
Abstract
Objective:
To examine the effects of laughter therapy on secretory IgA (sIgA) in postpartum women.
Methods:
The study used a nonequivalent control group with nonsynchronized design. The participants were 76 postpartum women who agreed to participate in this study and were selected by convenience sampling (experimental group, n = 38; control group, n = 38). The data were collected from December 15, 2009, to April 8, 2010. The experimental group participated in a postpartum laughter program from a laughter therapy expert for 60 minutes per session, twice a week for 2 weeks, for a total of four sessions. To evaluate the effects of the postpartum laughter program, sIgA levels in breast milk were measured. The data were analyzed using SPSS WIN 20.0 software.
Results:
Immune response (sIgA) significantly differed between the experimental and control groups.
Conclusion:
A postpartum laughter program can be applied as a complementary and alternative intervention to postpartum women in a transitional mother-infant care center.
Introduction
T
Korea has a tradition wherein the postpartum period is considered a family responsibility rather than a personal duty. Members of the family provide support, and a Korean woman who has given birth is familiar with a type of care called Sanhujori, which is provided for about 3 weeks. Because traditional postpartum care in the home has been difficult as a result of modern changes to the social structure, transitional mother-infant care centers (also known as Sanhujoriwon facilities) have emerged. 2
A transitional mother-infant care center operates postpartum care businesses, and the numbers have increased consistently along with social conditions since the first establishment in October 1996. The facility generally provides feeding, convalescence, and other conveniences for daily lives of women who have just given birth. Care can last as long as 2 months for both mothers and infants under 2 months, but most women stay for 1 to 3 weeks after being discharged from the hospital. 3 Aromatherapy sitz bath, 4 aroma therapy, 5 social support, 6 and doula intervention 7 have been reported in previous studies as complementary and alternative interventions for helping women postpartum, but the development of effective interventions that have verifiable research results and can help postpartum women is needed, as well as more accessible, self-controlled, and easily applicable interventions during puerperium.
Laughter therapy makes the human body and mind healthy. It draws on humans' internal self-healing and self-recovery abilities from the body, 8 and it is beneficial physiologically, psychosocially, and mentally for a variety of people, such as patients with cancer, 9 –12 patients with diabetes, 13 postpartum women, 14 elderly persons, 15 –17 soldiers, 18 and nursing students. 19 It affects the circulatory system, respiratory system, and immune system; can change or alleviate pain, blood glucose levels, and stress reaction; reduce anxiety 20 and depression; 21 alleviate stress; 22 and improve self-esteem. 23 Such effects have made laughter therapy so popular that various studies have applied this therapy to nursing in Korea.
Many of the previous studies on laughter therapies and immune responses 24 –26 have reported that the therapies increase activities of natural killer (NK) cells and revitalize immune factors (IgA, IgG, and IgM). Cho and Oh 11 reported on breast cancer survivors and showed that laughter therapy had no effects on NK cells or T cells. Sustainable and repeatable research is needed to verify these results because the reported effects of the therapy were different from the published research.
In this study, the postpartum women who stayed in a Sanhujori facility for 1–3 weeks were selected to participate in a laughter program developed for this study. To verify effects of the program, effects on the immune responses via secretory IgA (sIgA) in breast milk were measured (all the women in the study were breast-feeding during the postpartum period).
Based on theoretical grounds and the effectiveness of laughter therapy described in previous studies, this study sought to provide empirical evidence for use of this therapy as a nursing intervention for postpartum women by verifying the effects of laughter therapy on immune responses.
The study hypothesis of this study was as follows: Compared with women in the control group, women in the experimental group (i.e., those participating in laughter therapy) will show little decrease in breast milk sIgA.
Materials and Methods
Design
This study used a quasi-experimental design with nonequivalent control groups to examine the effects of laughter therapy on immune responses in postpartum women.
Participants
The participants were women who gave birth at a women's hospital in Gyeonggi Province, Korea, and were admitted to the affiliated Sanhujoriwon facility after delivery (third day for vaginal deliveries, fifth day for cesarean deliveries). Each participant provided written consent in advance.
The criteria for selecting the participants were as follows: (1) women who gave birth between the 37th and 41st weeks of gestation, (2) postpartum women age 20–40 years, (3) women who delivered a healthy infant, (4) breast-feeding mother, (5) women who showed no complications during labor and puerperium, (6) women who have not previously been exposed to laughter therapy, and (7) women who understood the purpose of this study and agreed to participate with written consent.
Because the medical environment of health personnel and medical practice could affect the dependent variables, only the women admitted to the same Sanhujoriwon facility were selected. Health problems of the infant or a premature baby may also be an exogenous variable that affects the level of immune responses; thus, they were excluded from the selection. In addition, women who had previously participated in laughter therapy were excluded from the selection because the effects of the intervention could not be measured precisely.
On the basis of the statistical program G. Power 3.0, with conditions set as medium-sized effects of 0.5, significance level of 0.05, and statistical power of 0.8, the number of participants in each of the two groups was calculated as 16, totaling 32 participants. Considering that there might be dropouts, the researchers selected 49 participants for the experimental group and 45 for the control group. Eleven participants from the experimental group were eliminated (6 because of early discharges and 5 dropouts for private reasons), along with 7 from the control group (1 for the lack of breast milk, 4 for incomplete surveys, and 2 for not collecting breast milk samples), so the final number of the participants was 76 (n = 38 for each group).
Research instruments
Immunoglobulin is a protein related to immunity. It belongs to globulin among antibodies, and breast milk immunoglobulin is sIgA in milk. 27 Breast milk immunoglobulin in this study was measured as the value of sIgA content within milk of an early postpartum woman who was breast-feeding.
Because the participants were women who had given birth recently, immune responses were checked for changes in the amount of sIgA secreted in breast milk. Changes in the density of immunoglobulin were analyzed by using an enzyme-linked immunosorbent assay kit (Immundiagnostik, Bensheim, Germany). For the analysis, 3 mL of breast milk was collected from both the experimental group and the control group between 10:00 a.m. and 12:00 noon, before the experiment was conducted, and at 6:00 to 7:00 p.m., shortly after the end of the postpartum laughter program. Each breast milk sample was put in a sterilized tube, and the sample tubes were preserved at −20°C in a freezer. Then, each frozen breast milk sample was moved to a −70°C freezer 1 week after being preserved. The collected breast milk was put in a 5-mL sterilized tube, and the tube was preserved in a −70°C freezer. Before analysis, the frozen breast milk was melted at room temperature; then, the melted breast milk was analyzed by using the enzyme immunoassay kit (Assay Designs, Inc., Ann Arbor, MI). Clinical specimen analysis was conducted after collection of all data from both groups. To prevent measurement errors, the entire clinical specimen was analyzed by the same person in the clinical laboratory of K University Hospital. sIgA was the most dense immunoglobulin in breast milk, and it is distinguished depending on the secretion time of breast milk after childbirth; the highest density is seen right after delivery. The density gradually decreases as time goes by; therefore, there are different opinions among researchers. 28,29 In this study, the average density of breast milk sIgA collected on the third day after vaginal delivery (sixth day after a caesarean delivery) at the time the pretest started was 778.82 mg/dL, and the one collected on the 16th day after vaginal delivery (19th day after a caesarean delivery) at the time of post-test was 350.11 mg/dL.
Data collection
Data were collected through a preliminary investigation and the main collection. Figure 1 illustrates the procedure in detail.

Postpartum laughter program.
Preliminary investigation
The postpartum laughter program was verified by two professors of nursing science and three laughter therapy experts (one from the Korea Laughter Institute and two from the Korea Laughter Clinic Academy) to develop a proper protocol for puerperal woman and in order to use the program as an item of care for mothers in the affiliated Sanhujoriwon facility of the women's clinic.
For the program, a pre-investigation was conducted with 13 women who had given birth and were entering the Sanhujoriwon, where the main investigation was to be conducted. The contents of the program were modified and supplemented so that the women could easily follow it and the Sanhujoriwon could use it as an actual postpartum education program.
Main investigation
Data were collected from December 15, 2009, to April 8, 2010. To avoid a diffusion effect of the experiment, the data for the control group were collected from December 15, 2009, to January 30, 2010, and for the experimental group from February 5 to April 8, 2010.
With cooperation of the nursing department, the purpose of the study, the study process, and the data collection procedure were explained to three chief nurses from three wards for the pretest, as well as to the Sanhujoriwon management director and two nurses for post-test data collection.
In addition, the experimental medical treatment was assisted by a laughter therapy expert and the researcher, and data collection for the survey and breast milk sampling were conducted by six research assistants. This was done to maintain a distinction between those who gave the experimental medical treatment and those who collected the data.
The pretest was conducted by individually contacting participants who had delivered and were hospitalized in the maternity ward of the target hospital and who understood the standards of selection criterion. Pretests for the experimental group and the control group were conducted from 10:00 a.m. to 12:00 noon on the day of discharge after delivery (third day for vaginal delivery, sixth day for caesarean delivery) on tests for immune responses in the maternity ward. Breast milk sIgA was collected directly from the woman with a 3-mL sample of her breast milk expressed with her own hands.
Following the report of Ryu and Lee, 30 a laughter program twice a week is more effective than once a week in terms of having effects on the changing body and mind. The researchers provided a program that consisted of 60-minute sessions held twice a week (Monday and Thursday), for a total of four sessions over 2 weeks according to the average time periods of women staying in the Sanhujoriwon facilities. Also following the report of Gardner et al. 31 that laughter is easier to provoke in a group than with an individual, the researchers organized the program into three stages (introduction, enhancement, wrap-up) for the groups of women (Fig. 1).
The first stage was an introduction to establish mood and intimacy, self-introductions, friendship, healthy clapping, and various ways of greetings and stretching facial muscles for 10–15 minutes.
The second stage of enhancement included laughter dance routines, healthy laughter, and applause with laughter, all with the goal of reducing stress, inducing positive thinking, and enhancing self-esteem. Each session lasted 30–35 minutes, with two or three different kinds of healthy laughter being provided to prevent boredom among the participants. These different types of laughter included lymph laughter (laughing while tapping and shaking both sides of the axillae as if the laughter were massaging the immune system), laughing while massaging the breasts clockwise, brushing-teeth laughter, muscle-stretching laughter, laughter shower, laughter gun, laughter dance routine, and laughter bomb.
In the third stage as a wrap-up, the program provided relaxation with quiet music and poetry reading and an opportunity for the participants to interact with each other by expressing their feelings on the changes in their body and mind after the program. Each session ended with stretching muscles and massages, greetings with a hug, greetings with a thankful mind, and positive conversations with the others. This wrap-up session lasted 10–15 minutes.
Because sustainability is more important than one-time laughter therapy, 15 the participants were given laughter assignments at the end of every program. This allowed them to repeat the laughter training in order to maintain the sustainability; specifically, immune laughter with massaging their own breasts clockwise was recommended.
For the experimental group, data from the immune responses test, 3 mL of breast milk was sampled by each woman in the same manner as for the pretest. The same data were collected from the control group. To satisfy ethical responsibility, the postpartum laughter program was introduced to the women in the control group through handouts after the data collection was completed. After the study was finished, a CD on infant massage was provided to all group members as an incentive.
Ethical considerations
Before the study began, it was approved by the university's ethics committee to verify contents of the study (IRB-2009-53). Before data collection, participants who met the inclusion criteria and agreed to participate were identified. Second, voluntarily written consent from the participants was received, followed by an explanation of the instructions orally and in writing, including the purpose and methods of the study, the guarantee of anonymity throughout the study participation, voluntary agreement and disagreement of study participation, assurance that any participant could quit at any time, and possible benefits and disadvantages. It was also explained that the clinical specimen sampled from breast milk would only be used for the breast milk test.
Statistical analysis
Data collected for this study were analyzed by using SPSS WIN PC 20.0. Fisher exact test, chi-squared test, and t test were used for analyzing general characteristics of the experimental and control groups, and homogeneity test on predependent variables. Two-way repeated-measures analysis of variance was used to verify hypotheses in the experimental and control groups.
Results
Homogeneity test in the experimental and control groups
The result of the homogeneity test of general characteristics of the participants showed that no statistically significant differences were observed between the two groups according to age, education, job, religion, income, number of deliveries, number of weeks of pregnancy, types of delivery, whether the women participated in prenatal education, and the method of breast-feeding (Table 1).
Unless otherwise noted, values are expressed as number (percentage).
Fisher exact test.
The result of the homogeneity test between the experimental and control group on immune responses before the laughter therapy intervention also showed no significant differences between the two groups (Table 2).
Unless otherwise noted, values are expressed as mean ± standard deviation.
Hypothesis testing
We tested the hypothesis that “compared with those in the control group, the experimental group participating in laughter therapy will show little decrease in breast milk sIgA”. The average amount of breast milk sIgA for the experimental group was 784.92 mg/dL at pretest and 486.84 mg/dL at post-test, while that of the control group averaged 772.72 mg/dL at pretest and 213.39 mg/dL at post-test. Analysis of the results showed that breast milk sIgA of the control group decreased quite sharply when compared with that of the experimental group; thus, there was a significant difference between the two groups (F = 24.06; p < 0.001), between test measurement times (F = 311.31; p<0.001), and between measurement times and reciprocal actions (F = 28.90; p < 0.001). Therefore, the hypothesis is supported (Table 3, Figs. 2 and 3).

Change of secretory IgA (sIgA) in breast milk by time (individual data). Cont, control group; Exp, experimental group.
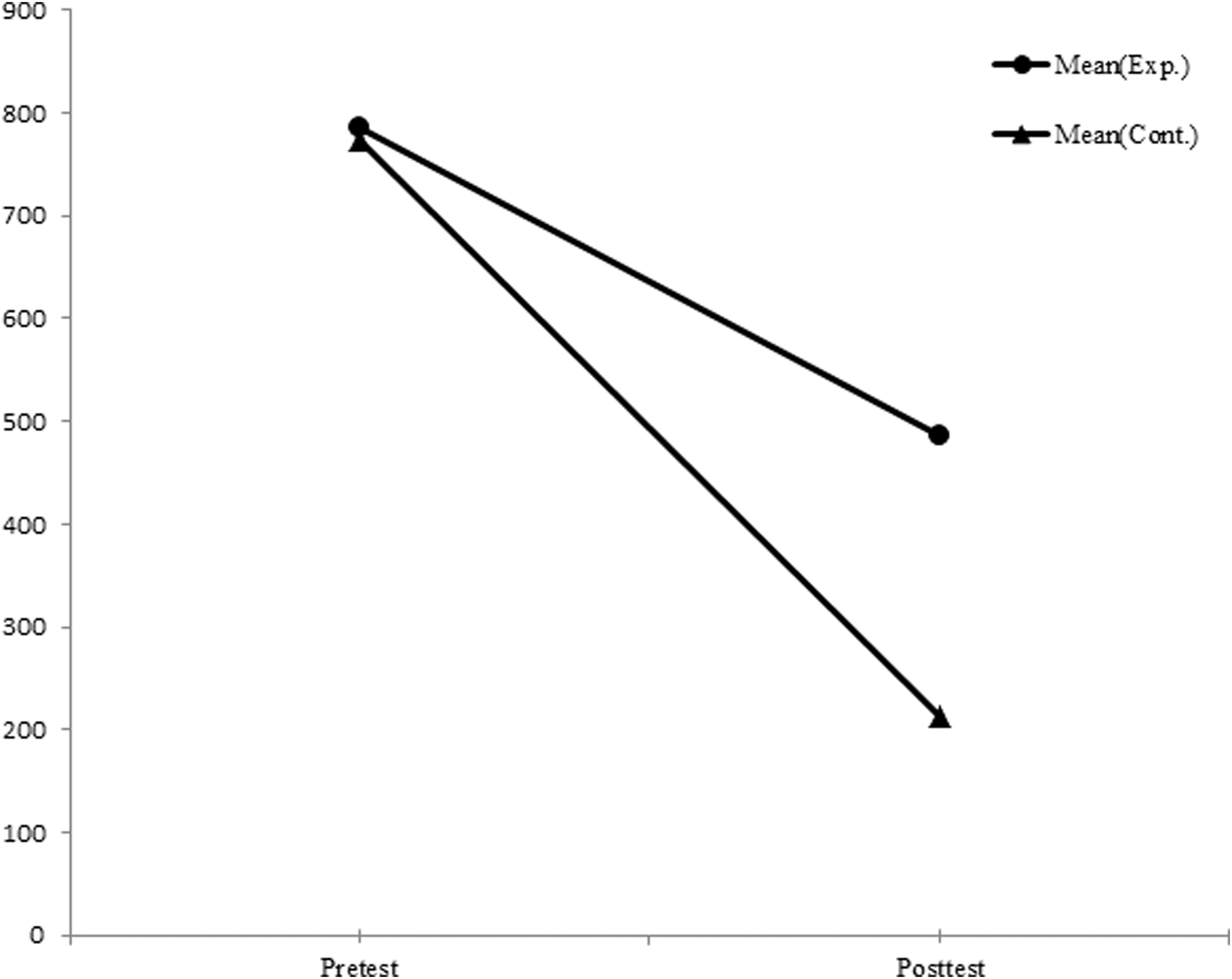
Change of secretory IgA (sIgA) in breast milk by time (mean).
Unless otherwise noted, values are expressed as mean ± standard deviation.
Discussion
Recent changes in social structures, such as industrialization, nuclearization of family, and increase in the employment of parents who help with postpartum care and child-raising, are causing difficulties in providing traditional postpartum care at home for women in Korea. Thus, health care for these women is being provided in Sanhujoriwon facilities, which assist with postpartum care.
This study provided the postpartum laughter program to women during puerperium care in a Sanhujoriwon facility and tested effects on breast milk sIgA.
While previous studies on laughter therapy interventions should have had more rigorous and theoretically informed research, some previous studies have shown effects on the endocrine system or immune responses as well as physiologic functions of the human body. 11,24,25,32
Because the participants in the current study were women who had recently given birth, immune responses were measured not through serum but through the noninvasive method of assessing sIgA in breast milk. This study for changes in breast milk sIgA after the postpartum laughter program was investigated as a small number of studies; therefore, limitations exist in discussing the results of this study.
This study sought objective results by scientifically testing the effects of laughter therapy with the physiologic index for the effects on immune response in the sIgA of breast milk, and results showed a slight decrease in the experimental group. Density of breast milk sIgA is highest in colostrum after delivery and physiologically decreases after deliver with time; previous studies 28,29 have identified these slight differences. Post-tests in this study were done at a time when the amount of breast milk sIgA started to decrease physiologically; the amount decreased in both the experimental and control groups. However, although the decrease in the level of breast milk sIgA among the women participating in the postpartum laughter program was small, the postpartum laughter program affected the secretion of breast milk sIgA. Density of breast milk sIgA after the intervention (16th day after vaginal delivery, 19th day after caesarean delivery) could be attributed to a physiologic decrease rather than the density of breast milk sIgA before the intervention (third day after vaginal delivery, sixth day after caesarean delivery), but the interpretation of the result does not address the problem of the density of breast milk sIgA being checked at the same time for both groups.
Lee 33 differed from this study in terms of the intervention method; that study investigated the difference of breast milk IgA before and after an intervention of aroma massage for 20 minutes once a day for 3 days (from the third to the fifth day after caesarean delivery). Levels were 247.2 mg/dL before intervention and 135.5 mg/dL after intervention in the experimental group and 298.2 mg/dL before intervention and 180.0 mg/dL after intervention in the control group, with no statistically significant differences.
Many previous studies tested the effects of NK cell function and NK cell activity 24 –26,32 on immune responses after applying laughter therapy; they report that laughter therapy has a positive effect on immune factors. Martin, 34 in a review of previous studies on humor, laughter, and physical health, reported significant correlations between humor and immunity. Cho and Oh 11 also provided laughter therapy twice a week for 4 weeks to 37 patients with breast cancer (16 in the experimental group, 21 in the control group) and reported no effects on immune responses (total T cell, total B cell, NK cell). The participants were cancer survivors who had completed radiotherapy and chemotherapy after surgery, which may have affected their immune function, and the examination results of the participants before the experiment were recorded as normal.
Recently, the study of laughter therapy has been reported among patients with different diseases or conditions, and programs operated in a variety of ways. 12 In the current study, laughter therapy was applied in a program that considers the characteristics of women; however, verification of the effects in a replicated study and the standardization of the program should also be considered in the future.
In this study, the schedule and activities of the Sanhujoriwon facility were already fixed, so the program had to be applied within a restricted structure. Known restrictions were that the program was held twice a week, for a total of four times over 2 weeks, and during an intervention period that took place in a 1- to 2-week stay in the Sanhujoriwon facility. Intervention effects at a later time and the sustainability of the effects should be checked in a study that includes women returning for follow-ups.
In addition, laughter programs often include laughing loudly, and the women in the Sanhujoriwon facility who did not participate in the program might be bothered by the noise; thus, a properly enclosed location for the experimental medical treatment is needed.
The intervention in this study provides laughter therapy as a complementary therapy during puerperium recovery and health care for these women. Laughter therapy is a safe intervention that does not require any special techniques or equipment. It is applicable as a self-care method for puerperal women and their families and as a service program in the clinical field or Sanhujoriwon facilities in Korea.
Although this study was conducted to test the effects of laughter therapy, the sample consisted only of postpartum women during their stay in the affiliated Sanhujoriwon facility of one hospital located in Gyonggi Province. Thus, results should be generalized with caution.
In conclusion, this study used a nonequivalent control group with a non-synchronized design to test the effects of laughter therapy on immune responses (sIgA) in postpartum women. Because the laughter therapy resulted in statistically significant differences in the amount of breast milk sIgA, the study suggests that the therapy affects immune responses in postpartum women. Therefore, the postpartum laughter program used in this study can be accepted and used in the clinical field as an element of evidence-based nursing for puerperium recovery and health care of women whom have recently given birth.
On the basis of the study results, the following are proposed: First, subsequent studies are needed to verify the effects and sustainability of the laughter therapy. Second, a longitudinal study is needed to refine the frequency and length of sessions of laughter therapy in the puerperium and to account for diversely related variables. Third, replicated studies that apply postpartum laughter programs are needed, and studies in which the results and study design allow for comparisons with other interventions should be done to further verify the effects of laughter therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.