
Abstract
Objective:
Postoperative pain is caused by surgical injury and trauma; is stressful to patients; and includes a series of physiologic, psychological, and behavioral reactions. Effective postoperative analgesia helps improve postoperative pain, perioperative safety, and hospital discharge rates. This study aimed to observe the influence of postoperative intravenous sufentanil patient-controlled analgesia combined with music therapy versus sufentanil alone on hemodynamics and analgesia in patients with lung cancer.
Methods:
This was a randomized parallel study performed in 60 patients in American Society of Anesthesiologists class I or II undergoing lung cancer resection at the Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University. Patients were randomly assigned to a music therapy (MT) group and a control (C) group. The MT group underwent preoperative and postoperative music intervention while the C group did not. Both groups received intravenous patient-controlled sufentanil analgesia. The primary outcome was the visual analogue scale (VAS) score at 24 hours after surgery. The secondary outcomes included hemodynamic changes (systolic blood pressure, diastolic blood pressure, heart rate), changes on the Self-Rating Anxiety Scale (SAS), total consumption of sufentanil, number of uses, sedation, and adverse effects. The postoperative sufentanil dose and analgesia frequency were recorded.
Results:
Compared with the C group, the MT group had significantly lower VAS score, systolic and diastolic blood pressure, heart rate, and SAS score within 24 hours after surgery (p < 0.01). In addition, postoperative analgesia frequency and sufentanil dose were reduced in the MT group (p < 0.01).
Conclusions:
Combined music therapy and sufentanil improves intravenous patient-controlled analgesia effects compared with sufentanil alone after lung cancer surgery. Lower doses of sufentanil could be administered to more effectively improve patients' cardiovascular parameters.
Introduction
P
Comprehensive pain management in cancer seeks to address distressing and problematic symptoms to improve patient quality of life and peace of mind. Recently, a novel therapeutic approach in palliative and postoperative surgical care for patients with cancer adopted patient-specific music medicine or music therapy (MT) interventions. 9,10 In music medicine interventions, patients listen to prerecorded music, managed by health care specialists, and are carefully preselected by study researchers who might not be formally trained in MT. 11 Music medicine requires only a stimulus and a response, whereas MT involves a therapeutic effect based on individual patient assessment, treatment, and subsequent evaluation. 11 Studies support the use of music as an intervention to dampen subjective pain and in acute pain management. 12
Some previous studies have shown that interventions combining MT and opioids promoted a synergistic analgesic effect on the opioid and reduced the required opioid dose to induce the same effects while reducing adverse effects. 13 –15
No previous study appears to have reported the effects of combining MT to intravenous patient-controlled analgesia (PCA) in patients with lung cancer after surgical resection. The objective of this study was to observe the outcomes of intravenous sufentanil PCA combined with MT in postoperative patients with lung cancer to establish whether MT could indeed improve pain management in these cancer.
Materials and Methods
Patients
This study was conducted at the Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, China, from March 2013 to January 2014. Inclusion criteria were (1) highly suspicious lung cancer according to clinical and radiologic findings, (2) stage I or II cancer, (3) tumor size of 2–3 cm, 4) American Society of Anesthesiologists class I or II, and (5) plan to undergo surgery. Exclusion criteria were (1) history of allergic reaction to opioids, (2) blood coagulation dysfunction, (3) asthma, (4) peptic ulcers, (5) liver or kidney disease, (6) hearing impairment, (7) history of alcohol or drug abuse, (8) any known mental illness or memory dysfunction, (9) inability to operate PCA, (10) severe high blood pressure or heart disease, or (11) professional musical background.
The local Ethics Committee of the Affiliated Cancer Hospital of Xiangya School of Medicine, Central South University, approved this study. All participants provided written informed consent prior to study participation.
Study design
Consecutive patients were recruited and randomly assigned to the MT group and control (C) group by using a random-numbers table and sealed sequential envelopes prepared by an independent statistician. One W.Y. recruited and registered the patients. L.J. allocated the patients and Y.W. recorded the data. There was no blinding.
One day before the operation, study investigators/therapists explained how to operate the PCA device and use the Self-Rating Anxiety Scale (SAS) and visual analogue scale (VAS) to all patients. Additionally, interviews were performed to evaluate the patients' educational (e.g., educational history, career, language) and musical (favorite music type, interest, and frequency of listening to music) background. The main music selected by the therapist was the patient's favorite, as established through joint discussion after evaluation. The music therapy scheme was cooperatively determined by the patient and the therapist. Patients fasted for at least 8 hours before the operation and were intravenously injected with 0.8 mg of penehyclidine 30 minutes before surgery.
Music intervention method
The music relaxation and music meditation methods were used in the MT group; these combined music listening with music imagination technology in a personalized way. Specific music intervention operations were as follows: (1) before surgery, the music therapist implemented music-assisted progressive muscle relaxation for 15 minutes; the therapist guided the patient to enter light and moderate hypnosis with language accompanied by relaxing music; (2) the music intervention ceased during the operation, and the music therapist departed the operating room; (3) at 3, 7, 15, and 19 hours after the patients entered the intensive care unit, the music therapist implemented music intervention for 1 hour each time.
The music therapist guided the patients in the whole process of music imagination with the guiding music meditation method. The therapist always controlled the music material selection and switching and pre-established the imagination situation. The music therapist also paid close attention to the patients' development of the imagination process. The patients listened to the music under the same therapist's guidance throughout the whole study.
For the relaxation phase, the music therapists selected new-age music without a defined melody. In the music-guided imagery step, the music was selected by the therapist after discussion with the patient and according to the comprehensive evaluation. In the process of intervention, the therapist could change the music at any time according to the mood of the patient. All selected music and songs were without lyrics. All music interventions were tailored to each patient. On the day before the operation, 8–12 tunes were selected by the music therapist to develop this strategy. The MT group was treated before and after the operation.
Music material were as follows: relaxing music (“The Stream,” “The Sea,” “The Mountain,” and “The Prairie” provided by the Beijing Gaotian music mental health research center) and music imagination (“A Lover's Concerto” from Johann Sebastian Bach, “Annie's Wonderland” from Bandari, “A Moonlit Night on the Spring River,” “Song of the Homebound Fishermen” and “Shepherd Boy's Piccolo” from ancient Chinese melodies; “The Enchanting Forest” from Wu Jindai; “Yao's Dance Music” from Zhu Longtao; “The Shining Tashikuergan” and “Morning of Miao Mountain” from Chinese famous violin music; “Horse Racing” from Chinese Erhu music; “Yun Shui Yin” and “Heart of Heaven” from Chinese Buddhist music).
After surgery, hemodynamics, VAS, and sedation score were used to choose the music at each intervention point. If the music could ease pain and anxiety without increasing hemodynamics, the intervention music remained unchanged.
Anesthesia and analgesia
Blood pressure (BP), heart rate (HR), pulse oxygen saturation (SpO2), and partial pressure of carbon dioxide in end expiratory gas (PetCO2) were monitored after the patients entered the operating room. The upper extremity vein was punctured for infusion of sodium lactate Ringer's solution. For anesthesia induction, the following intravenous formula was used: 0.1 mg/kg of midazolam, 0.6 mg/kg of propofol, and 0.4 μg/kg of sufentanil. After patients were confirmed as being anesthetized, 0.1 mg/kg of vecuronium bromide was injected, and mechanical ventilation was implemented through orotracheal intubation with a tidal volume set at 8–10 mL/kg. For anesthesia maintenance, remifentanil at 0.1–0.2 μg/kg per minute and propofol at 6–8 mg/kg per hour were continuously and intravenously infused. Vecuronium bromide was intermittently injected to maintain muscle relaxation. The anesthesia depth was adjusted by altering the infusion speed of propofol and remifentanil. If low BP was observed (i.e., a systolic BP [SBP] ≤80 mmHg for more than 1 minute), the patient was brought out of anesthesia; corrections were first made by speeding up infusion or infusing 6% hydroxyethyl starch. If such correction was inefficient, 5–10 mg of ephedrine was injected. In the case of bradycardia (i.e., heart rate ≤55 beats/min), 0.5–1 mg of atropine was injected. All anesthetic drugs were withdrawn at the end of the operation. After entering the intensive care unit, 0.5 mg of atropine and 1 mg of neostigmine were given to antagonize the residual effects of the muscle relaxant. When the patients were conscious and their spontaneous breathing recovered satisfactorily, they were extubated and underwent postoperative PCA using intravenous PCA pumps (Tuoren Group Co., Ltd, Xinxiang, China).
The analgesic PCA drug formulation was 2 μg/kg of sufentanil (Yichang Humanwell Pharmaceutical Co., Ltd, Yichang, China) in 100 mL of normal saline administered as a single 2-mL dose, a 10-minute locking time, and a background input quantity of 0.5 mL/h. A VAS score <4 meant that analgesia was effective, and PCA was withdrawn within 24 hours. If the VAS score was >4, the patients were injected with 50 mg of tramadol in a single bolus dose for prompt pain relief.
Observational indices
The primary outcome was the VAS score at 24 hours after surgery. The secondary outcomes included hemodynamic changes (SBP, diastolic BP [DBP], and HR), SAS changes, sufentanil total consumption, number of uses, sedation, and side effects. The main outcome was assessed at 4, 8, 12, 16, 20, and 24 hours after surgery. The total consumption of sufentanil and the number of uses were assessed according to the PCA recording data 24 hours later.
After the Aldrete score (the Aldrete score is also known as the post-anesthesia recovery score and is provided to evaluate postoperative activity, breathing, circulation, and hypoxia performance) was ≥9, the degree of satisfaction among all patients was evaluated by using a VAS (0 means satisfactory, and 10 means very dissatisfactory). The degree of postoperative pain was also evaluated by using a VAS (0, painless; 1–3, mild pain; 4–6, moderate pain; 7–10, severe pain). The postoperative anxiety state was evaluated by using the SAS questionnaire (<50, no anxiety; 50–59, mild anxiety; 60–69, moderate anxiety; and >70, severe anxiety).
Measurements of SBP, DBP, HR, SpO2, respiratory rate, SAS score, VAS score, drug dose, and total consumption of sufentanil at 4, 8, 12, 16, 20, and 24 hours were recorded postoperatively. At the same time, adverse reactions, such as sedation (i.e., sedation scores of 1, 2, 3, and 4), nausea, vomiting, and itching, were recorded at 4, 8, 12, 16, 20, and 24 hours after surgery. All postoperative measurements were evaluated and confirmed by two independent observers. Observations were compared between them, and differences were solved by discussion.
Statistical analysis
No previous study were available from which to obtain data for a reliable power analysis. Therefore, the size of the groups was arbitrarily set at 30 patients. Statistical analyses were performed by using SPSS software for Windows, version 11.5 (SPSS Inc., Chicago, IL). Continuous variables are presented as mean ± standard deviation and were analyzed by using the independent samples t-test for intergroup comparisons and repeated- measures continuous analysis of variance with the Tukey post hoc text for intragroup comparisons. Categorical variables are presented as frequencies and were analyzed by using the Pearson chi-square test. A p-value <0.05 was considered to represent a statistically significant difference.
Results
Characteristics of the patients
Sixty patients were recruited (35 men and 25 women), aged 35–69 years, with a body weight range of 45–80 kg. Thirty patients (18 men and 12 women) aged 53.8 ± 11.2 years were included in the C group, and 30 (17 men and 13 women) aged 53.5 ± 10.7 years were included in the MT group. ASA grade, sex, age, body weight, and operation duration did not significantly differ between the two groups (p > 0.05) (Table 1), nor did the patients' musical background (p > 0.05) (Table 2). All patients in the MT group completed the whole course of music interventions. No adverse reaction related to MT occurred.
Unless otherwise noted, values are the mean ± standard deviation.
Independent samples t-test.
ASA, American Society of Anesthesiologists.
Unless otherwise noted, values are the number of patients.
Chi-square test.
NS, not significant.
Postoperative VAS and SAS scores at each time point
Compared with scores in the C group, the postoperative VAS and SAS scores in the MT group were significantly lower at each time point (all p < 0.05) (Fig. 1).
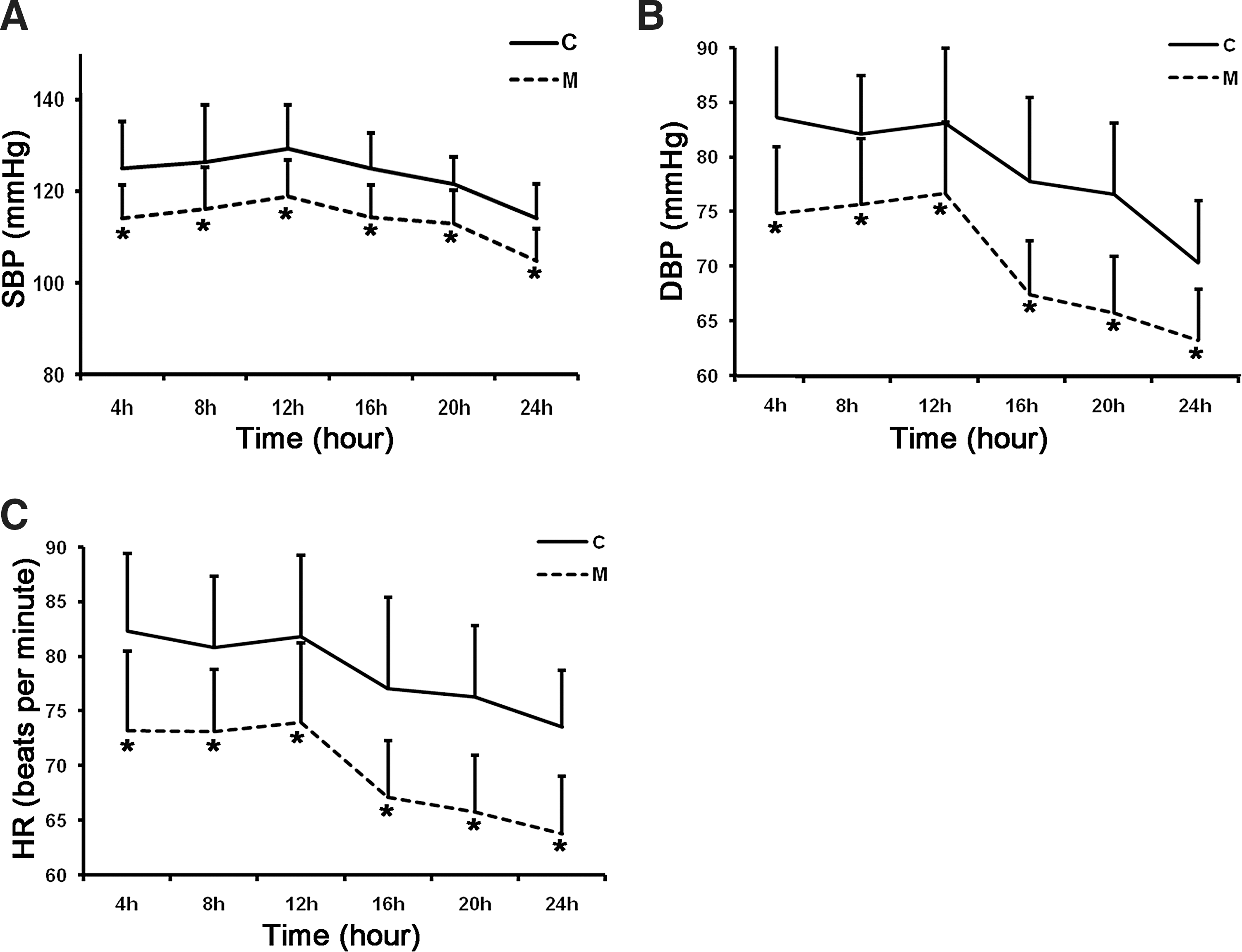
Comparison of hemodynamic changes between the music (M) therapy group and control (C) group at postoperative time points. *Compared with control group at each time point, p < 0.01.
Hemodynamics at each time point
Compared with values in the C group, postoperative SBP, DBP, and HR in the MT group were lower at each time point (all p < 0.05) (Fig. 2).
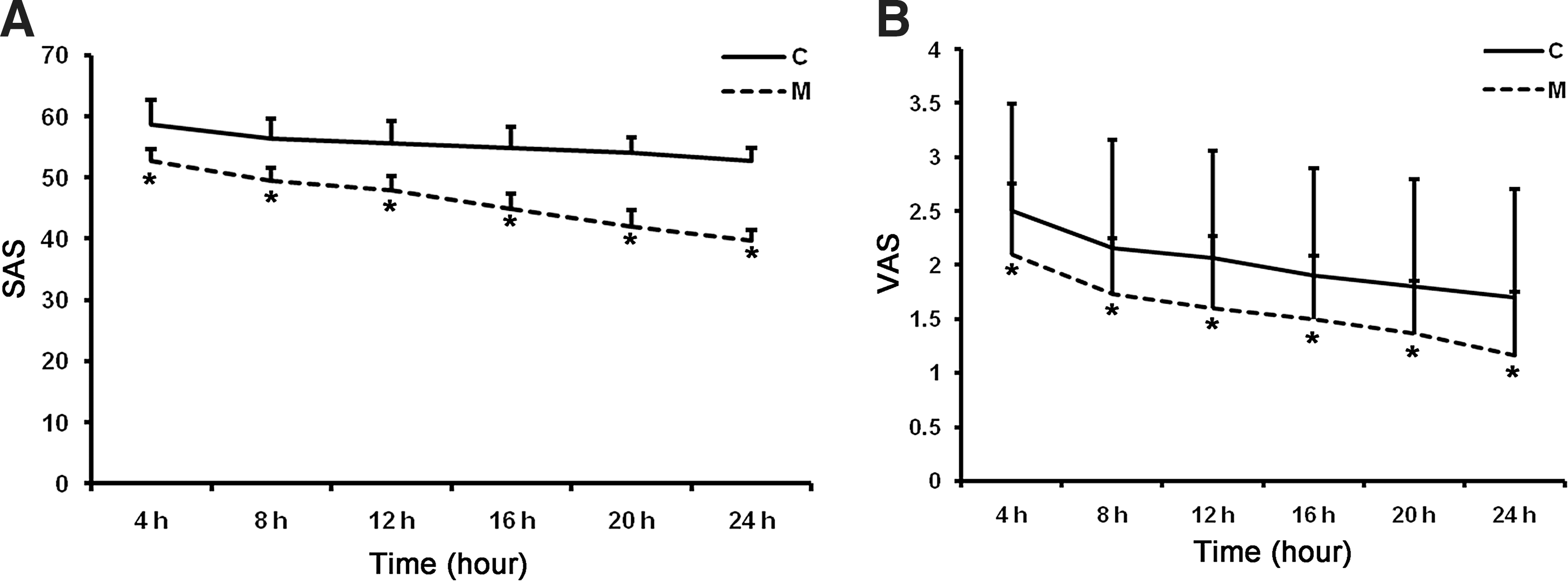
Comparison of the Self-Rating Anxiety Scale (SAS) scores and visual analog scale (VAS) scores between the music therapy group and control group at postoperative time points.
Sufentanil consumption and adverse reactions
Compared with values in the C group, the postoperative total consumption of sufentanil (82.65 ± 6.19 μg in the C group versus 52.68 ± 7.07 μg in the MT group; p < 0.001) and PCA use frequency (31.0 ± 4.0 in the C group versus 19.1 ± 3.5 in the MT group; p < 0.001) in the MT group were decreased significantly (Table 3). Two of 30 patients in the C group required additional tramadol analgesia compared with no patients in the MT group. Five patients in the C group and one in the MT group had nausea and vomiting. There were two cases of pruritus in the C group and none in the MT group (Table 3).
Unless otherwise noted, values are the mean ± standard deviation.
Independent samples t-test.
PCA, personal-controlled analgesia.
Discussion
This study observed the analgesic effects and influence on hemodynamic changes of intravenous PCA combined with MT and sufentanil after surgical resection of lung cancer. The research findings showed that combining MT and sufentanil significantly reduced pain and anxiety within 24 hours of surgery and postoperative analgesic drug consumption. This approach also reduced SBP, DBP, and HR within 24 hours of surgery, thus permitting better hemodynamic parameter stabilization.
Sufentanil has a stronger analgesic effects than fentanyl 5 and is characterized by mild respiratory depression and more stable hemodynamics compared with fentanyl and morphine. 6 –8 The present study showed that this agent had a significant postoperative intravenous analgesic effect in the context of postoperative intravenous sufentanil PCA. However, the postoperative SAS score was higher, as was the total sufentanil consumption. In addition, the PCA use frequency was high, and two patients needed additional analgesics. Some patients experienced vomiting (16.0%) and pruritus (6.6%).
Music not only has extensive, profound social functions and prominent aesthetic educational functions but also provides entertainment and rest. Music and songs can improve patients' physical and mental health, physical and mental well-being, cognitive and social ability, and physical and mental pain. 16 Sweet music provides a benign brain stimulation, allows the patients' body and mind to be relaxed completely, and increases pain tolerance. 13 Patients' acoustic stimuli caused by listening to music can affect their adaptation to stress response, discomforting or unfamiliar environment, uncontrollable mood, and fear of operative wounds. After listening to sweet music, patient moods can be calmed. Researchers suggested that pain and sweet auditory pathways are mutually inhibited, and acoustic stimuli caused by music can inhibit the central transmission of pain and produce analgesic effects. 13,17,18
Studies have shown that 30-minute postoperative MT could result in postoperative analgesia for 1 hour in patients after cesarean delivery and reduce postoperative analgesic drug requirements. 13 Nillsson et al. 17 observed that MT for 1 hour could reduce postoperative pain and morphine consumption. Some studies also showed that perioperative music therapy could produce a postoperative analgesic effect and reduce postoperative analgesic drug requirements. 19 Of course, the effects of MT on postoperative pain are controversial. 20 The results of the present study suggest that the patients in the MT group had a superior analgesic effect along with reduced doses of sufentanil. The net outcome was that postoperative adverse reactions were decreased, suggesting that MT can promote mood relaxation in patients. Music therapists guide and encourage patients to concentrate on the music and to follow the music so that the patients themselves have a more active role in pain control. At the same time, music is involved in cognitive pain control as the information carrier, which helps patients to relieve their physical and mental pain.
Many studies reported the influence of MT on patient hemodynamics following surgery. A meta-analysis by Loomba et al. 21 has shown that MT could reduce patient anxiety caused by the operation through relaxing the physiologic and mental state, thereby significantly reducing SBP, DBP, and HR. Anxiety is a common preoperative symptom, and it can interfere with sleep and enjoyment of life, social relationships, and general daily activities. Indeed, a large-scale study in the United States (535 million surgical operations in 347 million outpatients) showed that preoperative anxiety was frequent. 22 Such moods could clearly affect their postoperative recovery and increase the risk of complications. 21 This could significantly reduce postoperative vomiting, pain, and patient recovery time. Likewise, properly reducing hospitalized patients' preoperative anxiety can also significantly reduce their hospital stay, incidence of postoperative fever, and need for sedation and analgesia. 21
This study has many limitations. Observations and conclusions were drawn from a relatively small subset of patients. In addition, future studies should assess MT in settings of acute versus chronic pain. Comparative analysis should also be made of preoperative and postoperative responses to the frequency, duration, and type of intervention, which this study did not explore.
In conclusion, the present study suggests that intravenous sufentanil PCA combined with MT after lung cancer resection led to improved analgesia and hemodynamics compared with sufentanil alone. The required dose of sufentanil was reduced, as was the incidence of adverse effects. In addition, this approach could be effective in reducing BP, HR, stress, and anxiety and improving well-being and quality of life. More detailed studies are necessary to clarify the postoperative analgesia mechanism of MT.
Footnotes
Acknowledgments
The authors would like to thank the participants and hospital staff for their contributions to this study. The study was funded by grant no. 2012FJ2004 from the Department of Science and Technology of Hunan Province, China.
Author Disclosure Statement
No competing financial interests exist.