
Abstract
Objective:
Acupuncture has been shown to treat various medical conditions, including acute and chronic pain, and there is limited evidence that acupuncture produces anti-inflammatory effects. This pilot study evaluated the use of acupuncture to treat pain and determine if acupuncture can reduce the inflammatory response in pediatric patients diagnosed with acute appendicitis.
Design:
This pilot study used convenience sampling and was conducted in the Pediatric Emergency Department (PED) of an urban tertiary care children's hospital. Patients conventionally evaluated and definitively diagnosed with appendicitis were eligible to voluntarily participate.
Intervention:
The diagnostic homogeneity of the target population allowed for a standardized intervention protocol. A licensed acupuncturist performed a specific form of Japanese acupuncture known as the Kiiko Matsumoto Style on all study patients.
Outcome measures:
Subjective pain was assessed immediately before the intervention and 20 minutes postintervention, using 3 measures: Faces Pain Scale-Revised (FPS-R), colored analog scale (CAS), and visual analog scale (VAS). Evidence of inflammation was assessed using two biomarkers: white blood cell (WBC) count and C-reactive protein (CRP). WBC and CRP were drawn and recorded 3 times: before the intervention, 2 minutes before removal of needles, and 30 minutes after needling.
Results:
Six Latino/Hispanic patients (4 males, 2 females, median age=15 years) with no previous acupuncture experience participated in the study. Median pre/postacupuncture pain scores were as follows: FPS-R, 5 vs. 4; CAS, 6.1 vs. 4.8; VAS, 46 vs. 32. Median WBC (103/μL) and CRP (mg/dL) across time were as follows: WBC, 13.2, 11.8, and 11.4; CRP, 4.5, 4.9, and 5.1. Median acupuncture duration was 28.5 minutes (range 22–32) and no complications were observed.
Conclusions:
Pilot data suggest that acupuncture may be a feasible and effective treatment modality for decreasing subjective pain and inflammation as measured by WBC. Acupuncture may be a useful nonpharmacological PED intervention for treating patients with acute appendicitis pain.
Introduction
T
In a descriptive study regarding patients with an “acute abdomen,” investigators explained the utility of acupuncture therapy, suggesting that it addresses pain through the vegetative nervous system. 2 Similarly, a review article surmised that the anti-inflammatory actions of acupuncture are thought to be mediated via “their reflexive central inhibition of the innate immune system.” Specifically, there is evidence that acupuncture has an effect on a variety of inflammatory substances, including TNF, IL-1 beta, IL-6, IL-18, and other postinflammatory cytokines. 3
Based on the background literature, the current pilot study attempted to demonstrate that acupuncture is an effective pain-relieving modality for Pediatric Emergency Department (PED) patients who have acute appendicitis. We further sought to show that acupuncture reduces the levels of inflammatory serum biomarkers over time.
Materials and Methods
Standard of care
Evaluation for appendicitis in the PED involves a history and physical examination and laboratory studies, which includes white blood cell (WBC) count and C-reactive protein (CRP) level. Some patients are diagnosed clinically by pediatric surgeons, while others receive an ultrasound or CT scan (abdomen/pelvis) to definitively diagnose appendicitis. Patients requiring pain relief are typically given morphine.
Research procedures
The study was approved by the Institutional Review Board at the treating hospital, which is an urban, tertiary care children's hospital with an annual PED census of approximately 70,000 patients. Patients definitively diagnosed with appendicitis were eligible for study participation. Given the pilot nature of this study and its emphasis on demonstrating the effectiveness of acupuncture, convenience sampling was used to generate a single treatment group, which thereby precluded a control group undergoing sham acupuncture. 4 Informed assent and consent were obtained if patients and parents agreed to participate after meeting with the study's licensed acupuncturist and a research investigator. The acupuncturist, employed at a pain clinic within the hospital, volunteered time each month during the study period to treat all PED patients and families who agreed to participate in this pilot research. Patients who declined study participation were offered pain treatment by standard means (e.g., morphine).
Kiiko Matsumoto Style (KMS), a type of Japanese acupuncture, 5 was used in the study. The diagnostic homogeneity of the target population allowed for a standardized intervention protocol. In KMS, identifying active reflexes guides the selection of treatment points. This is done by a systematic palpation of the abdomen, acupuncture channels, and points—revealing specific patterns that are associated with the patient's presenting symptoms. A successful treatment in KMS acupuncture reduces the discomfort found in these diagnostic areas and, as a result, reduces the patient's presenting symptoms. Most cases of acute appendicitis fit the pattern identified as “spleen and immunity deficiency,” and commonly present with the following reflexes: right side St-26 and St-27 area; one side or bilateral Tw-16 area; and left subcostal region. These reflexes can be treated with a combination of two or more of the following points listed in the order of most effective first: “Master Nagano's immune points” located on the radial side of the forearm about 5 cm below the elbow: Ki-6; Sp-5; Sp-9; Tw-16; St-40; Ki-16; and Ren-6.
The number of points selected depends on the changes observed in the active reflexes, with most of the cases only requiring the bilateral needling of the first 4 points, listed above, to release the pain present on these reflexes. The KMS needle insertion depth varies from 5 to 15 mm depending on the size of the patient. Needles used in the study were sterile, single-use (disposable) Seirin 40-gauge (0.16 mm wide) and Seirin 30 mm solid and flexible, nonbreakable needles with hollow canals.
The study procedures are presented in Figure 1. Pain was assessed subjectively using the Faces Pain Scale-Revised (FPS-R), 6 colored analog scale (CAS), 7 and visual analog scale (VAS), 8 and objectively using WBC and CRP. All data were examined using summary statistics.
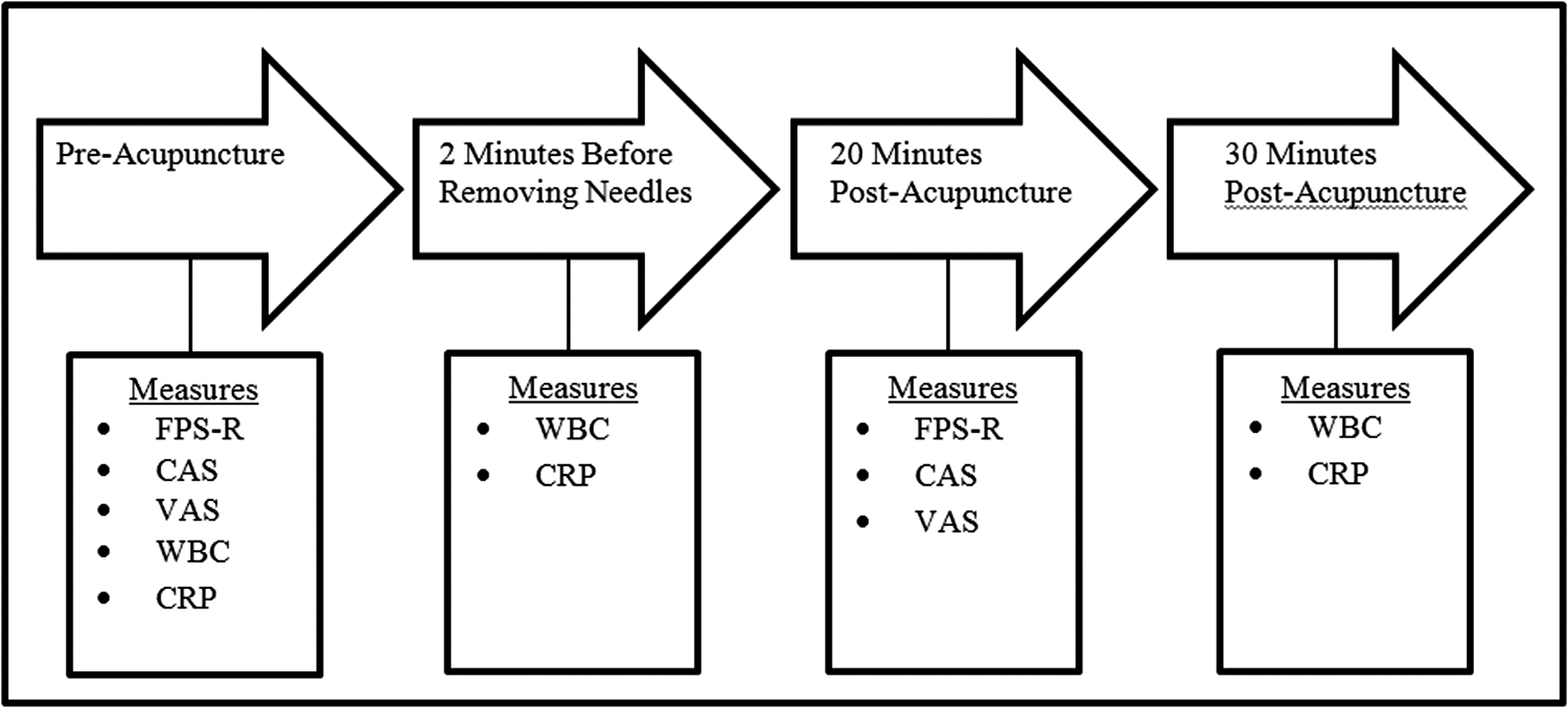
Study procedures. CAS, colored analog scale; CRP, C-reactive protein; FPS-R, Faces Pain Scale-Revised; VAS, visual analog scale; WBC, white blood cell.
Results
Study patients consisted of 4 males and 2 females of Latino/Hispanic background with no previous acupuncture experience. This study sample was achieved during a period of 7 months, during which 8 other patients (5 males and 3 females) and their families were approached but declined to participate in the study. Of these refusals, 3 families preferred pain treatment by standard means (e.g., morphine), 2 patients reported that they had almost no pain to address, and 2 patients reported fear of needles.
Median age of the study sample was 15 years (range 10–17). Median needling duration was 28.5 minutes (range 22–32) with no complications observed. Pre/postacupuncture median pain scores and median WBC (103/μL) and CRP (mg/dL) are presented in Figure 2.

Median pain scores and inflammation values.
Discussion
Acupuncture has been shown to treat various acute and chronic medical conditions. In addition, there is limited research reflecting acupuncture's anti-inflammatory effects. Because narcotics have numerous known side effects, including respiratory depression, nausea, dizziness, vomiting, constipation, and arrhythmias, we sought to find a viable alternative. The current pilot data support the concept that acute acupuncture in the PED can affect subjective pain scores and produce reductions in serum biomarkers, that is, inflammatory response.
PED acupuncture is novel, as there is no prior published work in the same setting. Acceptance of acupuncture and other CAM therapies has, however, been documented in the literature. A survey was undertaken in a PED, asking families to determine whether they were interested in or had used CAM therapies. A review of 525 surveys identified that 63 (12%) of caretakers had acknowledged that they had used a CAM therapy to treat their children's symptoms or illness. 9 In a similar study, 602 parents/caregivers of children 0–18 years who presented to an urban PED were surveyed. The overall use of CAM among children was 15%, especially among children older than 5 years. 10
Pediatric pain management was examined in a clinical trial by Wu et al., 11 who described the acceptability and feasibility of acupuncture for acute postoperative pain control in hospitalized children. A total of 20 patients, 7 months to 18 years old, underwent 10–15-minute sessions of acupuncture 24–48 hours apart. The treatment was highly successful, tolerated well, and did not produce adverse events. Seventy percent (70%) of parents said that they would pay for acupuncture even if it was not covered by insurance. The authors concluded that acupuncture is a highly accepted modality in critically ill postoperative pediatric patients with acute pain. Similar to the effectiveness in the aforementioned study, our pilot study demonstrated that acupuncture may be a useful adjunct for acute pediatric pain management in PED patients with acute appendicitis.
Regarding pain scoring strategies, changes in subjective pain intensity scores of ≥1 point on the FPS-R and CAS and ≥10 points on the VAS are considered clinically significant. Our patients reported a moderate level of subjective pain, but on all scoring schemes, their reported pain decreased. These changes suggest that patients' subjective pain decreased because of the acupuncture treatment.
Considering the possible biological basis of acupuncture, we examined inflammation using serum biomarkers. Specifically, we measured WBC and CRP before acupuncture treatment, before removing the needles, and after the end of the treatment. Although CRP as a general marker of inflammation stayed roughly the same on sequential blood draws, the median WBC showed a modest and noticeable drop. The implication of this finding is that the effectiveness of acupuncture may have a biophysiological basis.
Limitations
Since our research was a pilot study with a small sample size that precluded statistical analysis, the data may still be open for interpretation, especially the data from the biomarkers. As with all studies involving acupuncture, pediatric patients of varying ages may subjectively interpret the treatment differently from one another. They may report psychological effects, especially if acupuncture is a new experience for them. Furthermore, we acknowledge that our study patients' subjective pain ratings may have been affected by the environment of a busy PED, associated with their parents' anxiety, or influenced by unfamiliarity with the treating physicians, nurses, study investigators, and/or acupuncturist. In addition, the results from this study reflect effects of acupuncture in a very specific group. All of the participants in our study presented with the same active reflexes, and therefore the selection of the same treatment points was possible. In a less homogenous population, however, the palpated findings may significantly vary between patients, and consequently a standardized protocol of acupuncture treatment points would not be possible. This is a significant limitation of many acupuncture studies that prioritize a standardized protocol of treatment points versus an individualized treatment approach.
Future directions
This study was a first attempt to demonstrate that acupuncture can be effective for patients suffering from pain associated with appendicitis and to show that there may be a biological basis regarding acupuncture's effectiveness. Our hope in the future is to conduct a large randomized controlled trial in the PED, whereby patients would receive KMS acupuncture treatment, sham acupuncture, or morphine for pain relief. This design would allow us to more rigorously investigate serum biomarkers and the overall utility of PED acupuncture.
Conclusions
The pilot data from this study suggest that acupuncture may be a feasible and effective treatment modality for decreasing inflammation as measured by WBC and decreasing subjective pain. Acupuncture may be a useful nonpharmacological Emergency Department intervention for treating patients with acute appendicitis pain.
Footnotes
Author Disclosure Statement
No competing financial interests exist.