
Abstract
Background:
Childhood constipation is a common ailment that in certain cases can lead to encopresis or fecal incontinence. The literature suggests that standard care varies in effectiveness, especially in the long term. Fecal incontinence can lead to frustration, guilt, and shame for both the child and family and has untold long-term psychological and physical consequences.
Objective:
To address alternative treatment options for pediatric constipation and encopresis by using acupuncture and Chinese medicine.
Patient and Setting:
This is a case study of a 6-year-old girl seen in a private practice acupuncture clinic in the northwestern United States.
Intervention:
Treatment involved acupuncture, massage, and Chinese herbal medicine.
Results:
The patient in this study began to have regular bowel movements on her own, from a type 5 on the modified Bristol Stool Form Scale for Children to a type 3, with no laxative use and few to no fecal accidents.
Conclusions:
Emotional stability and support seem to play an important role in pediatric constipation and encopresis. Acupuncture may be an effective treatment option in the integrative care model to address both the emotional and physical components of childhood constipation.
Introduction
E
Some of the literature suggests that there is a high correlation between encopresis and attention-deficit/hyperactivity disorder (ADHD) and that children with ADHD are significantly more likely to have constipation and fecal incontinence with or without medications. 1,11 The connection may stem from the lower likelihood of children with ADHD to respond as promptly to their body's cues for defecation, but it has also been proposed that perhaps the shame involved in soiling themselves leads to the misbehaviors that may be mistaken as ADHD. 1,11 In almost all studies, boys are disproportionately more likely to have constipation and encopresis than girls; 1,2,11 however, women are more likely to have constipation than men in adulthood. 12
Standard treatment requires first ruling out a structural issue, specifically Hirschsprung disease, which is a congenital mega colon due to the absence of myenteric plexuses in the bowel wall. 13 Symptoms of Hirschsprung disease begin in infancy and involve chronic constipation leading to mega colon of impacted feces. 13 Once encopresis is diagnosed, standard therapy involves treating the constipation with laxatives, enemas, and suppositories, and sometimes manual removal of impacted feces. Another treatment is behavioral modification known as toilet-sitting, in which the child practices sitting on the toilet to release the bowels. 7,9,11 In more severe cases, surgery and colectomy is performed. 11
Case Description
A 6-year-old girl was brought to the author's clinic for symptoms relating to her constipation and encopresis diagnosis given by her primary care physician. She had been having constipation since infancy; and even after potty training was complete she still preferred to use a diaper. At her initial visit, it was noted that she would go several days without a bowel movement, followed by fecal incontinence at sporadic times. Her pediatrician had diagnosed encopresis due to low muscle tone. The treatment protocol so far had been taking a laxative (Miralax; Bayer Corp., Robinson Township, PA) daily for the last 6 months, with occasional suppositories if she had gone more than 5 days with no bowel movement. She had also been doing behavioral modification of toilet sitting every evening for 5 minutes at a time with the hope of encouraging a bowel movement.
The patient did not report pain during a bowel movement but had mentioned to her mother in the past of a fearfulness of it. Stool varied between being loose and formed, was more often loose, and usually was a “brownish-greenish” color, ranking between a type 4 and type 5 on the modified Bristol Stool Form Scale for Children (mBSFS-C). 14 No accidents were reported at night while sleeping; all fecal accidents occurred in the day. Her mother reported the child's temperament as being “sensitive and highly affected by what is going on around her.” On the day of her initial visit, she also had a 100.9°F (37.8°C) temperature along with fatigue; several of her classmates had been out sick from school that week.
Physical examination of the patient showed a willowy and thin build. She had weak muscle tone in her legs, especially the right. In addition, her entire abdomen was very tight and hard with palpable hardened stool along the transverse colon. She also had extreme hypertonicity bilaterally along the erector spinatus muscles from T7 to L2. The patient's abdomen and feet were cold to palpation. Her pulse was rapid but weak; tongue was pale and flabby, moist with no coat. AcuGraph digital meridian imaging readings (Miridia Acupuncture Technology, Meridian, ID) were taken the first, second, and eighth visits and indicated low energy and circulation (Fig. 1).
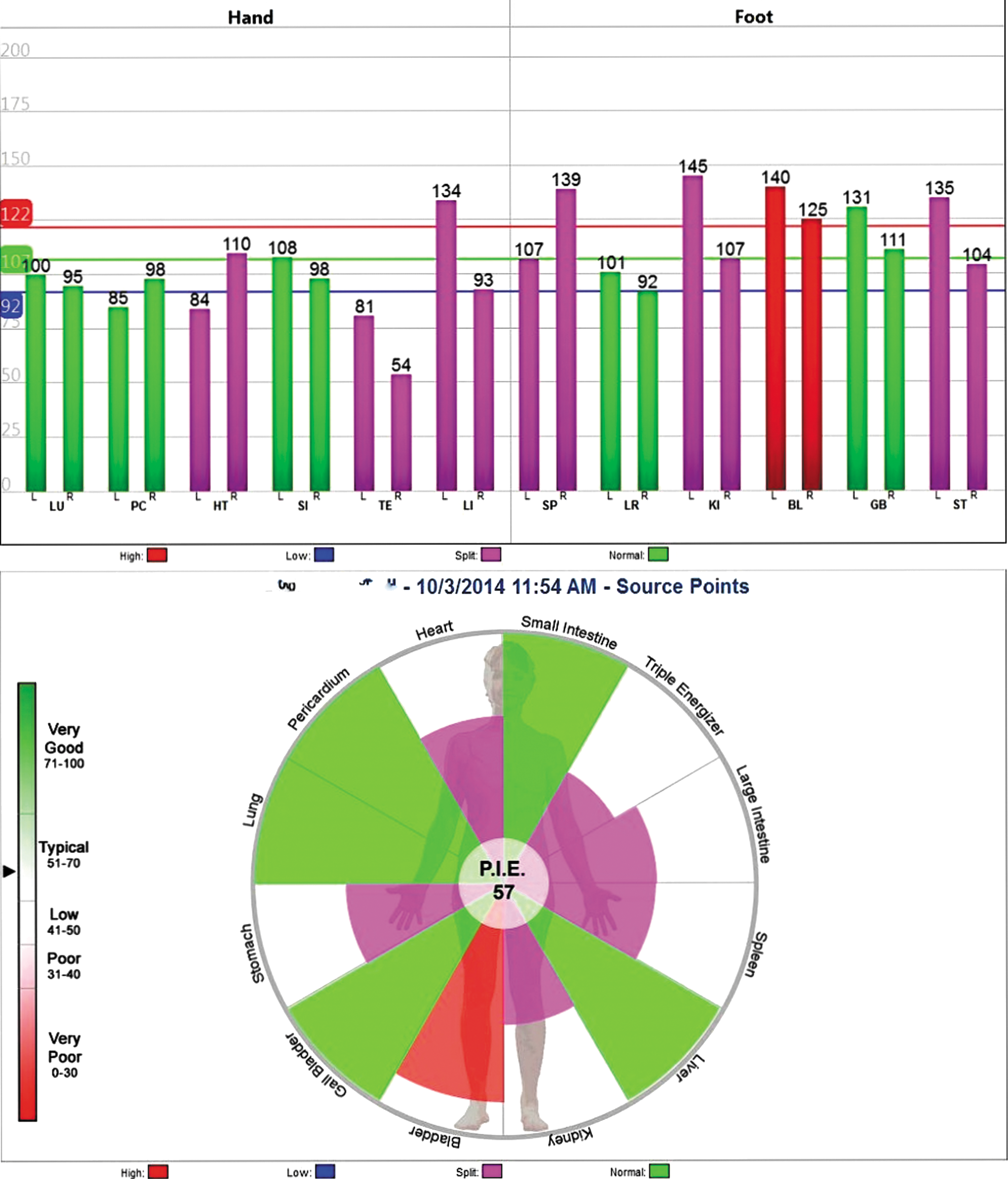
AcuGraph reading taken on first visit. Note that the most obstructed meridian is the Bladder, which follows along the erector spinatus muscles. P.I.E., Personal Integrated Energetics graph; it provides a snapshot of the patient's overall meridian balance. Color images available online at
Because of the poor muscle tone and tendency toward loose stool, the patient was diagnosed with the Traditional Chinese Medicine (TCM) pattern of constitutional Spleen qi deficiency. For the initial visit, the fever was diagnosed as an acute Wind Heat Invasion. Furthermore, the pale and flabby tongue, tendency toward being cold, and weak pulse indicated a yang deficiency. Her thin stature, weak muscle tone, and the fact that the constipation began in infancy indicated a Kidney and Essence deficiency as well.
Treatment
The patient received a total of eight treatments during a 3-month period. In an effort to keep stress on the child as low as possible (thus not adding to any psychological distress already experienced with encopresis), needles were not used if the child was unwilling but were offered every visit. Therefore, acupuncture needles were used only on the first three visits. Acupuncture needles were 0.5-inch, 40-gauage Seirin needles, used with quick insertion, manipulation using the even method, and withdrawal of the needle within 30–60 seconds. If needles were not chosen by the patient, the alternative treatment was using the Pointer Plus device (Mayfair Medical Supplies, Kowloon, Hong Kong), with electrical stimulation of 10 Hz. Pointer Plus points were chosen by running the Pointer Plus device along the LI, SP, BL, KI, and LR channels and selecting any point emitting a charge on the device. Thirty to 60 seconds of “sedation” was implemented at each active point.
A massage technique called tui na was used every other visit on the legs and abdomen and on the last visit on the neck and back. See Table 1 for full description of the modalities used during treatments.
BL, Bladder; KID, Kidney channel; LI, Large Intestine channel; SP, Spleen channel; ST, Stomach channel.
Outcomes and Results
The primary focus of the first treatment was to do a full examination, introduce the child to the process of acupuncture, and relieve the fever. The patient was going to be departing on a family vacation, so no herbs were prescribed this visit; it was agreed to return in 1 month. The following visit, 4 weeks after the initial visit, the patient's mother reported that the child's mood had been more “even-tempered” and that she had had no fecal accidents the first week after the initial treatment. The patient was prescribed a golden flower Chinese herb tablet formula called Ginseng and Longan (gui pi tang), with a dosage of one tablet twice per day.
By the fifth acupuncture session, there was much improvement. The patient had had no fecal incontinence episodes since the last treatment; however, she had not had a bowel movement in 3 days, so the mother used a suppository again the night before. The mother reported that the patient had been rather emotional that week. This time the patient was prescribed the blue poppy liquid formulas Dry Nites and Peaceful Focus, two droppersful of each formula twice per day. The child had been inconsistent in taking the tablet formula because of its taste, so the goal with the liquid formulas was to more strongly address the emotional component while simultaneously improving adherence by choosing a formula with a better taste. The mother was also given dietary instructions to eliminate sugar and dairy from the child's diet.
The most substantial change occurred by the sixth acupuncture visit. Although there had been one fecal accident 4 days prior, the child was taking her herbs regularly, and had had one bowel movement (solid stool type 2 on the mBSFS-C) on her own without parental intervention later the same day after the accident. This was the first time in many months that the child had been willing to use the toilet on her own accord and had had a solid stool. The mother also reported that the child was “more even-keeled” that week.
Two weeks later, on the seventh visit, the patient had been having regular bowel movements on her own every 1–2 days and had had no fecal accidents. Examination showed that the abdomen was soft to palpation. There was a slight atlas rotation from left to right, which was addressed using massage.
At the final visit, the patient had not needed laxatives for over 2 months or needed a suppository in 9 weeks. More important, she was again aware of the need to evacuate her bowels and was willing to use the toilet on her own. There had been no fecal accidents in 7 weeks; therefore, the prognosis of this patient seems to be good.
Discussion
At the fifth acupuncture visit this patient began to see substantial relief from constipation. This seems to correspond with Broide and colleagues' study on chronic constipation, 5 indicating that treatment dosage and frequency is an important aspect to treatment success. It appears that the key to treating fecal incontinence is by primarily treating constipation, as most studies on childhood encopresis link the two conditions. 1,2,4,5,8,9,11 The author initially assumed that the child's hyperactivity and sensitive temperament were separate issues from the constipation/encopresis; however, it became clear during treatment that as the physical component responded, so too did the emotional component, and vice versa. This observation is supported in the literature.
Several studies have linked constipation and encopresis with emotional disorders, most specifically ADHD. 1,11 Although this patient was not officially diagnosed with ADHD, she was hyper upon each interaction, and the mother reported significant emotional instability. The emotional component improved simultaneously with the resolution of constipation/fecal incontinence with this patient. From a TCM perspective, emotions and physical symptoms are closely linked and not separated as disparate components. This mind–body integration could be of great value in the future treatment of encopresis, and further research on integrated approaches to childhood constipation is warranted.
Conclusion
Although much has been written on encopresis, the cure rate and level of improvement with standard care vary and have been reported to be as low as 40%–50%. 4,7,8,10 In addition, evidence suggests that chronic constipation in childhood can result in constipation in adolescence and adulthood, resulting in 2.5 million physician visits annually in the United States. 12 The long-term psychological effects of the shame and social unacceptability of fecal soiling have not been researched. There is some evidence that perhaps some of the treatment options for encopresis, specifically enemas, can lead to emotional frustration and anger repression, which could further complicate encopresis in the long term. 11
This case report adheres to the Jenicek criteria to justify the clinical relevance of a case study, and it demonstrates a mind–body connection when treating functional gastrointestinal disorders in childhood. The literature establishes that fecal incontinence can lead to long-term social and emotional repercussions, and more research on these themes is needed. TCM may be a potential effective treatment plan that can treat both the physical and emotional components of constipation and encopresis. More research to confirm these hypotheses is warranted.
Footnotes
Author Disclosure Statement
No competing financial interests exist.