool findings in a valid form for meta-analysis.
Most studies did not mention blinding of patients and acupuncturists or adjusting for confounding factors, which may bias outcomes. Our search was also limited to studies published in the English language, which excludes many studies performed in China, where acupuncture is more prevalent and widely studied. Finally, studies with small sample sizes may overestimate the effect size and lower reproducibility of results. Our evaluation of level of evidence using a valid scale enabled us to systematically identify weaknesses associated with each study.
In summary, the findings of this review reveal that acupuncture may improve outcome measures in the treatment of multiple dermatologic conditions, including dermatitis, chloasma, pruritus, urticaria, hyperhidrosis, and facial elasticity. Future studies in this area will need to consider standardizing the control intervention. For example, investigators aiming to evaluate the efficacy of acupuncture may use no intervention as the control, while investigators aiming to evaluate the validity of acupoints and meridians may consider using placebo acupuncture as the control. Blinding of participants to treatment modality and blinding of acupuncturists to disease being treated will also prevent psychological and procedural bias in an area already prone to subjectivity. More high-quality studies are needed to suggest mechanisms, clarify efficacy, and ultimately guide clinicians in this evolving field.
Footnotes
Acknowledgments
We would like to thank Bruce Abbott for his assistance with systematic search protocols.
Author Disclosure Statement
No competing financial interests exist.