
Abstract
Objective:
There have been no systematic reviews, let alone meta-analyses, of randomized controlled trials (RCTs) comparing tongxinluo capsule (TXL) and beta-blockers in treating angina pectoris. This study aimed to evaluate the efficacy of TXL and beta-blockers in treating angina pectoris by a meta-analysis of eligible RCTs.
Methods:
The RCTs comparing TXL with beta-blockers (including metoprolol) in treating angina pectoris were searched and retrieved from databases including PubMed, Chinese National Knowledge Infrastructure, and WanFang Data. Eligible RCTs were selected according to prespecified criteria. Meta-analysis was performed on the odds ratios (OR) of symptomatic and electrocardiographic (ECG) improvements after treatment. Subgroup analysis, sensitivity analysis, meta-regression, and publication biases analysis were conducted to evaluate the robustness of the results.
Results:
Seventy-three RCTs published between 2000 and 2014 with 7424 participants were eligible. Overall ORs comparing TXL with beta-blockers were 3.40 (95% confidence interval [CI], 2.97–3.89; p<0.0001) for symptomatic improvement and 2.63 (95% CI, 2.29–3.02; p<0.0001) for ECG improvement. Subgroup analysis and sensitivity analysis found no statistically significant dependence of overall ORs on specific study characteristics except efficacy criteria. Meta-regression found no significant except sample sizes for data on symptomatic improvement. Publication biases were statistically significant.
Conclusion:
TXL seems to be more effective than beta-blockers in treating angina pectoris, on the basis of the eligible RCTs. Further RCTs are warranted to reduce publication bias and verify efficacy.
Introduction
A
TXL was approved as a new drug (drug approval number Z19980015) by the Ministry of Health of China in 1996. 7 According to the Chinese Pharmacopoeia 2010, the recommended dosages of TXL are two to four pills each time (three times daily) given a content of 0.26 g per pill. 8 TXL comprises Radix ginseng, Hirudo species, scorpion, Radix paeoniae Rubra, Periostracum cicadae, Eupolyphaga species, Scolopendra species, sandalwood, Lignum dalbergiae odoriferae, frankincense, spina date seeds, and borneol. 8 Ginseng and its active compound ginsenosides slow down the heart rate and reduce myocardial oxygen consumption. 9 Hirudo species and its active compound hirudin reduce blood viscosity, improve blood circulation, and dilate blood vessels. Eupolyphaga species reduces left ventricular end-diastolic pressure and heart rate. 9 As a result, TXL enhances myocardial contractility, dilates blood vessels, reduces cardiac afterload, and improves myocardial blood supply. 10
Previous systematic reviews studied beta-blockers or TXL in treating angina pectoris but did not compare them head-to-head. Because hundreds of randomized controlled trials (RCTs) comparing TXL with beta-blockers have been published, a systematic review and meta-analysis would be in great demand to synthesize evidence from those RCTs. This study aims to conduct a meta-analysis to compare the efficacy of TXL with that of beta-blockers in treating angina pectoris.
Materials and Methods
The design, implementation, analysis, and reporting of this meta-analysis were in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 11
Search strategies
Databases including PubMed, MEDLINE, Cochrane Library, ScienceDirect, China National Knowledge Infrastructure, WanFang Data, China Master Theses Full-text Database, and China Doctor Dissertations Full-text Database were searched for RCTs on the efficacy of TXL in treating angina pectoris between the inception dates of the databases and 2014 (last search was performed on May 27, 2013). The following search strategy with keywords was used in searching PubMed and other English-language databases: 1. “tongxinluo” 2. “tong-xin-luo” 3. “tong xin luo” 4. 1 OR 2 OR 3
The following search strategy was used in searching the Chinese National Knowledge Infrastructure and other Chinese databases: 1. “tongxinluo” 2. “guanxiabing” [coronary disease] 3. “xinjiaotong” [angina pectoris] 4. 1 IN abstract 5. 2 IN title 6. 3 IN title 7. 4 AND (5 OR 6)
where IN, AND, OR are logical operators for database search.
Study selection
Inclusion criteria for study selection were the following: (1) the participants had and were being treated for angina pectoris, (2) the study design was an RCT; (3) the RCT compared TXL with beta-blockers, and (4) the follow-up period was no less than 4 weeks. Exclusion criteria were the following: (1) duplicated or redundant reports on the same study, (2) studies did not include symptomatic improvement as a major outcome, and (3) the studies were inconsistent or there were discrepancies between methods and results. Figure 1 shows the flow for study selection according to the inclusion and exclusion criteria.

Results of the database search and study selection process. IHD, ischemic heart disease; RCT, randomized controlled trial.
Data extraction and quality assessment
For each of the included studies, the following data were extracted: (1) publication year, (2) sample characteristics, (3) follow-up periods, (4) baseline characteristics of participants between groups, (5) sample sizes, (6) outcome measures, including symptomatic and electrocardiography (ECG) improvement, (7) drug treatments in experimental and control groups, and (8) frequencies of adverse events. The quality of the included studies was assessed according to the Cochrane Collaboration's tool for assessing risk of bias, 12 the Jadad scale, 13 and the refined version of the Jadad scale, the M scale. 3 The Cochrane Collaboration's tool to assess the risk of bias comprises six domains assessed as low risk, high risk, and unclear risk: generation of the allocation sequence, concealment of the allocation sequence, blinding, incomplete outcome data, selective outcome reporting, and other biases. 12 The Jadad scale assesses the methodologic quality of a clinical trial in randomization, blinding, and withdrawals and dropouts. 13 The M scale comprises the Jadad scale plus two additional items: the use of group baselines comparison and the adverse effects description. 14 The quality of evidence was assessed by the grading of recommendation, assessment, development, and evaluation (GRADE) method 14 and was classified into four categories: high, moderate, low, and very low. 15
Efficacy criteria for symptomatic and ECG improvements
For efficacy evaluation, symptomatic improvements should achieve at least 50% (basic) or 80% (significant) reduction in frequency, duration, and severity of angina pain and palpitation. ECG improvements should achieve (1) at least 0.05 mV lowering at the ST segment on ECG (basic) or (2) nearly normal (significant) performance during an exercise test according to the American College of Cardiology/American Heart Association guidelines. 16
Statistical analysis
Overall effect sizes were represented in odds ratios (OR) 17 and 95% confidence intervals (CI). 18 Meta-analysis used the random-effects model, with heterogeneity assessed by chi-square and I 2 tests. 19 Subgroup and sensitivity analyses were conducted according to the publication years, follow-up periods, sample sizes, study quality scores, efficacy criteria, and treatments. Meta-regression 20 was performed to determine possible relationships between the overall effects and such factors as sample sizes, follow-up periods, M scores, and publication years. Funnel plot, 21 the Egger test, 22 and the Begg test 23 were used to assess publication bias. The trim-and-fill method 24 was used to correct funnel plot asymmetry arising from publication bias. Information about adverse events (AEs) of RCTs, including nonreported AEs and types and frequencies of AEs reported, was tabulated for evaluation. The Spearman rank correlation test was performed to determine possible correlation between ORs of symptomatic and ECG improvement. The Mann-Whitney-Wilcoxon test was used to compare two subgroups. The Kruskal-Wallis test was used to compare multiple subgroups at the same time. Bonferroni correction of p-values was performed for multiple comparisons. All statistical analyses were performed with statistical software R. 25 The “metafor” 26 package was used in R for meta-analysis. Any p-values below 0.05 were considered to represent statistically significant findings.
Results
Study selection and characteristics
The search of databases found 2328 records. According to the inclusion and exclusion criteria, 78 RCTs
27
−104
were included in meta-analysis. Figure 1 shows the process of study selection. Table 1 summarizes the main characteristics of the included studies. All included studies with 7424 participants in total were published in Chinese language between 2000 and 2014. The mean sample size was 95.2 (median: 82; 95% CI, 84.6−105.7). The follow-up periods were between 28 and 180 days. Ten RCTs
30
−33,42,49,50,75,81,95
reported participants with stable angina pectoris, and 25 RCTs
28,29,34,35,37,41,46,51,54,55,57,60,64,78,79,82,83,86
–88,90,97,98,100,101
reported participants with unstable angina pectoris. One RCT
86
used single metoprolol as control daily dosage, 31 RCTs
27,28,34,35,37,39,43,47,49,50
–52,54,58,61,64,68,69,71,73,74,79,81
–83,87,89,94,99,102,104
used metoprolol plus other conventional anti-anginal drugs as the control daily dosage, and other RCTs used beta-blockers plus other conventional anti-anginal drugs as the control daily dosage. One RCT
51
selected 6 to 12 TXL pills. Four RCTs
48,86,87,91
selected 6 TXL pills, 31 RCTs
27,29
–31,33
–39,44
–46,56
–58,61,67,69,73,76,78,81,82,84,89,94,99,101,104
selected 9 TXL pills, and other RCTs selected 12 TXL pills as daily dosage for treatment. Dosage details were listed in Supplemental Table 1. (Supplementary materials are available online at
Numbers 1 and 0 in the “Trial date” column mean that study reported or did not report the trial date, respectively. Numbers 1 and 0 in the “Comparable” column mean that the study reported the comparability between the experiment and control groups (1) or did not report that, respectively.
AE, adverse event; SYM, symptomatic improvement; ECG, electrocardiography improvement; TXL, tongxinluo capsule; CG, interventions in control group.
Quality assessment
Table 1 shows the results of quality assessment according to the Jadad and M scales. Eight RCTs 32,45,67,71,83,86,98,99 had a score of 3 according to the Jadad scale, while the other 70 RCTs had a score of 2. According to the M scale, 5 RCTs 36,38,51,74,81 had a score of 2, 5 RCTs 30,31,34,56,79 had a score of 3.5, 24 RCTs 32,35,40,46,49,52,55,59,62,64,65,71,72,75 −77,80,82,85,87,88,95,97,100 had a score of 4, 1 RCT 45 had a score of 4.5, 5 RCTs 67,83,86,98,99 had a score of 5, and the other RCTs had a score of 3. Seventy RCTs 32,36,38,51,61,74,81 did not report baseline comparison of participants in treatment and control groups while 71 included RCTs reported. Twenty-nine RCTs 32,35,40,46,49,52,55,59,61,62,64,65,67,72,75,76,77,80,82,83,85,86,87,88,95,97,98,99,100 reported types and numbers of AEs and other RCTs did not report any AEs. Other six RCTs 30,31,34,45,56,79 did not report complete information about types and numbers of AEs. The results of the quality assessment according to the Cochrane Collaboration's risk of bias tool are shown in Figure 2. The overall quality of the included studies were at low risk of bias.

Quality assessment of randomized controlled trials according to the Cochrane Collaboration's risk of bias tool.
Overall effect sizes
Overall OR of symptomatic improvement was 3.40 (95% CI, 2.97–3.89; Z=17.69; p<0.0001) with non-significant heterogeneity (I 2 =0%, p=0.9999) among the 78 studies with an outcome of symptomatic improvement (Fig. 3 and Table 2). Figure 4 and Table 3 show that the overall OR of ECG improvement was 2.63 (95% CI, 2.29–3.02; Z=13.85; p<0.0001) with non-significant heterogeneity (I 2 =0%; p=0.8602). Both ORs for symptomatic improvement and ECG improvement indicated that TXL was more effective than beta-blockers for treating angina pectoris. The Spearman correlation between symptomatic improvement and ECG improvement in ORs was statistically significant (rho=0.6193; p<0.0001), indicating that symptomatic improvement and ECG improvement corroborated with each other to provide positive evidence. According to GRADE in Table 4, the quality of evidence for overall effect sizes with data on symptomatic improvement was classified as high and the quality of evidence for overall effect sizes with ECG data was classified as moderate.

Forest plot of the symptomatic improvement outcome measure. CI, confidence interval; Neg, negative; OR, odds ratio; Pos, positive.

Forest plot of the electrocardiography improvement outcome measure.
Z and p-value (effect) evaluated the statistics of overall effect; I2 , chi-square, and p-value for heterogeneity were computed to assess heterogeneity.
RCT, randomized controlled trial; OR, odds ratio; CI, confidence interval; CM, Chinese medicine; df, degrees of freedom.
Z and p-value (effect) evaluated the statistics of overall effect; I2 , chi-square, and p-value for heterogeneity were computed to assess heterogeneity.
GRADE, grading of recommendation, assessment, development, and evaluation.
Subgroup and sensitivity analyses
The ORs of the subgroups for both symptomatic improvement (Table 2) and ECG improvement (Table 3) were compared according to study characteristics, including M scores (≤3 or >3), sample sizes (<95 or ≥95), number of authors (1 or >1), years of publication (before or after January 1, 2008), reports of trial dates (yes or no), baseline comparison of participants (yes or no), reports of AEs (yes or no), and follow-up periods (28 days or >28 days); different interventions in the control group (monotherapy with metoprolol, metoprolol with other Western medicines, or beta-blockers with other Western medicines); different improvement criteria (basic or significant); different type of angina pectoris (stable, unstable, or angina); and different daily dosage of TXL (6 pills, 9 pills, or 12 pills).
When the improvement criteria were raised to the significant level from the basic level, the overall results remained effective (i.e., OR>1.9) and statistically significant. The overall OR for symptomatic improvement decreased from 3.40 to 1.90 (95% CI, 1.72–2.10; Z=12.70; p<0.0001). The overall OR for ECG improvement decreased from 2.63 to 1.95 (95% CI, 1.71–2.22; Z=10.04; p<0.0001). This sensitivity test for symptomatic improvement and ECG improvement showed that the overall efficacy of TXL over beta-blockers was still significantly positive even when the improvement standards were raised. There was a statistically significant correlation between the significant improvement in ORs for symptomatic and ECG outcomes (rho=0.3083; p=0.0350). The quality of evidence for overall effect sizes with data on symptomatic improvement and ECG improvement was classified as moderate when the improvement criteria were raised to the significant level (Table 4).
There was no statistically significant difference between ORs of other subgroups. The agreement among the subgroup analysis results on different study characteristics indicated that the efficacies of TXL versus beta-blockers with all included studies were consistently stable.
Meta-regression
Meta-regression was performed between ORs and study characteristics. Table 5 shows no statistically significant or high correlation between efficacies of TXL over beta-blockers and study characteristics.
Publication bias
Funnel plots (Fig. 5) show the presence of publication biases among the included studies. Both the Egger test (symptomatic improvement: t=0.2209, p=0.0044; ECG improvement: t=0.1626, p=0.1084) and the Begg test (symptomatic improvement: Z=2.8375, p=0.0045; ECG improvement: z=1.8697, p=0.0615) indicated statistically significant publication biases. Use of the trim-and-fill method found that on the left side of the funnel plots there should have been 23 missing studies for symptomatic improvement and 10 missing studies for ECG improvement. On the basis of data for symptomatic improvement, the OR was 2.95 (95% CI, 2.70–3.20; Z=17.14; p<0.0001) and heterogeneity was not statistically significant (Q=65.32; p=0.9971) after trim-and-fill adjustment. On the basis of ECG data, the OR was 2.34 (95% CI, 2.08–2.59; Z=13.01; p<0.0001) and heterogeneity was not statistically significant (Q=63.56; p=0.2275) after trim-and-fill adjustment.
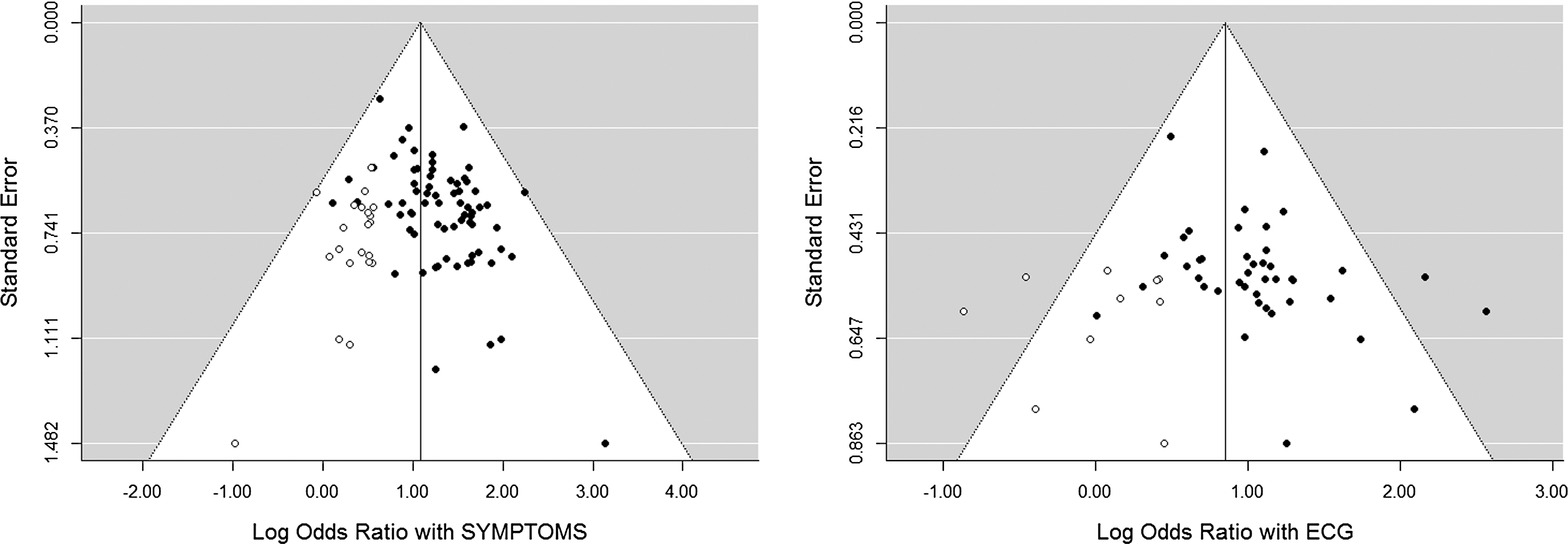
Funnel plots for symptomatic (SYMPTOMS) and electrocardiography (ECG) improvement.
Adverse events
Table 6 listed the information about AEs. All AEs were minor or well tolerated; none caused dropouts except in one study, 45 in which two participants dropped out because of severe stomachache and abdominal distention. Nineteen studies reported that 56 participants in total had epigastric discomfort. Epigastric discomfort, flush, and headache were the top three AEs reported in the control groups. Thirty studies reported AEs and 42 studies did not report any AEs. The other five studies reported that 45 participants in total had epigastric discomfort. Overall, AEs of TXL were more frequent and severe than those of the control drugs.
The other five RCTs reported 45 participants with epigastric discomfort.
NR, not reported.
Discussion
This analysis of 78 RCTs with 3812 participants in a treatment group and 3612 participants in a control group is the first PRISMA-compliant systematic review on the efficacy of TXL versus beta-blockers in treating angina pectoris. Overall ORs of symptomatic improvement and ECG improvement were 3.40 (95% CI, 2.97–3.89; Z=17.69; p<0.0001) and 2.63 (95% CI, 2.29–3.02; Z=13.85; p<0.0001), respectively. There was no significant heterogeneity among the 78 RCTs with data on symptomatic improvement (I2 =0%; p=0.9999) and the 47 RCTs with data on ECG improvement (I2 =0%; p=0.8526). Subgroup and sensitivity analyses on various features, such as study quality, sample sizes, follow-up periods, improvement criteria, and interventions, demonstrated that the efficacy findings were consistent. Meta-regression analysis showed no significant correlations between the selected features and overall efficacies. The Egger test, Begg test, and trim-and-fill method found significant publication biases. After trim-and-fill adjustment to cope with publication biases, the adjusted overall efficacy of TXL was still more effective than that of beta-blockers in treating angina pectoris.
Although the efficacy of TXL was improved as the daily dosages increase (6 pills, 9 pills, and 12 pills) for both symptomatic improvement (OR, 2.99, 3.20, and 3.60) and ECG improvement (OR, 3.29, 2.30, and 2.70) as outcome measures (Tables 2 and 3), there was no significant difference in subgroups between symptomatic improvement (chi-square=0.1475; p=0. 0.9289) and ECG improvement (chi-square=0.2030; p=0.9035).
Beta-blockers could not be analyzed individually because of sparse data. Further RCTs are warranted to compare the efficacies among beta-blockers. The overall ORs are higher than 1 no matter how categories RCTs are grouped and outcome measures used.
Low quality of the included RCTs is a major limitation in this meta-analysis, although the overall findings were consistent with those of previous studies. 105 –108 While all studies were described as RCTs, only 6 studies 44,66,70,82,97,98 used randomization procedures. Two studies 31,85 were described as single blind. Only one RCT 44 clearly reported having dropouts. The mean Jadad score was 2.10 (median, 2.00; 95% CI, 2.04–2.17) and the mean M score was 3.42 (median, 3.00; 95% CI, 3.27–3.58). As such, high-quality RCTs would be necessary for this meta-analysis to draw a positive conclusion.
All included RCTs were conducted in China and reported in Chinese journals. The follow-up period of 53 RCTs was 28 days and the mean follow-up period of 78 RCTs was 42 days. Such short follow-up periods for patients with angina pectoris could not support the efficacy of longer treatment with TXL. The mean sample size of 95 was small. Thirty-eight RCTs did not report AEs at all, and others did not report AEs formally.
In conclusion, TXL seems to be more effective than beta-blockers in treating angina pectoris, according to the eligible RCTs. Further RCTs are warranted to reduce publication bias and verify efficacy.
Footnotes
Acknowledgments
The work of both authors was supported by research grants (MYRG190-Y3-L3-ICMS11-LSW and MYRG2014-00117-ICMS-QRCM) from the University of Macau.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.