
Abstract
Objective:
To evaluate the immediate effect of acupuncture on cortico spinal tract (CST) activity in patients with chronic disorders of consciousness (DOC) after traumatic brain injury (TBI) by measuring motor-evoked potential (MEP) using transcranial magnetic stimulation (TMS).
Design:
Changes in several variables in the acupuncture session were compared with those in the control session without acupuncture in the same patients.
Setting:
Chubu Medical Center for Prolonged Traumatic Brain Dysfunction, Gifu, Japan.
Patients:
Fourteen patients (mean age ± standard deviation, 39 ± 17 years; 12 men) with chronic DOC (5 in a vegetative state and 9 in a minimally conscious state) following severe TBI.
Intervention:
Acupuncture treatment was performed at GV 26, Ex-HN 3, bilateral LI 4, and ST 36 for 10 minutes.
Outcome measures:
Main outcome measure was MEP amplitude. MEP amplitude, measured by using TMS on the primary motor cortex, was recorded from the abductor pollicis brevis muscle. MEP recordings were performed before acupuncture (baseline), 10 minutes after needle insertion (phase 1), and 10 minutes after needle removal (phase 2). As a control, the same procedure without acupuncture was performed on another day with the order randomized. MEP amplitude and latency were calculated. Evoked F-wave measurements were also performed to calculate maximum M-wave amplitude (Mmax), M-wave latency, and F-wave latency in the same muscle. Central motor conduction time (CMCT) and MEP/Mmax ratio were also calculated from the MEP and F-wave measurement data.
Results:
MEP amplitude and MEP/Mmax were increased significantly in the acupuncture session at phases 1 and 2 compared with the control session (p < 0.001, p < 0.001, p < 0.001, and p = 0.001, respectively). CMCTs were reduced at phases 1 and 2 in the acupuncture session compared with the control session, and the change at phase 1 was statistically significant (P = 0.002).
Conclusions:
Acupuncture treatment increased the CST activity of patients with chronic DOC after severe TBI.
Introduction
F
It is difficult to assess motor dysfunction in patients with DOC by physical examination because of their severe DOC. Motor evoked potentials (MEPs) using transcranial magnetic stimulation (TMS) is a useful tool for the measurement of motor response in DOC. 4 MEP using TMS is a less invasive, generally pain-free, objective indicator to assess motor cortex excitability and integrity of motor pathways in various disease states, including DOC. 5 –7 In typical TMS experiments, stimulation is delivered to the primary motor cortex, and MEP is recorded from a muscle by using surface electromyography electrodes. TMS is thought to activate the corticospinal neurons transsynaptically. MEP is altered in patients with DOC and motor disturbances after cerebral insult (e.g., lower MEP amplitude, higher resting motor threshold, and prolonged latency and central motor conduction time [CMCT] compared with healthy controls). 8 –12
Acupuncture treatment is a part of traditional Eastern medicine developed in Asia. During acupuncture treatment, stimulation with acupuncture needles on acupuncture points leads to improvement of various symptoms. In some case reports, acupuncture treatment has been reported to be beneficial for DOC. 13 –17 Patients with DOC sometimes show motor responses, even if the responses are unclear or inconsistent. In the authors' clinical experience, spontaneous movements of the finger and neck with pursuit have been observed and increased in patients with DOC during and after acupuncture treatment, although these motor responses were slight and could not be quantitated in most cases. Acupuncture and electroacupuncture point stimulation have been reported to alter motor cortex excitability as measured by MEP using TMS in healthy persons and stroke patients. 18 –21 There appear to be no reports investigating the effects of acupuncture on patients with DOC following TBI using TMS.
The study hypothesis was that acupuncture treatment would increase the excitability of the cortico-spinal tract (CST), which can be evaluated by MEP using TMS, leading to a therapeutic effect in patients with DOC. The aim of this study was to investigate the immediate effects of acupuncture treatment on excitability of the CST in patients with DOC following severe TBI.
Materials and Methods
Setting
This study was performed in an examination room in Chubu Medical Center for Prolonged Traumatic Brain Dysfunction, Gifu, Japan. This center is a special hospital for patients with chronic DOC due to TBI following a traffic accident.
Study design
Changes in variables in the acupuncture session were compared with those in the control session under a resting state without acupuncture on another day. Acupuncture and control sessions were performed in random order. Each session was separated by at least a 3-day interval. The time course is shown in Figure 1. This study was approved by the Ethics Committee of the Kizawa Memorial Hospital, and written informed consent was obtained from each patient's legal guardian in accordance with the Helsinki declaration.
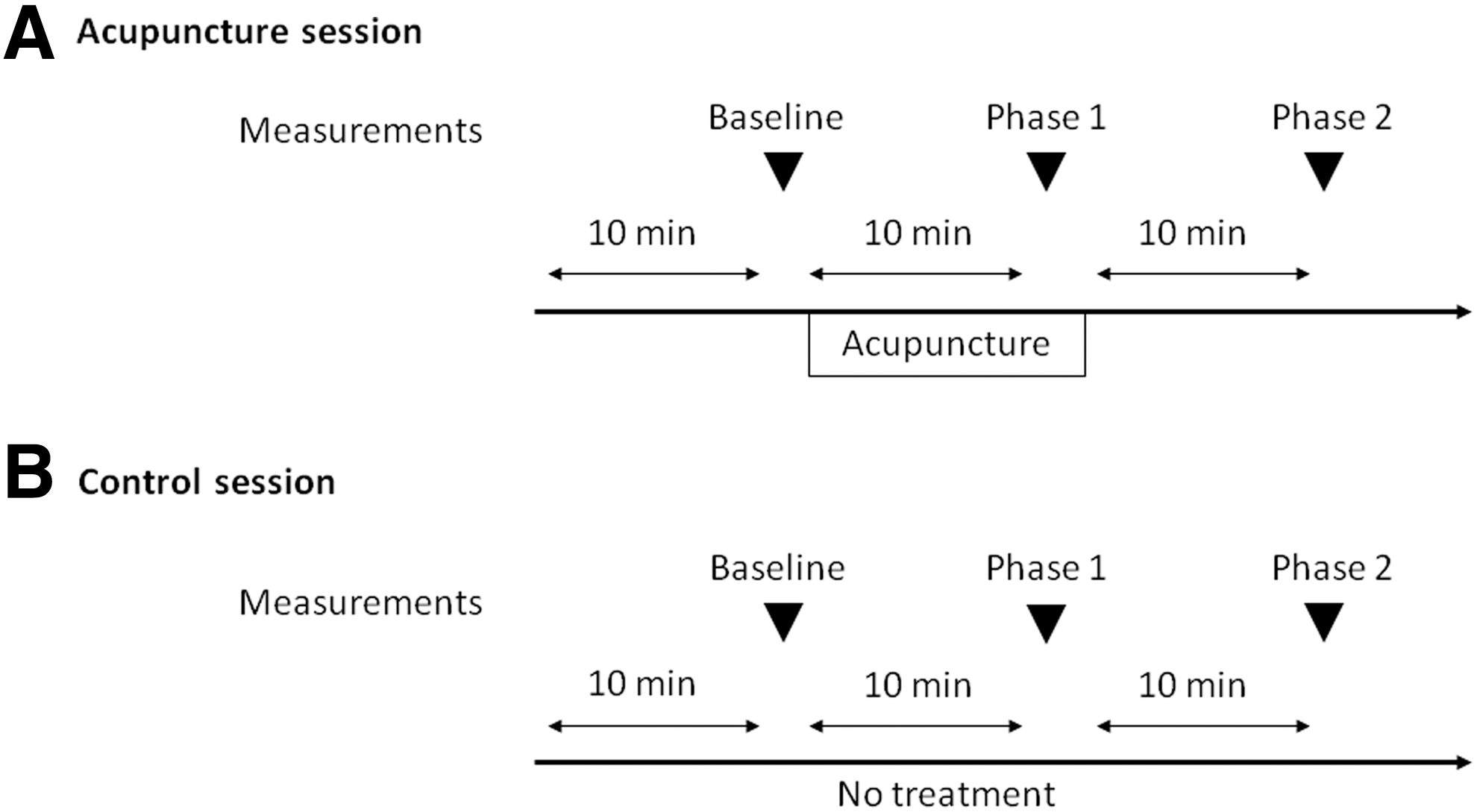
Time course of the study. Acupuncture session
Participants
Fourteen Japanese patients (12 men and 2 women; 5 with VS and 9 with MCS) with chronic DOC following severe TBI due to a traffic accident were enrolled. The patient characteristics are shown in Table 1. The median (first and third quartiles) age was 34 (24, 56) years. Median (first and third quartiles) durations after injury and after admission to our hospital were 18 (12, 24) months and 8 (4, 13) months, respectively. TBI diagnosis, obtained by using computed tomography and magnetic resonance imaging, included a combination of diffused axonal injury (DAI) and contusion (n = 8); contusion (n = 4); a combination of DAI and traumatic subarachnoid hemorrhage (SAH) (n = 1); and a combination of DAI, contusion, and traumatic SAH (n = 1). The following types of patients were excluded from this study: (1) patients with an implanted pacemaker or intracranial ferromagnetic material, (2) patients receiving intrathecal baclofen therapy, (3) patients in whom MEP could not be elicited in both hemispheres on routine TMS examinations upon admission to the study hospital, and (4) patients with a history of convulsive attack induced by TMS.
Data are shown as the number of cases or median (first and third quartiles).
Medication: Five patients received a combination of two or more of these drugs.
DOC, disorder of consciousness; VS, vegetative state; MCS, minimally conscious state; DAI, diffused axon injury; SAH, subarachnoid hemorrhage; CNS, central nervous system.
Five patients took medications that influenced the central nervous system or muscle tone (anticonvulsant or antispasticity drugs), and 5 patients received a combination of 2 or more of these drugs and antiparkinson agents. The administration of these drugs could not be stopped for clinical reasons. No sedative medication was administered before the TMS measurement.
Intervention
During the acupuncture session, sterilized stainless disposable needles (0.16 mm in diameter, 40 mm in length) (SEIRIN Co. Ltd., Shizuoka, Japan) were used. Six acupuncture points, consisting of GV 26, Ex-HN 3, bilateral LI 4, and ST36, were used. GV 26 is located on the midpoint of the philtrum midline. LI 4 is located on the dorsum of the hand, on the radial side in the middle of the second metacarpal bone. ST 36 is located on the anterior aspect of the leg, on the tibial anterior muscle. Details of the locations of these points are indicated in the World Health Organization acupuncture point guideline. 22 These acupuncture points were chosen in consideration of the effects on brain activation according to Traditional Chinese Medicine theory, according to some previous reports 13 –18,20,23 –27 and the authors' clinical experiences. GV 26, LI 4, and ST 36 have been used for patients with DOC. 13 –17 LI 4 and ST 36 have been used for motor recovery after ischemic stroke. 25 LI 4 and ST 36 have also been reported to modulate CST activity. 18,20 LI 4, ST 36, and Ex-HN 3 were used in previous molecular imaging study for neurologic disease. 24 GV 26 has been considered a life-saving point according to Traditional Chinese Medicine theory and has been reported to reduce the central nervous depressive activity in rabbits. 26 GV 26 also has been used for resuscitation and recovery from unconsciousness. 27
Acupuncture needles were inserted into these acupuncture points at depths of about 4–20 mm in patients in the resting supine position and were left for 10 minutes without manipulation. These methods of acupuncture stimulation, including treatment time and manipulation, were chosen according to clinical experiences, such as the observation of increasing motor responses (including finger and/or neck movement) during acupuncture treatment for patients with DOC. Treatments were applied by one acupuncturist who had a national license and 9 years of practical experience.
In control sessions conduced on a separate day, patients rested in the supine position but no treatments were performed.
Outcome measurements
For the electrophysiologic studies, the participants relaxed in the supine position in an air-conditioned examination room. MEP was obtained from the abductor pollicis brevis (APB) muscle using pairs of standard Ag/AgCl electrodes by TMS on the contralateral primary motor area (upper limb area). TMS was performed by neurosurgeons. Although participants enrolled in this study had DOC, they were instructed to keep their hands relaxed, and the electromyography (EMG) activity in the target muscle was monitored to confirm complete muscle relaxation. For recording MEP, only one examination side was chosen on the basis of which side presented a larger or clearer motor response according to clinical impression and MEP when patients received routine examinations upon admission to our hospital (right side: 8 cases; left side: 6 cases).
The maximum stimulation strength of the magnetic field produced by the stimulator (SMN1200; Nihon Koden Co., Tokyo, Japan) used for TMS was 1.27 Tesla per single pulse of 90 μsec. A single, round coil 120 mm diameter (YM-121B; Nihon Koden Co.) was connected to the stimulator and used for TMS. MEP was obtained and analyzed by using a Neuropack MEB 2200 recorder (Nihon Koden Co.) with a band pass of 20 Hz to 1 kHz. The site of TMS application, at which the coil was placed tangentially, was over the convexity located about 5 cm laterally and 1 cm anteriorly to the cortical electrode location Cz. 28 This site and adjacent positions were stimulated by TMS in order to seek the hot spot at which maximum MEP was obtained. The right cerebral hemisphere was stimulated with a clockwise current flow and the left hemisphere with a counterclockwise current flow. The hot spot was marked directly on the scalp to ensure constant coil position during the entire experimental session. After the hot spot was decided on for each patient, TMS intensity was increased in 10% intervals from 10% to 100% of maximum stimulator output (MSO) to determine the resting motor threshold (RMT). The RMT was defined as the minimum stimulus intensity to elicit MEP with a peak to peak amplitude of 50 μV or greater in 2 of 4 attempts. Stimulation intensity was set at the RMT plus 20% of MSO. Ten consecutive TMS events (stimulation interval of 10 seconds) were performed. MEP amplitude was defined as the peak-to-peak amplitude (Fig. 2). Mean amplitude and latency were calculated. To avoid a possible bias due to outliers, the average of 8 of 10 MEPs, excluding maximum and minimum values, were used for the calculation.

Motor-evoked potential wave.
In the acupuncture session, baseline MEP was obtained in patients in the resting supine position after 10 minutes of rest. Then, patients received 10 minutes of acupuncture treatment. MEP at phase 1 was recorded before acupuncture needle removal. MEP at phase 2 was recorded 10 minutes after removal of acupuncture needles (Fig. 1). In MEP measurements at phase 1 and phase 2, 10 consecutive TMSs (same intensity as baseline) were applied after seeking RMT. In the control session, MEP recordings using the same procedure were performed every 10 minutes without acupuncture treatment.
Elicited F-wave measurement was used to calculate the maximal M-wave (Mmax) amplitude, peripheral motor conduction time (PMCT), and central motor conduction time (CMCT). F waves were recorded from the APB muscle on the same side in the same time course as MEP measurements on separate days. F-wave recording was obtained by using a Neuropack MEB 2200 recorder with a band-pass filter of 50 Hz to 3 kHz, and the sensitivity was set at 2 mV and 200 μV per division for recording compound muscle action potentials (M wave) and F wave.
M waves were elicited by orthodromic activation of motor neurons and F waves were elicited by antidromic activation, reflecting backfire. Sixteen F waves obtained by electric stimulation of the median nerve were recorded from the APB muscle. The stimulus intensity to elicit F waves was 120% of that required to elicit a maximal M wave. Electric stimulus rate was 1 Hz and duration was 0.2 millisecond. The EMG electrode was attached firmly over the APB muscle. The median nerve was stimulated with a rigid bar electrode strapped securely at the wrist with the cathode positioned proximally. The ground electrode was placed between the stimulating and recording electrodes.
F wave was defined as a response with peak-to-peak amplitude of at least 50 μV. The Mmax was also calculated from peak-to-peak amplitude. The ratio of MEP amplitude and Mmax amplitude (MEP/Mmax) was calculated. PMCT was measured as the latency of the response from the spinal cord to the muscle, calculated by using the formula (F + M − 1)/2, where F was the shortest latency of 16 consecutive F waves, M was the M-wave latency, and 1 was the delay time (in milliseconds) for antidromic activation of the alpha motor neuron. 7,29 CMCT was calculated as the difference between the cortical MEP latency and PMCT. 7,8
The primary outcome measure was MEP amplitude; the other outcome measures were MEP/Mmax, MEP threshold, and CMCT. Changes in variables at phases 1 and 2 from baseline in the acupuncture session were compared to the control session.
Statistical analysis
The Shapiro-Wilk test was used for all variables to assess normal distribution. Parametric data are expressed as mean (standard deviation), and nonparametric data are presented as the median and quartiles (first and third). When the data were normally distributed, two-way repeated-measures analysis of variance for two factors (session and phase) was used. When significant interactions were detected, post hoc Bonferroni tests were used for statistical comparison between baseline and phase 1, baseline and phase 2, and phase 1 and phase 2 in each session. Changes from baseline to phase 1 and phase 2 were compared between acupuncture and control session by paired t-test. When the data were not normally distributed, Friedman tests with the post hoc Bonferroni-corrected Wilcoxon tests (number of comparisons, 3) were used for intersession comparisons. Wilcoxon signed-rank tests were also used for comparison of changes in variables from baseline at phase 1 and phase 2 between acupuncture and control sessions. To test for period and carry-over effects, Mann-Whitney U tests were used on the differences and sums of the summary score for control and acupuncture sessions in terms of changes of MEP amplitude. p-Values less than 0.05 were considered to indicate statistical significance, except for the Bonferroni-corrected Wilcoxon test. For the Bonferroni-corrected Wilcoxon test, the significance level was set at p < 0.017 (0.05/3). These statistical analyses were performed with SPSS software for Windows (version 22.0; IBM, Armonk, NY).
The strength of the findings in terms of the differences in changes from baseline in variables between two sessions was determined by calculating the effect size r. 30 According to Cohen, 30 r = 0.10 is a small treatment effect, r ≥ 0.30 represents a medium effect, and r ≥ 0.50 is a large effect.
Results
There were no significant differences at baseline in MEP amplitude (p = 0.529), MEP/Mmax (p = 0.855), MEP threshold (p = 0.844), MEP latency (p = 0.289), PMCT (p = 0.725), or CMCT (p = 0.254) between acupuncture and control session.
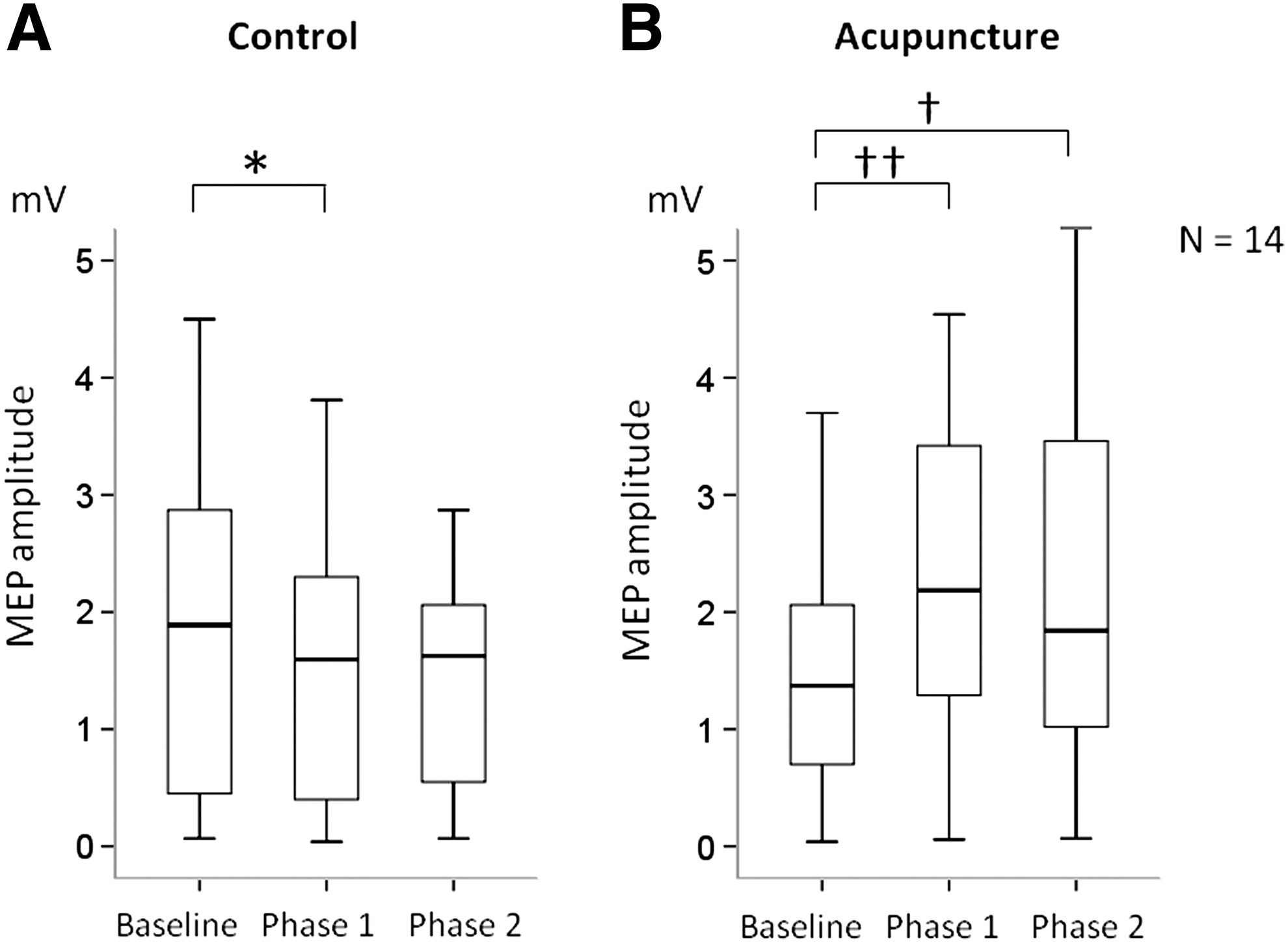
MEP amplitudes at each session are shown in Figure 3. Medians (first, third quartiles) of MEP amplitude in the acupuncture session were increased at phase 1 (2.19 [1.26, 3.56]) and phase 2 (1.84 [0.87, 3.50]) compared with baseline (1.37 [0.61, 2.20]), and the difference between phase 1 and baseline (p = 0.002) and phase 2 and baseline (p = 0.003) were statistically significant. In comparison, medians in the control session were reduced at phase 1 (1.60 [0.35, 2.30]) and phase 2 (1.63 [0.46, 2.11]) from baseline (1.89 [0.42, 2.87]), and the difference between phase 1 and baseline was statistically significant (p = 0.001). Changes form baseline to phases 1 and 2 are shown in Figure 4. Changes from baseline of MEP amplitude in the acupuncture session were significantly larger than those in the control session at phase 1 (0.52 [0.09, 1.79] versus −0.20 [−0.57, −0.03], p < 0.001, r = 0.437) and phase 2 (0.47 [0.03, 1.12] versus −0.16 [−0.69, 0.00], p < 0.001, r = 0.624). Nine patients received the acupuncture session first followed by the control session, whereas 5 patients received a control session, then acupuncture. There was no significant period effect (p = 0.541) or carryover effect (p = 0.606) in MEP amplitude.
Change in motor-evoked potentials (MEPs) in acupuncture and control session.

Changes from baseline in MEP amplitude at phase 1
The other variables in MEP and F wave measurements are shown in Table 2. MEP/Mmax in the acupuncture session was significantly increased at phase 1 (p = 0.002) and 2 (p = 0.001) compared to baseline, while those in the control session did not significantly change (p = 0.72, Friedman test). Changes from baseline of MEP/Mmax in the acupuncture session were significantly larger than those in the control session at phases 1 and 2 (p < 0.001, r = 0.623; p = 0.001, r = 0.576). Mmax amplitude did not show a statistically significant interaction between the treatment session and phase (p > 0.05).
Data are shown as mean (standard deviation) or median and quartiles (first and third).
p < 0.01 versus baseline.
p < 0.01 versus control.
p < 0.05 versus baseline.
p < 0.05 versus control.
MEP/Mmax, ratio of motor evoked potential amplitude and maximal M wave amplitude; MEP, motor evoked potential; Mmax, maximal M-wave amplitude; MSO, maximum stimulator output; PMCT, peripheral motor conduction time; CMCT, central motor conduction time.
MEP threshold in the control session was not changed significantly, whereas that in the acupuncture session was reduced, and there were significant interaction (p = 0.007) between treatment session and phase. Reductions in MEP threshold at phases 1 and 2 were significantly larger in the acupuncture versus control session (p = 0.031, r = 0.437; p = 0.023, r = 0.446).
CMCT was significantly reduced at phase 1 in the acupuncture session, although it was not changed significantly in the control session, and there was a significant interaction (p = 0.021) between treatment session and phase. Reductions of CMCT from baseline in the acupuncture session were larger than in the control session at both phases 1 and 2, and there was a significant difference only in phase 1 (p = 0.002, r = 0.552). The difference in CMCT change between both sessions at phase 2 was not significant (p = 0.135); however, it did present a medium-sized effect (r = 0.372). In the PMCT, no significant differences during either session were observed (p > 0.05).
There were no adverse events necessitating medical treatment in the present study.
Discussion
The current study evaluated the immediate effect of acupuncture at GV 26, Ex-HN 3, LI 4, and ST 36 on excitability of CST in patients with chronic DOC through use of TMS. This appears to be the first report to evaluate acupuncture effects on DOC patients following TBI by measuring MEP using TMS. MEP amplitude was increased and MEP threshold and latency were reduced during and after acupuncture. The amplitude and the latency of MEP using TMS may reflect not only supraspinal excitability but also the excitability of spinal neurons and the conduction along the peripheral motor pathway to the muscle. Therefore, MEP/Mmax amplitude and CMCT were calculated by the Mmax amplitude and PMCT using F-wave measurements, which reflect spinal motor neuron excitability and orthodromic stimulation of motor neurons that reach the muscle fiber. MEP/Mmax was significantly increased during and after acupuncture. CMCT exhibited a significant reduction during acupuncture and a tendency to be reduced after acupuncture, which was not statistically significant but represented a medium effect. Thus, the changes in MEP variables in the acupuncture sessions of the present study are thought to be due to changes in excitability of not spinal motor neurons but upper motor neurons. These findings indicate that CST excitability in patients with DOC following TBI is increased by acupuncture treatment, suggesting the possible mechanism of acupuncture treatment for these patients.
MEP variables are altered in patients with DOC and cerebral insult compared with healthy persons. 8 –12 Significant elevations in motor threshold levels in persistently unresponsive postcomatose patients with brain injury have also been reported. 9 Patient groups with VS and MCS exhibit lower MEP amplitudes and higher resting motor thresholds compared with healthy controls. 8
Acupuncture treatment and acupuncture point stimulation have been reported to alter excitability of the motor cortex. Treatment with electrical acupuncture point stimulation (EAS) with 2 Hz for 2 weeks was reported to improve the latency, CMCT, and amplitude more than did EAS with 100 Hz in patients with ischemic stroke. 25 In a study with stroke model rats, EAS at GV 26 tended to improve motor cortical excitability and facilitate motor function recovery. 31 In some case reports, acupuncture treatment has been shown to be a beneficial treatment for DOC. 13 –17 In the authors' clinical experiences, spontaneous movements of the finger and neck with pursuit were observed and increased in patients with DOC during and after acupuncture treatment, although clinical effects of acupuncture were not evaluated in the present study.
Given these findings, acupuncture treatment may promote the recovery of motor function in patients with DOC by activating CST. Acupuncture treatment might represent a viable therapy for patients with DOC and poor motor response following severe TBI. Further research is necessary to elucidate those clinical effects.
The mechanism of increasing CST excitability by acupuncture treatment and the specificity of acupuncture points that we used are not clear. It is generally well known that peripheral sensory stimulation induces short- and long-term changes in motor cortex excitability. Inhibition of motor cortex excitability by painful cutaneous 32 and muscle 33 stimuli has been reported. Conversely, a prolonged nonpainful stimulation of peripheral nerves induces a long-term increase in the excitability of the motor cortical representation of the corresponding hand muscles. 34 –36 Acupuncture and EAS have been reported to increase motor cortex excitability measured by TMS in healthy persons and stroke patients, 18 –20,25 similar to the results of the present study. The effect of acupuncture on the motor cortex was indicated to be a nonperipheral effect because acupuncture of the lower limbs affected MEP amplitudes recorded from upper limbs. 20 The inhibitory effect of acupuncture on motor system excitability has also been described. 21 Motor cortex inhibition was induced by acupuncture needle penetration at GB 34 on the lower leg in healthy persons. 21 Differences in points stimulated by acupuncture or condition of the brain (healthy or injured) might be associated with differential effects on motor systems evoked by acupuncture stimulation.
Acupuncture stimulation has been reported to alter cerebral blood flow and neuropeptide levels in the brain. 26,37 –40 EAS at GV 26 has been suggested to be able to activate noradrenergic neurotransmission in the brain, which in turn could reduce the central nervous depressive activity of anesthetics. 26 Acupuncture-like stimulation produces an increase in cortical cerebral blood flow via supraspinal reflex pathways, including intrinsic cholinergic changes in anesthetized rats. 37 Cortical inhibitory circuits have been suggested to be impaired in patients with DOC. 8 Intrinsic changes in neurotransmitter levels might be associated with increased motor cortex responsiveness by acupuncture in the current study. However, the effect of manual acupuncture on neuropeptides in the brain has been unclear because most acupuncture studies have used electrical stimulation with acupuncture. Moreover, the current study did not investigate changes in neuropeptide levels in the brain. In future studies, measurements of short intracortical inhibition, silent periods, and short latency afferent inhibition using TMS (which can evaluate the association between central cholinergic transmission and γ-aminobutyric acid interneurons) might be helpful for understanding mechanisms underlying acupuncture effects on the motor cortex.
Median MEP amplitude in control sessions was slightly but significantly reduced. The current study used interval times of 10 seconds in 10 consecutive TMSs because it was reported that TMS at 0.1 Hz did not change cortical excitability in healthy persons. 41 Although the reasons for reductions in MEP are not clear, the reduction in the control session might be due to habituation to consecutive TMS or differences between injured and healthy brains. Also, some of the patients were receiving medications that might contribute to changes in cortical excitability. 42 Moreover, not only central but also more peripheral effects might be related to these reductions in MEP amplitude because there was no significant change in MEP/Mmax and there was a trend for a reduced Mmax in the control session. Further studies with larger sample sizes under similar conditions of brain lesion need to be performed.
The current study includes some limitations regarding the interpretation of acupuncture effects because of small sample size, heterogeneity of TBI lesion, and an open-blinded design. Long-term and clinical effects and the specificity of the six acupuncture points used in this study are also unclear. However, the study demonstrated significant changes during and after acupuncture treatment on MEP using TMS. Further rigorous research with larger sample size, long-term observations, and clinical assessments, including motor function and a blinded randomized controlled design, should be conducted.
Conclusion
Acupuncture treatment increased CST excitability in patients with DOC following severe TBI. Acupuncture treatment might be a beneficial treatment by accelerating the pace of recovery of motor function in these patients.
Footnotes
Acknowledgments
The authors thank Mr. Norio Nishiyama for assistance with EMG examinations and all participants in this study.
Author Disclosure Statement
No competing financial interests exist.