
Abstract
Objectives:
Patients in Taiwan with allergic rhinitis seek not only Western medicine treatment but also Traditional Chinese Medicine treatment or integrated Chinese–Western medicine treatment. Various studies have conducted pairwise comparison on Traditional Chinese Medicine, Western medicine, and integrated Chinese–Western medicine treatments. However, none conducted simultaneous analysis of the three treatments. This study analyzed patients with allergic rhinitis receiving the three treatments to identify differences in demographic characteristic and medical use and thereby to determine drug use patterns of different treatments.
Materials and Methods:
The National Health Insurance Research Database was the data source, and included patients were those diagnosed with allergic rhinitis (International Classification of Diseases, Ninth Revision, Clinical Modification codes 470–478). Chi-square test and Tukey studentized range (honest significant difference) test were conducted to investigate the differences among the three treatments.
Results:
Visit frequency for allergic rhinitis treatment was higher in female than male patients, regardless of treatment with Traditional Chinese Medicine, Western medicine, or integrated Chinese–Western medicine. Persons aged 0–19 years ranked the highest in proportion of visits for allergic rhinitis. Traditional Chinese Medicine treatment had more medical items per person-time and daily drug cost per person-time and had the lowest total expenditure per person-time. In contrast, Western medicine had the lowest daily drug cost per person-time and the highest total expenditure per person-time. The total expenditure per person-time, daily drug cost per person-time, and medical items per person-time of integrated Chinese–Western medicine treatment lay between those seen with Traditional Chinese Medicine and Western medicine treatments.
Conclusions:
Although only 6.82 % of patients with allergic rhinitis chose integrated Chinese–Western medicine treatment, the visit frequency per person-year of integrated Chinese–Western medicine ranked highest. In addition, multiple-composition medicines were used more frequently than single-composition medicines, and mar huang (Ephedra sinica Stapf) was seldom used to decrease the risk of combining medications.
Introduction
T
Although allergic rhinitis is not a highly fatal disease, it can disrupt patients' social activities, work, learning, and sleeping and decrease their quality of life. 12 According to the findings of epidemiologic studies, asthma frequently coexists with allergic rhinitis in the same patient. Moreover, allergic rhinitis is one of the dangerous features of asthma. 4,11 In addition to receiving treatment with such medications as antihistamine, decongestant agents, cromolyn sodium, montelukast, and ipratropium bromide, patients should avoid exposure to allergens. For those who have poor response to medications and cannot avoid allergens, allergen immunotherapy, also called hyposensitization, is available. 10,13 In addition, according to Traditional Chinese Medicine theory, differential symptoms and treatments are efficacious against allergic rhinitis. 14 –16
When the National Health Insurance (NHI) of Taiwan launched in 1995, the program reimbursed for Traditional Chinese Medicine. As a result, patients in Taiwan with allergic rhinitis sought not only Western medicine treatment but also Traditional Chinese Medicine treatment to improve allergic physique. 16 –18 The reason is that Chinese people believe that Western medicine has quicker effects but more side effects, whereas Traditional Chinese Medicine has slower effects but greater safety. 19 –21 Consequently, patients with chronic or recurrent diseases often integrate Chinese medicine and Western medicine into their treatment plan, especially patients with allergic rhinitis. 22 –25 Various studies conducted pairwise comparisons among patients with allergic rhinitis treated with the three treatments (Traditional Chinese Medicine alone, Western medicine alone, and integrated Chinese–Western medicine). However, none conducted simultaneous analysis on the three treatments. 26 –29 The current study analyzed the three treatment methods to illustrate the differences in demographic characteristic and medical use in order to determine drug use patterns of different treatments.
Traditional Chinese Medicine and Western medicine almost operate in separate treatment divisions in Taiwan. Only a few medical institutions provide outpatient departments of integrated Chinese medicine and Western medicine. 30 Patients seek Traditional Chinese Medicine treatment and Western medicine treatment separately. Because most patients seldom report to physicians that they are receiving other treatments, physicians often are unaware of patients' other medicines.
In recent years, some research showed that taking Chinese medicines and Western medicines at the same time can cause severe drug–drug interactions.
17,31
–34
Generally speaking, Traditional Chinese Medicine prescribed to treat allergic rhinitis often consists of mar huang (Ephedra sinica Stapf), which induces perspiration (diaphoresis) and soothes asthma. Besides, The components of mar huang, such as ephedrine and
Therefore, this study sought to explore the NHI claims data in Taiwan to determine the pattern of use of integrated Chinese–Western medicine treatments for allergic rhinitis. It is hoped that the results will be helpful in the formation of recommendations for and health education of integrated treatment of Chinese medicine and Western medicine.
Materials and Methods
In 1998, the National Health Research Institutes in Taiwan established and managed the NHI Research Database (NHIRD) on the basis of claims data from the NHI to allow academic and nonprofit organizations to conduct medical research. The Chinese medicines reimbursed by the NHI are limited to extract Chinese medicines, and raw medicinal substances and other herb medicines are excluded.
This study population consisted of patients with allergic rhinitis from the 2009 NHIRD; 200,000 patients were drawn as samples from the registry for beneficiaries by random sampling. Patients with allergic rhinitis were classified into three categories by their treatment: Traditional Chinese Medicine alone, Western medicine alone, and integrated Chinese–Western medicine. After exclusion of patients treated with Traditional Chinese Medicine or Western medicine but not the other one, those who sought Traditional Chinese Medicine treatment and Western medicine treatment were included in the integrated Chinese–Western medicine group. The differences in demographic characteristic and medical use among the three categories were analyzed.
According to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM), patients diagnosed with allergic rhinitis with subcategories (codes 470–478) were selected as the study patients. SAS software, version 9.13 (SAS Institute, Cary, NC), was used for data analysis. Chi-square test was used to test the effect of sex and age on visit option for Traditional Chinese Medicine, Western medicine, or integrated Chinese–Western medicine treatments. Analysis of variance (ANOVA) and Tukey studentized range (honest significant difference [HSD]) test were used to illustrate the difference in visit frequency per person-year, total expenditure per person-time, daily drug cost per person-time, and medical items per person-time among the three treatments.
In addition, the use of hypnotics in Traditional Chinese Medicine and Western medicine were explored by using records in which the first three characters of the 7seven-character code were N05. These Traditional Chinese Medicines included su tsang pu (Acori tatarinowii Rhizoma), suan zau rirn (Ziziphi spinosae Semen), ling zu (Ganoderma australe Fr.), bor zu rirn (Platycladus orientalis L.), yen zu (Polygala tenuifolia Willd.), hir huan pee (Albizzia julibrissin Durazz), hir soe wu (Polygonum multiflorum Thunb.), and suan zau rirn tang (multiple-composition containing Ziziphi spinosae Semen, Glycyrrhiza uralensis Fisch, Anemarrhena asphodeloides Bunge, Peltandra virginica, and Ligusticum chuanxiong Hort). Western medicines included alprazolam, diazepam, estazolam, lorazepam, mephenoxalone, fludiazepam, zolpidem hemitartrate, chlordiazepoxide HCl, oxazolam, and zolpidem tartrate. 42,43 The research framework is shown in Figure 1.
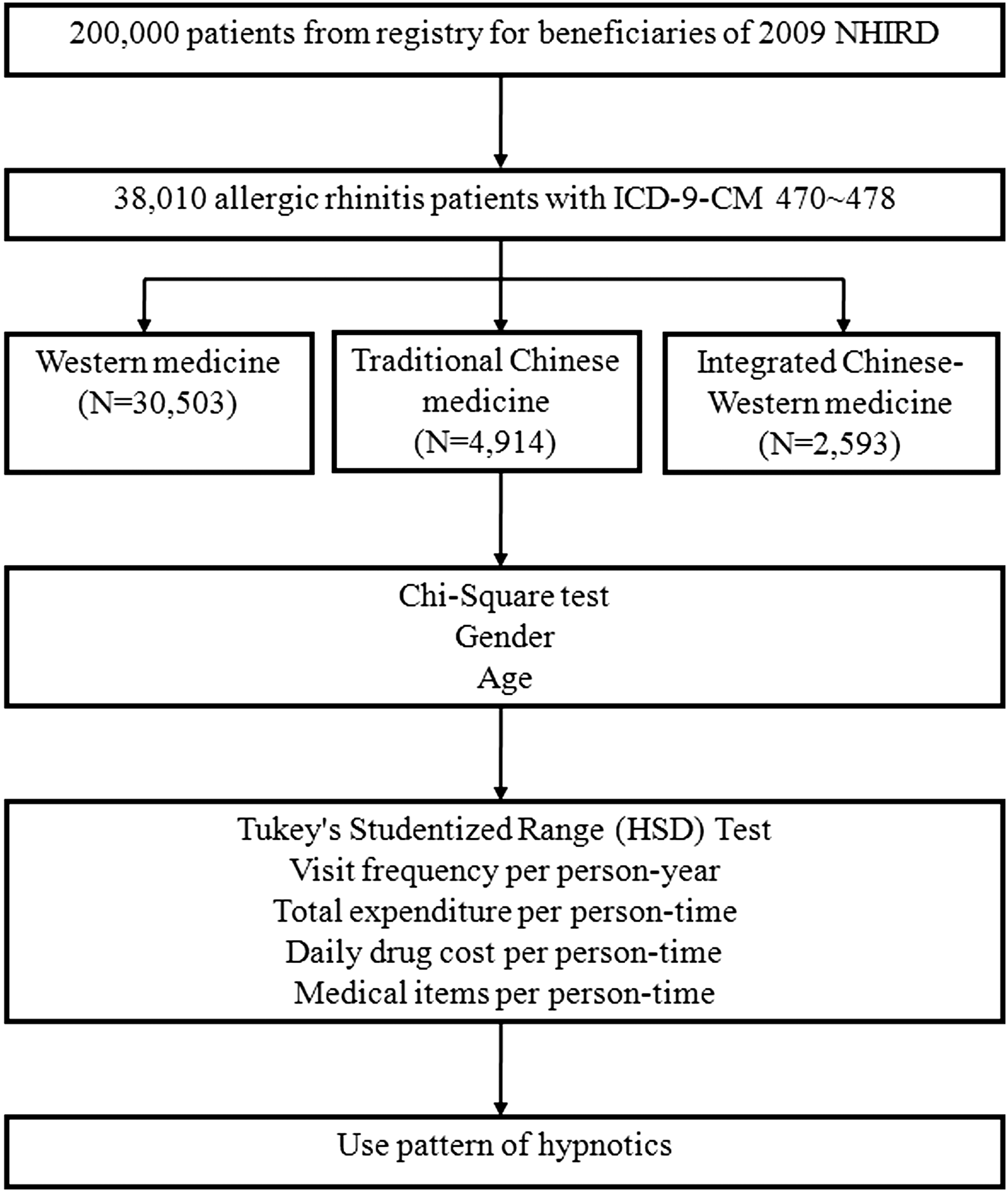
Research framework. HSD, honest significant difference; ICD-9-CM, International Classification of Diseases, 9th Revision, Clinical Modification; NHIRD, National Health Insurance Research Database.
Results
According to the research design, 38,010 patients diagnosed with allergic rhinitis according to ICD-9-CM codes 470–478 were selected. A total of 30,503 subjects received Western medicine treatment, 4914 received Traditional Chinese Medicine treatment, and 2593 received integrated Chinese–Western medicine treatment.
This study analyzed 17,706 male (46.58%) and 20,304 female (53.42%) patients. The Western medicine group consisted of 14,285 male (46.83%) and 16,218 female (53.17%) patients; the Traditional Chinese Medicine group, 2191 male (44.59%) and 2723 female (55.41%) patients; and the integrated Chinese–Western medicine group, 1230 male (47.44%) and 1363 female (52.56%) patients. A chi-square test of independence was performed to examine the relation between sex and treatments. The relation between these two variables was significant (p = 0.0092), as shown in Table 1.
The average age of all patients was 31.60 ± 19.94 years. In the three treatment groups, the average ages were 32.78 ± 21.79 years for the Western medicine group, 30.16 ± 18.53 years for the Traditional Chinese Medicine group, and 26.83 ± 19.49 years for the integrated Chinese–Western medicine group (Table 2).
SD, standard deviation.
As shown in Table 2, among patients with allergic rhinitis treated by Western medicine, the highest proportion consisted of those age 0–9 years (19.15 %), followed by 10–19 years (14.57 %). Among those treated by Traditional Chinese Medicine, the highest proportion comprised those 10–19 years of age (22.06%), followed by those 30–39 years of age (16.71%). Among those treated by integrated Chinese–Western medicine, the highest proportion consisted of those age 0–9 years (24.26%), followed by those age 10–19 years (21.94%). A chi-square test of independence performed to examine the relation between age and treatments showed a significant relation between these two variables (p < 0.0001), as shown as Table 3.
In this study, after exclusion of patients treated with Traditional Chinese Medicine or Western medicine but not the other one, those who sought Traditional Chinese Medicine treatment and Western medicine treatment were included in the integrated Chinese–Western medicine group. A total of 117,857 visits with 38,010 patients diagnosed with allergic rhinitis were sampled from NHIRD. There were 83,257 visits (70.64%) for Western medicine, 16,283 visits (13.82%) for Traditional Chinese Medicine, and 18,317 visits (15.54%) for integrated Chinese–Western medicine.
By ANOVA and Tukey studentized range (HSD) test among patients treated by Traditional Chinese Medicine, Western medicine, and integrated Chinese–Western medicine, the visit frequency per person-year of integrated Chinese–Western medicine ranked first as 7.06 ± 6.07, followed by Traditional Chinese Medicine with 3.31 ± 4.11 and Western medicine with 2.72 ± 3.24. The difference was statistically significant (p < 0.0001), as shown in Tables 4 and 5.
I, Integrated Chinese–Western medicine; T, Traditional Chinese Medicine; W, Western medicine.
According to ANOVA analysis and Tukey studentized range (HSD) test, the medication items per person-visit were greatest for Traditional Chinese Medicine at 5.77 ± 2.53, followed by integrated Chinese–Western medicine at 4.67 ± 2.48 and Western medicine at 3.55 ± 1.77. The difference was statistically significant (p < 0.0001), as shown in Tables 6 and 7.
ANOVA and Tukey studentized range (HSD) test showed that the total expenditure per person-time was highest for Western medicine at 594.33 ± 1374.70 New Taiwan Dollar (TWD), followed by integrated Chinese–Western medicine at TWD 555.97 ± 669.67 and Traditional Chinese Medicine at TWD 514.27 ± 145.59. The difference was statistically significant (p < 0.0001), as shown in Tables 8 and 9.
By ANOVA and Tukey studentized range (HSD) test, The daily drug cost per person-time was highest for Traditional Chinese Medicine at TWD 29.99 ± 0.08, followed by integrated Chinese–Western medicine at TWD 24.69 ± 14.75 and Western medicine at TWD 18.13 ± 77.98. The difference was statistically significant (p < 0.0001), as shown in Tables 10 and 11.
Finally, as shown in Table 12, among the top 25 prescription medicines, the top 8 Western medications were almost the same for the Western medicine and the integrated Chinese–Western medicine treatments. The top 4 herbal medications (shin yee ching fay tang, shau ching long tang, shin yee san, and tsang err san shin yee ching fay tang) were multiple-composition formulas and had the same ranking for both Traditional Chinese Medicine and integrated Chinese–Western medicine treatments. Table 13 contains cross-references between Traditional Chinese Medicine names and botanical plant names.
Discussion
Previous research showed that males had a higher probability of developing allergic rhinitis than females. 4 However, this study based on NHIRD data showed a greater probability among female patients regardless of treatment with Traditional Chinese Medicine, Western medicine, or integrated Chinese–Western medicine. Younger children (age 0–9 years) had the highest visit frequency in Western medicine and integrated Chinese–Western medicine groups, whereas adolescents (age 10–19 years) ranked the highest in Traditional Chinese Medicine group. In other words, younger patients accounted for a greater proportion of those with allergic rhinitis. Although patients with allergic rhinitis mostly chose Western medicine, Western medicine clinics had the lowest visit frequency, whereas integrated Chinese–Western medicine had the most.
From the analysis of total expenditure per person-time, daily drug cost per person-time, and medical items per person-time, Traditional Chinese Medicine treatment had more medical items per person-time and higher daily drug cost per person-time. However, drug cost does not make up the greatest proportion of total expenditure. Traditional Chinese Medicine treatment had the highest daily drug cost per person-time but the lowest total expenditure per person-time. In contrast, Western medicine had the lowest daily drug cost per person-time but the highest total expenditure per person-time. As for the integrated Chinese–Western medicine, its total expenditure per person-time, daily drug cost per person-time, and medical items per person-time all lay between those of Traditional Chinese Medicine and Western medicine (Table 14). The results showed that patients with allergic rhinitis in Taiwan could chose Western medicine with the expectation of rapid therapeutic effects but greater expenditure. Those who chose Traditional Chinese Medicine could expect improvement in allergic physique by taking more medications but paying the least. The expectation for integrated Chinese–Western medicine is not only rapid therapeutic effects but also improvement in the allergic physique; this treatment entailed the mid-range number of medical items and had expenditure between that of the other two treatments. It might be a good option for patients with allergic rhinitis.
Significant difference in Tukey studentized range (honest significant difference) test (p < 0.05).
TWD, New Taiwan Dollar.
Western medicine treatment used more hypnotics than the other two treatments, whereas integrated Chinese–Western medicine treatment used the least. The significant difference is shown in Table 15.
Conclusions
As the findings of this study showed, among patients with allergic rhinitis treated by Western medicine and integrated Chinese–Western medicine, the highest proportion consisted of those age 0–9 years of age, followed by those 10–19 years, compared with 10–19 years followed by 30–39 years for those receiving Traditional Chinese Medicine. It is suggested that adults have a stronger inclination toward Traditional Chinese Medicine than young patients. Most TCMs are in powder form, and it is difficult for children younger than age 10 years to take this form of medicine without choking. The bitter taste of TCM is also almost universally unpleasant to younger patients, even though the powder form can be made into a more palatable elixir. That is why children age 0–9 years old are less inclined to receive TCM than other age groups. In addition, the total expenditure per person-time, daily drug cost per person-time, and medical items per person-time for integrated Chinese–Western medicine treatment all lay between those for Traditional Chinese Medicine treatment and Western medicine treatment. This finding suggests that integrated Chinese–Western medicine treatment might be a good option for allergic rhinitis. On the other hand, although only 6.82% of patients with allergic rhinitis chose integrated Chinese–Western medicine, the visit frequency per person-year was highest for integrated Chinese–Western medicine. This indicates that these patients would accept Traditional Chinese Medicine treatment and Western medicine treatment by turns in a short period of time. Furthermore, the fact that multiple-composition medicines were used more frequently than single-composition medicines in Traditional Chinese Medicine treatment and integrated Chinese–Western medicine treatment suggests that the synergistic effects of multiple-composition medicines were recognized as appropriate for most patients.
Finally, mar huang (Ephedra sinica Stapf) appeared only in two multiple-composition formulas (gir girn tang and shau ching long tang), accounting for 7.11% and 4.3% of prescriptions in Traditional Chinese Medicine treatment and integrated Chinese–Western medicine treatment, respectively. That means that the risk of combining drugs could be decreased.
In conclusion, this study of patterns of use of integrated Chinese–Western medicine treatment provides preliminary findings that deserve more extensive research in the future.
Footnotes
Acknowledgments
This study is based in part on data from the NHIRD provided by the Bureau of National Health Insurance, Department of Health, and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health, or National Health Research Institutes.
Author Disclosure Statement
No competing financial interests exist.