
Abstract
Objectives:
This study sought to (1) assess the effectiveness of acupuncture and moxibustion with a method of soothing the liver and regulating the mind on the quality of life among patients with depression and (2) study the sex differences of acupuncture and moxibustion in the treatment of depression on the basis of patient-reported outcomes.
Methods:
In a single-blind, randomized, controlled trial conducted in Guangdong Province, China, in January and December 2010, 163 patients who met the criteria for depression were enrolled. Eligible patients were allocated to three treatment groups (soothing liver and regulating mind group, acupoint shallow puncturing group, and non-acupoint shallow puncturing group). In all three groups, the treatment was given twice a week for 12 weeks. The Hamilton Depression Rating Scale (HAMD) and Symptom Checklist 90 (SCL90) were used to quantitatively assess patients before and 1 and 3 months after treatment.
Results:
Non–statistically significant differences in the acupuncture and moxibustion therapeutic effects of soothing liver and regulating mind treatment were found between men and women (p>0.05). An item-by-item analysis of the SCL90 and HAMD scores showed sex differences between the efficacy of the soothing liver and regulating mind group and the group receiving acupoint shallow puncturing. Women obtained lower scores in somatization, interpersonal relationship, anxiety, terror, and extremeness items and HAMD scores in the soothing liver and regulating mind group than in the acupoint shallow puncturing group (p<0.05), while men showed no significant differences between the soothing liver and regulating mind group and the acupoint shallow puncturing group (p>0.05).
Conclusions:
The therapeutic effect of soothing liver and regulating mind is similar for both sexes, but women were more sensitive to the efficacy of the soothing liver and regulating mind treatment compared with other methods. These findings could indicate an important issue to consider for the different acupuncture and moxibustion treatments for depression in men and women.
Introduction
D
Epidemiologic studies conducted over the last three decades in different countries have consistently showed that women are more than twice as likely as men to have major depression. They also have higher rates of seasonal affective disorder, depressive symptoms in bipolar disorder, and dysthymia. 2,3 Genetic vulnerability, hormones, and environmental stress all contribute to women's increased susceptibility to depression. Some researches suggest that women may be more likely to ruminate over events than men do and are more prone to depressed. 4
Some recent advances in acupuncture research show that acupuncture can provide longer-term benefits for many patients with ongoing depression. 5 In view of antidepressants' adverse effects, acupuncture and moxibustion as non-pharmacologic treatments for depression are increasingly being used to improve long-term outcomes, with the hope that they might avoid some of the concerns regarding antidepressant safety and dependency. 6 According to Traditional Chinese Medicine (TCM) theory, the main pathogenesis of depression is stagnation of liver qi, which means the presence of stress in the body. Liver is responsible for the smooth flow of qi (energy) throughout the body and smoothing emotions. In Chinese medicine, liver qi stagnation is the initial stage of depression, and the heart's failure to control the spiritual of the emotional is the main pathogenesis of depression in Chinese medicine. 7 Acupuncture and moxibustion with a method of soothing the liver and regulating the mind can provide obvious curative effect for patients who have depression, with the advantage of security. 8
Previous studies of sex differences in response to acupuncture treatment have confirmed that women seek complementary treatment, including acupuncture, more frequently than do men. 9 In a cross-correlation analysis of brain networks during acupuncture in 38 participants (19 women and 19 men) who had brain functional magnetic resonance imaging during acupuncture, Qiu et al. found sex differences in the limbic-paralimbic-neocortical network or the default mode network; coherent activities in these networks are significantly stronger in women than in men during acupuncture needle manipulation and play a primary role in regulating emotion. 10,11 Yang et al. also found that women showed a higher likelihood of response and remission in terms of depressive syndrome, and women had shorter times for Hamilton Depression Rating Scale (HAMD) and other clinical assessments responses. 12
Currently, few acupuncture and depression studies have examined sex differences in Asians. Because sex differences are shown in response to acupuncture treatment and those neural networks in brain are also affected by acupuncture, the hypothesis of the current study is that women and men may have different responses to different acupuncture treatments, based on the theory of TCM. This study, using three different treatment groups, (1) investigated the effectiveness and safety of acupuncture group of soothing the liver qi and regulating the mind in the treatment of depression and (2) compared the differences and similarities between men and women in response to acupuncture and moxibustion treatments based on patient-reported outcomes.
Materials and Methods
Sample size estimation
A multigroup randomized controlled trial was conducted and the multiple sample mean estimate formula was used for sample size estimate:
According to the formula, each group must consist of about 41 participants. Considering the maximum allowable dropout rate of 15% in the observation process, the sample size was 165 participants.
Participants
The Guangzhou University of Chinese Medicine research board and ethics committee approved the study protocol. Participants with major depression were recruited from the outpatient department of Guangdong Provincial Hospital between January and December 2010. The inclusion criteria were as follows: (1) adults aged 18–70 years diagnosed with major depressive disorder by a qualified psychiatrist using the International Classification of Diseases, 10th Revision, and the Chinese Classification and Diagnostic Criteria of Mental Disorder, Third Edition; 13 (2) a total score of greater than 20 and less than 35 on the HAMD 24-item edition; and (3) meeting the criteria for “stagnation of liver -qi” and “qi depression transforming into fire” of “depression syndrome” in TCM. Patients were excluded if they had received antidepressants in the preceding 2 weeks, had a severe medical disease, had a history of stroke or other mental disorders, were pregnant or breast-feeding, or had an injury or an infection in the back. All eligible patients gave informed consent to participate.
Randomization
Patients were randomly assigned to one of three groups: soothing liver and regulating mind group, acupoint shallow puncturing group, and non-acupoint shallow puncturing group. Randomization was conducted using the PEMS 3.1 software pack (Sichuan, China). Assignments were placed in sequentially numbered, sealed opaque envelopes, prepared in advance (randomization ratio 1:1:1 for each group, respectively). Patients and efficacy evaluators, apart from the acupuncturist, were blinded to the group allocation throughout the study.
Intervention
All the acupoints used in this study were located in reference to Nomenclature and Location of Acupuncture Points. 14
Soothing liver and regulating mind group
The acupoints used in this group were bilateral LI4 (Hegu), bilateral LR3 (Taichong), GV20 (Baihui), and GV29 (Yintang). The needle size was 0.35×25 mm (Huatuo Suzhou Medical Instruments, Suzhou, China). The depth of vertical insertion was 10–12 mm for LI4 and LR3; the depth, at a angle of 30°, was 4–5 mm between the needle and skin for GV20 and GV29. After achieving de qi needling sensation (e.g., numbness, soreness, distention, heaviness during acupuncture stimulation), dao qi technique acupuncture was applied at the acupuncture points. This manipulation involved lifting, thrusting, and rotating the needle with light and smooth stimulation. Patients were asked to take deep breaths through the nose for the 30 minutes during which the needles were in place.
For moxibustion, the four flower points (bilateral BL17 Geshu and BL19 Danshu) were selected. A round moxa cone 1 cm in diameter and 1 cm high was placed and ignited on the selected points, which were smeared evenly with Wanhua oil. This was done according to the occurrence of flushing and tolerance of the patient. Five cones were applied to each point.
For intradermal needling, bilateral BL15 Xinshu and BL18 Ganshu were selected. The body of the intradermal needle (Hwato branch, 0.22 mm×5 mm) was completely inserted into the points, with the needle handle remaining outside the skin. A medical dressing (5 mm×5 mm) was plastered on the skin below the metal ring of needle handle and then was fixed with a medical dressing (15 mm×15 mm) and retained for 2 days.
The preceding treatments were given twice a week for 12 weeks, with an interval of more than 48 hours between two treatments.
Acupoint shallow puncturing group
For patients in this group, the same acupoints as in the soothing liver and regulating mind group were used, with a 2- to 3-mm needling depth. No lifting, thrusting, or rotating was done, and the needle sensation was not required. A shorter duration of moxibustion and only 1–2 mm of the needle body was inserted into the points during intradermal needling.
Non-acupoint shallow puncturing group
Patients received the spots located 10 mm lateral to LI4 and LR3 and 10 mm to the left side of GV20 and GV29 during the acupuncture procedure, 10 mm lateral to BL17 and BL19 during the moxibustion procedure, and 10 mm lateral to BL15 and BL18 during the intradermal needling procedure, with the same manipulation method as that in the acupoint shallow puncturing group.
Outcome measures
Demographic data and clinical data were collected, including details regarding age, sex, height, weight, education, occupation, health insurance, family history of depression, daily activities, medical history characteristics, and treatment history.
Treatment outcomes were measured by using Symptom Checklist 90 (SCL90) and HAMD. SCL90 comprehensively summarizes the symptoms and signs of a patient from 10 aspects. HAMD is one of the most reliable scales in depression assessment; 15,16 it was used as the gold standard of depression diagnosis in this study. Scores were assessed at four time points: before and immediately after treatment and 1 and 3 months after treatment. Higher score on each SCL90 and HAMD item indicates a more severe symptom. All data collectors received training twice a year, with a formal consensus meeting to agree on the application of the assessment instruments.
Statistical analysis
Descriptive statistics and baseline variables were calculated in terms of numbers, percentages, and means±standard deviation. A chi-square test was used to assess sex differences between categorical variables; an independent t-test (parametric analysis) or Mann-Whitney U test (nonparametric analysis) was used to test differences between continuous variables. A paired t-test was used for comparisons before and after treatment within a group, and analysis of variance was used for comparisons among different groups. Repeated-measurement analysis of variance was used for comparison among groups at multiple observation points. Statistically significant sex-related characteristics and clinical variables were included in the multivariate analysis as potential confounders.
Data were analyzed by a statistician blinded to the group allocations using SPSS software, version 19.0 for Windows (IBM, Armonk, NY). Significant levels were reported at p<0.05.
Results
Baseline characteristics
Ultimately, 143 patients completed the study. Six patients withdrew from the soothing liver and regulating mind group (3 because of an inability to receive treatment on time, 1 because of use of an antidepressant, and 2 because of fainting during acupuncture). Eight patients withdrew in the acupoint shallow puncturing group (4 because of an inability to receive treatment on time, 2 because of use of an antidepressant, 2 because of a change in contact information that led to interruption in follow-up). Six patients withdrew in the non-acupoint shallow puncturing group (5 because of use of an antidepressant and 1 because a change in contact information led to interruption in follow-up).
The baseline characteristics according to sex and study group are listed in Table 1. Other than differences in height (F=0.018, p<0.001; F=0.265, p=0.008; F=3.841, p=0.043) and weight (F=3.143, p<0.001; F=0.070, p=0.073; F=1.348, p=0.096) between men and women in the soothing liver and regulating mind group, acupoint shallow puncturing group, and non-acupoint shallow puncturing group, respectively, there were no statistically significant differences between different sexes in the general data (p>0.05). Scores on all dimensions of SCL90 and HAMD did not significantly differ between sexes before treatment among the three groups (all p>0.05), with comparability (Table 1).
Values are mean±standard deviation or number (percentage). Comparing men versus women using independent t-test for continuous variables and chi-square test for categorical variables.
p<0.05.
SCL90 scores
Table 2 shows each patient's dimension scores for SCL90 before and after treatment, with estimated differences.
Values are expressed as the mean±standard deviation.
Compared with the data before treatment in the same group, p<0.05.
Comparison between soothing liver and regulating mind group and non-acupoint shallow puncturing group at the same time point, p<0.05.
Comparison between soothing liver and regulating mind group and acupoint shallow puncturing group at the same time point, p<0.05.
Comparison between acupoint shallow puncturing group and non-acupoint shallow puncturing group at the same time point, p<0.05.
Comparison between men and women at the same time point, p<0.05.
An item-by-item analysis of the SCL90, adjusted for potential confounders (age, height, weight, duration of depression, education, occupation, health insurance, orderly life, family history, any previous treatments for depression), showed statistically significant differences between men and women for the “interpersonal relationships” item after treatment in the soothing liver and regulating mind group. Women had lower scores than men (mean, 1.57±0.40 versus 1.90±0.51; F=0.60; p=0.021).
Comparison of the data at all time points after treatment with those before treatment in the three groups showed the following: In the soothing liver and regulating mind group, except for the score for interpersonal relationships after treatment and terror at 1 month and 3 months after treatment in men and terror at 3 months after treatment in women (p>0.05), there were significant differences in all the other dimensions at all time points as compared with before treatment for both sexes (all p<0.05). In the acupoint shallow puncturing group, scores for the four dimensions (somatization, compulsion, depression, and others) significantly differed (p<0.05) except for somatization in women at 3 months after treatment (p>0.05). There were no statistically significant differences in the scores for interpersonal relationship at all three time points after treatment in men and at 3 months after treatment in women; in the scores for anxiety, hostility, and psychotic behavior at 3 months after treatment for both sexes; and in the scores for terror and extremeness at 1 and 3 months after treatment for both sexes (p>0.05). In the non-acupoint shallow puncturing group, only the depression item showed statistically significant differences at all three time points after treatment for both sexes (p<0.05); statistically significant differences were seen between men and women in other dimensions, as shown in Table 2.
With regard to the efficacy in the soothing liver and regulating mind group after treatment for somatization, interpersonal relationship, anxiety, terror and extremeness, women were more sensitive for the efficacy of soothing liver and regulating mind treatment at each time point after treatment compared with the acupoint shallow puncturing group.
HAMD scores
Table 3 shows a comparison of HAMD scores at all time points before and after treatment among the three groups for both sexes. The data at all time points after treatment compared with those before treatment in the three groups for both sexes were significantly decreased (all p<0.05). In the evaluation of HAMD, the efficacy seen in the soothing liver and regulating mind group and acupoint shallow puncturing group after treatment was better than in the non-acupoint shallow puncturing group for both sexes (all p<0.05). The HAMD reductive ratios 17 were significantly lower in the non-acupoint shallow puncturing group (p<0.05) than in the soothing liver and regulating mind group and acupoint shallow puncturing group (data not shown in Table 3).
Values are expressed as the mean±standard deviation.
Compared with the data before treatment in the same group, p<0.05.
Comparison between the soothing liver and regulating mind group and the non-acupoint shallow puncturing group at the same time point, p<0.05.
Comparison between the soothing liver and regulating mind group and the acupoint shallow puncturing group at the same time point, p<0.05.
Comparison between men and women at the same time point, p<0.05.
Comparison between the acupoint shallow puncturing group and the non-acupoint shallow puncturing group at the same time point, p<0.05.
In the acupoint shallow puncturing group, HAMD scores significantly differed between men and women after treatment and 1 month after treatment. Women had higher scores than men (mean, 12.44±4.27 versus 16.07±5.00; F=0.876; p=0.010 and mean, 13.54±4.06 versus 17.32±5.41; F=3.686; p=0.009); the curative effect of acupoint shallow puncturing treatment for women was inferior to that in men, as shown in Figure 1. However, there were no significant differences between the soothing liver and regulating mind group and the acupoint shallow puncturing group for men.
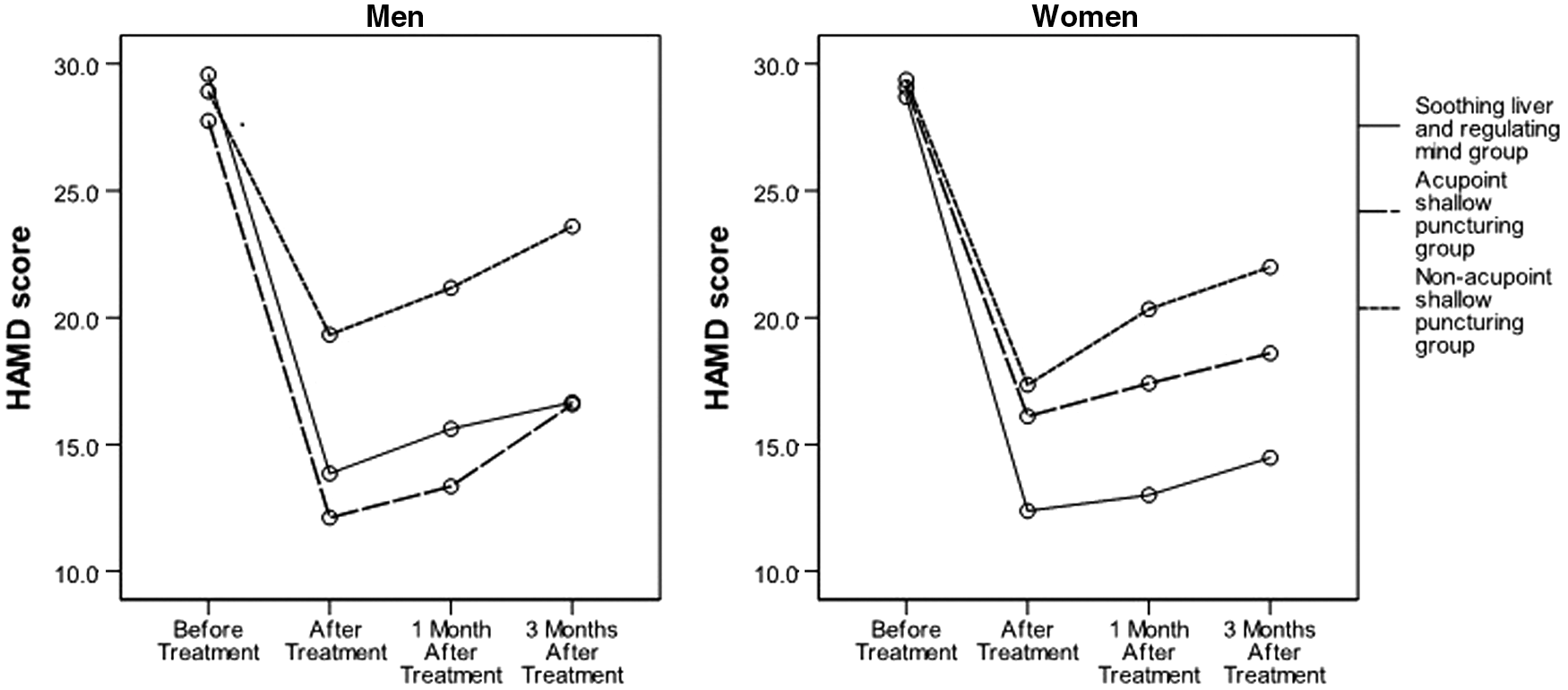
Scores of Hamilton Depression Rating Scale (HAMD) at different treatment stages in men and women.
Discussion
This study is unique in that it compared the sex-related differences in each treatment group and scale scores, which enabled determination of outcomes in a well-defined population. A feature that distinguishes this study from previous similar research was that treatment outcomes were evaluated not only from the level of depression clinical evaluation per se but also from other features of the depressive syndrome (e.g., interpersonal relationships, anxiety, and psychotic behavior). The SCL90 and HAMD scales were used as the clinical assessments of depression in our study; these are well-recognized and standardized evaluation scales.
Clinical experiences in acupuncture have suggested that de qi is necessary for attaining the therapeutic effectiveness of acupuncture. 18 In the present clinical study, placebo-acupuncture (acupoint shallow puncturing and non-acupoint shallow puncturing group) was used as control. Because patients cannot differentiate between real and placebo acupuncture, the soothing liver and regulating mind treatment seemed to provide more evidence on the benefits of de qi. However, an effect of placebo acupuncture cannot be completely excluded considering patients' psychological hint.
When the HAMD reductive ratio was evaluated by sex and treatment groups, statistically significant differences between men and women were found in the acupoint shallow puncturing group after treatment and 1 month after treatment. Men in the soothing liver and regulating mind group and acupoint shallow puncturing group and women in the soothing liver and regulating mind group had made remarkable progress in improving depressive symptoms, according to HAMD reductive ratio (more than 50%), and women in the acupoint shallow puncturing group and both sexes in the non-acupoint shallow puncturing group had amelioration of depressive symptoms (more than 25%). 17 The German Acupuncture Trails also found effects of both acupuncture and sham acupuncture in chronic diseases. 19 Further studies with greater sample size are necessary for further demonstrated.
There were no significant sex differences in treatment-related characteristics, such as medications, psychotherapy, and other acupuncture therapy. The most important finding of this study is the lack of obvious sex differences in acupuncture and moxibustion therapeutic effects by soothing liver qi and regulating mind among depressed patients based on patient-reported outcomes.
Different hypotheses might explain why no sex differences were found in depressed patients receiving soothing liver and regulating mind treatment. First, previous research suggested that more severe depressive symptoms might be associated with women, 20 but in the current study there were no sex differences in the course of depression. The second possible hypothesis is related to gender roles. Although gender roles and responsibilities vary between educations and occupation, 21 women in our study have work status rates similar to those of men, which means both male and female have similar responsibilities and activities at work. The third and most important hypothesis may be associated with the therapeutic effect of soothing liver and regulating mind. The mechanism of depression was derived from the theory of TCM, literature, and clinical practice. The incidence of melancholia in TCM is similar to that of depressive disorder in Western medicine.
It is held that heart and liver disorder is the most common diagnostic type of depression, 22 and it is first put forward that dysfunction of mind and the liver failing in soothing and regulating the circulation of qi are the basic pathogenesis of depression. Although it is unexpected that men and women have no differences with regard to the treatment of soothing liver and regulating mind, it is also important to bear in mind that the intervention of soothing liver and regulating mind combined with acupuncture on patients with depression can relieve depression symptoms and improve psychological functions. This in turn improves their quality of life and prognosis, which can be useful for both men and women. These results are similar to those of others studies. 23,24
Acupuncture may provide remission of depressive symptoms, which is considered a basic goal of acupuncture treatment. 25 However, researchers are conducting further studies on the outcomes of psychological well-being and interpersonal skills. 26 The current study analyzed the SCL90 responses item by item; the remission rate showed differences between the sexes. Women had lower interpersonal relationship item scores than men after treatment in the soothing liver and regulating mind group; for somatization, anxiety, terror, and extremeness items, women were more sensitive in the efficacy of soothing liver and regulating mind treatment than the acupoint shallow puncturing group. This could be an important issue to consider with regard to soothing liver and regulating mind acupuncture approaches.
For the reasons previously described, women were more vulnerable to depression. According to TCM theory, the liver is the key viscus in women's physiology 27 and plays a vital role in women's diseases. Researchers have long suspected that the fluctuations in female hormones, such as estrogen, and the organizational effects of estrogen on brains in utero and postnatally may underlie women's greater vulnerability to depression. 28 The treatment of soothing liver is an effective intervention on sex hormone secretion in depressed patients and is associated with improvement in female patients with depressive mood. 29 As a result it might help make women differentially sensitive to acupuncture compared with men. Thus, for women with depression, the treatment lies in soothing liver and regulating mind. Further research is needed to investigate acupuncture outcomes and the role of sex hormones in women with depression.
Overall, these findings could have important implications for clinicians and scientists seeking to apply acupuncture theory to therapies and research. The lack of significant difference between sexes on the treatment of soothing liver and regulating mind suggests that tailored acupuncture treatment might have benefits for both men and women. The above-mentioned results—that the likelihood of remission is almost the same in men receiving soothing liver and regulating mind treatment and those receiving treatment with acupoint shallow puncturing—suggest the need for further research on ways to improve outcomes in men. Treatment of depressed men therefore should focus on acupuncture that considers brain activity, pain tolerability, and response rates. The stronger response in women on the treatment of soothing liver and regulating mind will help to improve both diagnosis and treatment outcomes of depression among women.
As the first study addressing sex differences in outcomes on different acupuncture and moxibustion treatments among depressed patients, this study should be seen in light of some strength and limitations. The first strength was its comparison of three groups of acupuncture and moxibustion treatments, which could provide a profile of their efficacy in depression treatment. Second, including both men and women in the three groups could reveal sex-related differences of acupuncture and moxibustion therapeutic effects. Finally, the time frame of 12 weeks was relatively appropriate for the assessment of depression improvement. However, because SCL90 and HAMD are self-reported questionnaires, they may be prone to overestimation or underestimation, which could affect the results. In addition, other variables that might influence the results, such as possible marriage status and living conditions, were not considered. Another possible limitation is the representativeness of the sample. A large sample was needed to analyze the effect of different variables on different sexes. Further research to overcome the limitations is recommended.
In conclusion, this study highlights important aspects of the effectiveness of acupuncture and moxibustion on quality of life among patients with depression. It shows that the acupuncture and moxibustion therapeutic effects of soothing liver and regulating mind treatment are similar for both sexes. What's more, women were more sensitive to the efficacy of soothing liver and regulating mind treatment compared with other treatment methods. These findings could be an important issue to consider in different acupuncture and moxibustion treatments and in the medium- and long-term treatment of depression for men and women.
Footnotes
Acknowledgments
This research was financially supported, in part, by the National Natural Science Foundation of China (no. 81303041), the Class General Financial Grant from the China Postdoctoral Science Foundation (no. 2012M511784), Science Foundation of the Outstanding Young Innovative Personnel of Department of Education Guangdong Province (no. 2012LYM_0043), Special Research Foundation of the New Teacher Category for the Doctoral Program of Higher School by National Ministry of Education (no. 20124425120005), science foundation of the postdoctoral researchers in Guangzhou University of Chinese Medicine from Guangdong Provincial Department of Human Resources and social security fund (no. BBK429122K19).
Author Disclosure Statement
No competing financial interests exist.