
Abstract
Objective:
To examine the prevalence and modalities of complementary and alternative medicine (CAM) use in children with cancer and sickle cell disease; the reasons for use of CAM; and the use of CAM before, during, and after treatment in children with cancer.
Methods:
This single-center, observational study administered caregivers a written questionnaire regarding the use of CAM therapies.
Results:
A total of 101 caregivers completed questionnaires. Including prayer, total CAM use in oncology and sickle cell disease was 64% and 63%, respectively. Non-prayer CAM use was 30% in oncology and 23% in sickle cell disease. Of respondents who reported using any CAM, the three most commonly used types were prayer (62.3% oncology; 60.0% sickle cell disease), vitamins/minerals (14.8% oncology; 10.0% sickle cell disease), and massage (9.8% oncology; 7.5% sickle cell disease). The primary reasons for using CAM were to provide hope, to improve quality of life, and to lessen adverse effects. In oncology patients, CAM use tended to increase during treatment compared with before and after treatment.
Conclusions:
The reported prevalence of non-prayer CAM use was lower (23%–30%) in this sample than has been reported in national samples or other geographic regions of the United States. Nonetheless, participants reported many positive reasons for using CAM, including to gain hope, improve quality of life, and control pain. Thus, CAM use appears to be an important aspect of medical care for many pediatric hematology/oncology families and should be a consideration when providers are discussing treatment and quality of care with families.
Introduction
T
CAM is defined as “a group of diverse medical and health care interventions, practices, products, or disciplines that are not generally considered part of conventional medicine.” 16 However, no clear boundaries distinguish CAM from conventional medicine. 16 In a review based on 32 studies, mind-body interventions (i.e., hypnosis, distraction, and imagery) were the most common CAM therapies used to address pain, anxiety, and distress in children. 17 These CAM techniques were effective when used alone or in conjunction with pharmacologic therapies. 17
Although this growing body of pediatric CAM literature supports the overall efficacy of CAM in children, research indicates that CAM use varies by geographic region, ethnicity, and disease type. For instance, in Japan, the prevalence rate of CAM use in patients with cancer is 44.6%; the most common products are mushrooms, herbs, and shark cartilage. 18 In the United States, the most common CAM modalities used by adults with cancer are vitamins/minerals, prayer for self, and intercessory prayer. 19 Data from the National Health Interview Survey indicated that one in nine children throughout the United States used CAM in the previous 12 months. 20 However, there are ethnic differences in CAM use. Non-prayer CAM use among white children (12.8%) was reportedly two times greater than use among black children (5.9%). 20 Further, non-Hispanic children (12.8%) were about 1.5 times more likely to use CAM than Hispanic children (7.9%).
Estimates of CAM use among children with cancer vary widely, but most studies report that greater than 30% of children with cancer use CAM during the course of cancer treatment. 13,21,22 In 2003, 47% of pediatric oncology patients from Wake Forest University Baptist Medical Center used CAM after their diagnosis. 23 The most commonly used interventions were faith healing, megavitamins/minerals, massage, other dietary supplements, relaxation techniques, and herbal medicines/teas. In a systematic review of CAM use in pediatric hematology and oncology patients, the most commonly used therapies were herbal remedies, specialized diets and nutrition, and faith healing. 21 A commonly reported reason for CAM use is to relieve adverse effects from cancer treatment. 13,21,22
There is a lack of information on specific CAM use in patients with pediatric sickle cell disease. A study that surveyed 57 parents of children with sickle cell disease found that 54% of children used CAM. 24 Prayer, relaxation techniques, and spiritual healing were the three most commonly used interventions. Yoon and Black 25 suggest that CAM use in children with sickle cell disease may be as high as 70%. One study suggests that CAM use in patients with sickle cell disease may even increase in adulthood. 12 CAM is commonly used to treat or cure symptoms (80%), improve physical conditions (26%), and relieve symptoms of the illness (17%). 11 Little is known regarding pediatric use of CAM before and after cancer treatment. However, one recent study suggests that the majority of adults with breast cancer (66.7%) used CAM before their diagnosis and that 33% of patients became first-time CAM users after being diagnosed. 26
It was the primary aim of this study to examine specific CAM use in an ethnically diverse sample of children with cancer and sickle cell disease in Mississippi. Specifically, the study examined (1) the prevalence and modalities of CAM use in children with cancer and sickle cell disease; (2) reasons for use of CAM in this population; and (3) use of CAM before, during, and after treatment in children with cancer. Consistent with the broader literature, we hypothesized that children with oncology conditions would use CAM at a higher rate than children with sickle cell disease and that non-minority children would use CAM at a higher than minority children.
Materials and Methods
This single-center, observational study administered a single written survey during a regular outpatient hematology/oncology clinic visit. All survey data were collected between May 2009 and February 2012. The institutional review board of the University of Mississippi Medical Center approved the study, and each participant provided informed consent. The University of Mississippi Medical Center is the only children's hospital and hematology/oncology specialty clinic in the state. Eligible participants were identified by medical staff by daily chart review. Inclusion criteria consisted of being a primary caregiver of a child age 3–18 years diagnosed with cancer or sickle cell disease. The age criterion of 3 years of age or older was deemed necessary (e.g., Mungas et al. 27 ) for the assessment of children engaging in prayer. Participants were excluded if the caregiver was non–English speaking or had developmental delays or cognitive impairment. Eligible families were approached in an exam room by a research assistant. Participants then completed the author-generated Demographic Questionnaire, CAM Use Questionnaire, and Specific Therapies Questionnaire. A maximum of one caregiver per family participated. All questionnaires were completed by using a pencil and paper format and took approximately 25–35 minutes to complete. Participation was voluntary and participants were not compensated for their time.
Demographic Questionnaire
Parents completed a brief demographics questionnaire that assessed caregiver race, level of education, family income level, caregiver marital status, child age, child diagnosis, conventional treatment received for diagnosis (e.g., surgery, chemotherapy, long-term transfusion, pain medication), and disease being treated (e.g., leukemia/lymphoma, brain tumor, bone cancer, other cancer, sickle cell disease). Diagnoses were confirmed with medical chart review.
CAM Use Questionnaire
Items were multiple choice and included (1) whether parents have heard of CAM, (2) whether parents have used CAM personally, (3) whether their child has used CAM, (4) reasons for using/not using CAM, (5) perceived benefits/risks of CAM, (6) cost of CAM used, and (7) with whom they have discussed CAM use (e.g., primary care physician, oncologist, hematologist, friend, family). Items asked if CAM was used, in either the past or present, to treat the child's disease.
Specific Therapies Questionnaire
Parents reported on 23 different types of CAM. Items asked whether parents had (1) heard of a specific CAM therapy (e.g., vegan diet, meditation, yoga, massage), (2) whether their child has used that CAM therapy to treat his/her cancer or sickle cell disease, and (3) when their child used that therapy (i.e., before, during, or after therapy). Use of specific therapy items were scored as 0 = no and 1 = yes.
Statistical analysis
Demographic characteristics and descriptive statistics for the sample were computed in the SPSS software, version 22.0 (IBM, Armonk, NY). Seventeen caregivers (17%) did not complete the full survey, while all other data were randomly missing. Pairwise deletion with available data was used throughout analyses to minimize biases due to random missing data (1% to 66%). Group differences were examined by using independent sample t-tests for continuous data and chi-square test for categorical data. The relationship between parent self-use of CAM and child use of CAM was examined with zero-order correlations. CAM use percentages were calculated as the number of participants who reported using that therapy divided by the total number of oncology or hematology patients. Participants who did not respond were counted as not having used the CAM therapy. To examine change in CAM use over time, repeated-measures analysis of variance (ANOVA) with Greenhouse-Geisser correction was used to assess differences in the number of oncology participants who used CAM therapies before, during, and after treatment. A repeated-measures ANOVA was also used to assess differences in the total number of CAM therapies used before, during, and after oncology treatment. Given that sickle cell disease is a chronic genetic condition, with no off-set of therapy, this analysis was conducted only for oncology patients.
Results
A total of 101 caregivers completed the author-generated surveys (61 caregivers of oncology patients and 40 caregivers of patients with sickle cell disease). Patient demographics are presented in Table 1. Only 10% (n = 10) of caregivers reported that they had personally used CAM. Child CAM use significantly correlated with parents' use of CAM (r = 0.69; p < 0.001). Of those who used CAM, most (90%) spent less than $100 on CAM total. A total of 64% caregivers of oncology patients and 63% of sickle cell disease patients reported using at least one CAM therapy, including prayer. Non-prayer CAM use in oncology and sickle cell disease was 30% and 23%, respectively. White children had a lower prevalence of non-prayer CAM use (22%) than minority children (29%; p < 0.01). There was no significant difference in CAM use between male children (22%) and female children (13%; chi-square = 1.12; p = 0.29).
GED, General Education Development.
CAM use
The frequency of CAM use is presented in Table 2. Of those who reported using any CAM, the three most common types used were prayer (62.3% oncology; 60.0% sickle cell disease), vitamins/minerals (14.8% oncology; 10.0% sickle cell disease), and massage (9.8% oncology; 7.5% sickle cell disease). However, prayer, vitamins/minerals, and herbal therapy, respectively, were the three therapies most commonly heard of. The use of different categories of CAM (i.e., mind-body practices and natural products) was not significantly related to patient diagnosis.
Of those who used CAM, 75% (n = 9) and 40% (n = 2) of oncology and sickle cell disease patients, respectively, reported that it was “very helpful.” Table 3 describes the extent to which patients viewed CAM to be helpful. Only one oncology patient (8.3%) reported that CAM was “harmful.” The main reasons for using CAM was to provide hope (50% oncology; 25% sickle cell disease), to improve quality of life (0% oncology; 50% sickle cell disease), and to lessen adverse effects (33.3% oncology; 0% sickle cell disease). Chi-square analyses revealed that patients' perception of CAM was not significantly related to diagnosis.
There was a low response rate for this section of the survey; please see discussion of limitations in text.
CAM, complementary and alternative medicine.
Knowledge and discussion of CAM
Interestingly, 50% of caregivers of oncology and sickle cell disease patients reported that they had not previously heard about CAM (Table 4). Of those who had heard of CAM, 17.2% of caregivers of oncology patients and 40% of sickle cell disease patients reported first hearing about CAM from a medical provider. The remaining caregivers reported first hearing about CAM from other sources (i.e., a family member, the Internet, another parent, or other).
Not enough responses to conduct chi-square analyses.
Fifty percent of caregivers of oncology patients reported not discussing CAM use with anyone, while 66.7% of caregivers of children with sickle cell disease reported discussing CAM use with a nonmedical person. A majority of caregivers of oncology patients reported not discussing CAM with their oncology doctor/nurse because their provider did not ask (55.6%), and others reported that they did not feel it was important for the provider (44.4%). Caregivers of sickle cell patients also did not discuss CAM with their hematology doctor/nurse primarily because they did not feel it was important for the provider (40%). While 55.8% of caregivers of oncology patients reported that they would not like to discuss CAM with their oncology provider, 71.1% of sickle cell caregivers reported that they would.
CAM use during oncology treatment
Among oncology patients, the number who used CAM therapies did not change over time. As shown in Figure 1, a total of 37 oncology patients (out of 61 [60.7%]) were reported to use CAM before, during, and after treatment. The total number of CAM therapies increased from 88 before oncology treatment to 101 during oncology treatment and then declined to 74 after oncology treatment. Specifically, caregivers of patients reported using more CAM therapies during treatment (mean ± standard deviation, 1.66 ± 1.83 CAM therapies) than before oncology treatment (1.44 ± 1.78); however, this difference was not significant (F = 1.73; p = 0.19). The number of CAM therapies used after oncology treatment (1.21 ± 1.69) significantly decreased compared with during oncology treatment (F = 6.46; p = 0.01) and was similar to before-treatment levels of CAM use (F = 1.95; p = 0.17). CAM use before, during, and after treatment was not examined in patients with sickle cell disease because sickle cell disease is a chronic genetic condition with no off-set of therapy.
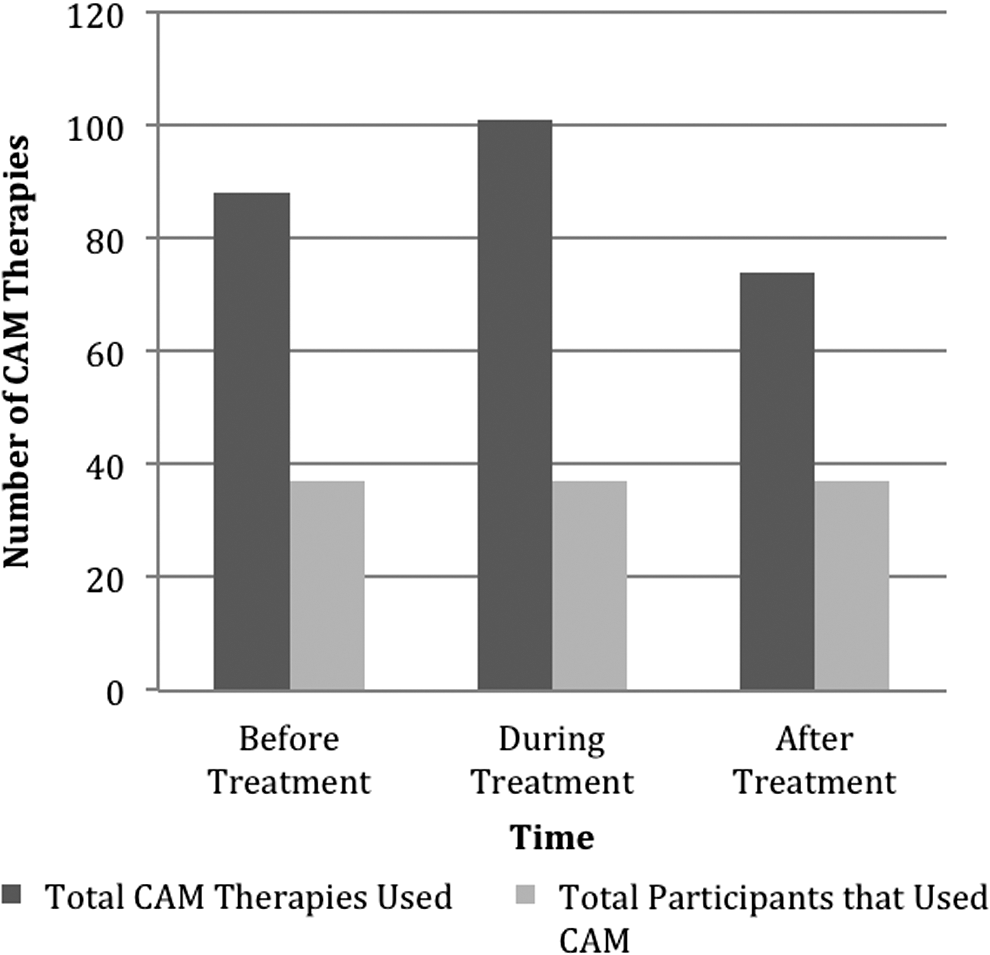
Caregivers' report of complementary and alternative medicine (CAM) therapies used by treatment phase for oncology patients.
Discussion
CAM is a constantly evolving field with varied modalities and varied geographic use among pediatric hematology/oncology patients. CAM use is increasing in pediatric populations, and thus it is important to examine the use of specific CAM modalities in pediatric hematology/oncology populations across different geographic regions and racial/ethnic groups in the United States. In this study, prayer was the most commonly reported CAM modality used for both cancer (59.0%) and sickle cell disease (56.3%) patients. Excluding prayer, this study found a 23%–30% estimated prevalence of CAM use in this sample, which is lower than what has been reported in other areas of the United States. 13 –15,22 –25 This low prevalence of non-prayer CAM use may have been due to fewer financial resources, limited accessibility, and lack of insurance coverage for CAM modalities in our population. The low prevalence also did not allow the study to have adequate power to provide statistically significant differences in demographic characteristics between sickle cell and oncology patients. The sickle cell population was lower income and from single-mother households, while other demographic characteristics were not significantly different.
Most (95.6%) of participants who did not use CAM reported that they did not use it because of the lack of information. This may indicate a lack of dissemination of information from clinical studies or lack of education. A majority of participants (56%) expressed interest in talking about CAM with their medical provider; however, only 21% had actually done so. The two most commonly reported motivations for CAM use were hope and improved quality of life. Other reasons why caregivers chose to use CAM for their child included cure, alleviation of pain, control of cancer, assistance with other therapies, and boosting of immunity. This study confirms previous findings that the reason individuals use CAM are varied and personalized to their condition and stage of disease. For those who used CAM, the majority felt it was helpful; however, 5% did report that it was harmful. More participants discussed their use of CAM with non-medical providers rather than with medical providers. Interestingly, of those who discussed CAM with their providers, none of them were told to discontinue use, although 5% of participants were concerned that they would be told to discontinue CAM use. Although participants felt that CAM might provide hope, improved quality of life, and possible cure, 32% did not feel it was important to discuss their CAM use with their medical provider.
In evaluating the timing of use, there are many missing data points possibly secondary to survey fatigue, which does not allow performance of a statistical analysis. However, the remaining data indicate an overall trend toward and increased use of CAM during therapy and a slight decrease to just below baseline after treatment completion.
Limitations of this study include a small sample size for the cancer and sickle cell disease groups and decreased power to detect group differences due to a low response rate on several items. Survey fatigue may have developed secondary to the large amount of specific therapies listed. Participants did not list therapies that were not shown, so either the questionnaire list was inclusive of all modalities being used in this sample, or participants were unwilling to write in specific modalities. Additionally, some participants may have also misunderstood certain items, as with more participants endorsing use of macrobiotics compared to the number of participants who had heard of macrobiotics. Other study limitations include the cross-sectional, single-site design, parent-only report of parent and child use of CAM, and the exclusion of non–English-speaking caregivers. Future studies would benefit from prospectively examining CAM use throughout the course of treatment and follow-up in hematology/oncology populations, as well as the use of multiple informants and standardized measures for better comparison across geographic regions. Prospective studies may obtain a more ethnically diverse sample by making the necessary accommodations to include non–English speakers in their research.
In conclusion, this study found a very high rate of use of prayer reported by parents in this pediatric hematology/oncology sample. Excluding prayer, there was a lower reported prevalence of CAM use (23%–30%) in this sample than has been reported in national samples or geographic regions of the United States. There was no significant difference in reported CAM use between parents of children with cancer or sickle cell disease. While the majority of participants expressed interest in talking about CAM with their medical provider, only a small proportion of participants had actually done so. Participants reported many positive reasons for using CAM, including to gain hope, improve quality of life, control pain, and help with other aspects of their disease. Although the prevalence of CAM use in Mississippi is relatively low, CAM use appears to be an important aspect of medical care for many pediatric hematology/oncology families and should be a consideration when providers are discussing treatment and quality of care with families.
Footnotes
Acknowledgments
The authors thank the families at the University of Mississippi Medical Center Children's Cancer Center and Sickle Cell Clinic for their participation in this project.
Author Disclosure Statement
No competing financial relationships exist.