
Abstract
Objective:
Transcutaneous electrical nerve stimulation (TENS) has been widely used for pain relief; however, the effect remains controversial. The authors hypothesized that TENS can relieve acute pain. Therefore, a single-blinded, randomized, controlled preliminary study was designed on postoperative pain in patients with Colles' fracture.
Methods:
In total, 36 patients were assigned to a real TENS or sham TENS group (18 patients in each group). TENS (50 Hz, 15 min/day) was applied near the Quchi (LI11) and Waiguan (TE5) surfaces of the operative side continuously for 5 days after surgical treatment.
Results:
The visual analog scale (VAS) scores did not differ significantly between the real and sham TENS groups before the TENS period, from the first to fifth day after surgical treatment (all p > 0.05), whereas the VAS scores were lower for the real TENS group than for the sham TENS group in the post-TENS period, on the first, third, fourth, and fifth days after surgical treatment (all p ≤ 0.01).
Conclusion:
TENS might be valuable as a treatment of postoperative pain, but clinicians and researchers should know that it is no different than a treatment with placebo. Especially, since this form of treatment and sham treatment has a great chance of working under the mechanism of the placebo effect due to its single-blindedness.
Introduction
C
Transcutaneous electrical nerve stimulation (TENS) is a pain control method that involves applying electrical stimulation to the skin. Although TENS has been widely used to treat chronic pain or acute postoperative pain because it is a noninvasive and easy-to-use modality, the efficacy remains unclear. 15 Therefore, this study designed a preliminary, randomized controlled trial to investigate the effect of TENS on postoperative pain in patients with Colles' fracture.
Materials and Methods
Subjects
Patients who were suffering from closed displaced Colles' fracture and required surgical treatment were recruited from the Department of Surgery, Yuanli Lee's General Hospital, Lee's Medical Corporation, Miaoli County, Taiwan, between June 16, 2009 and June 15, 2011. The protocol of the trial was approved by the Institutional Review Board of China Medical University Hospital, Taichung city, Taiwan (IRM: DMR98-IRB-102), and written informed consent was obtained from all the participants before the trial. The trial procedures complied with the ethical principles dictated in the Declaration of Helsinki.
The inclusion criteria in the present study were as follows: (1) age ranging from 20 to 80 years; (2) female or male; (3) no patient-controlled analgesia (PCA) experience; and (4) the subjects or their legal representatives should have signed the informed consent. The exclusion criteria were as follows: (1) open Colles' fracture; (2) neurovascular injuries; (3) pregnancy or lactation; (4) severe arrhythmia or the use of heart pacemaker equipment; (5) epilepsy history; (6) severe medical disease such as uremia, decompensated liver cirrhosis, and cancer; (7) psychosis unable to cooperate; and (8) TENS experience.
Design and randomization
This study was a single-blinded, randomized, controlled preliminary study. The randomization was obtained using computer-generated codes. Patients were randomly assigned to the real or sham TENS group using the closed envelope technique.
Sample size
The sample size was calculated according to the preliminary study, with at least 17 patients in each group, if a 95% confidence interval with a power of 85% was used for the analysis. The authors hypothesized that the dropout rate was 5% because the trial was for only 5 days and the subjects were inpatients; therefore, the trial required 18 patients.
Procedure of the trial and groupings
The patients underwent surgical treatment under general anesthetics and they were sent to the recovery room after the completion of the surgical treatment. All the patients received an intravenous (IV) administration of keto (30 mg) as one type of nonsteroidal anti-inflammatory drug (NSAID), after which they were sent back to the ward if vital signs were stable and consciousness was clear. The TENS treatment started 4–6 h after the patient was sent to the ward.
The patients were randomly divided into a real or sham TENS group after the completion of the surgical treatment on the basis of the following: (1) the real TENS group, the adhesive electrodes of the TENS were placed near the Quchi (LI11) and Waiguan (TE5) surfaces of the operative side. The TENS (TENS stimulator, HC-0501; Hometech, Taipei City, Taiwan) had a frequency of 50 Hz, and the intensity of stimulus was just enough to induce a visual muscle twitch of 15-min duration each time per day and continuously for 5 days; and (2) the sham TENS group, the method was identical to that of the real TENS group; however, no electrical stimulus was applied. The position of electrodes was based on the principle of selection of adjacent and local points in traditional Chinese medicine (Fig. 1).

Two adhesive electrodes placed at the dorsal site of the wrists (near TE5) and lateral epicondyle of the elbows (near LI11). In the real TENS group, the patients received high-frequency (50 Hz) electrical stimulation for 15 min per day during 5 days of hospitalization. In the sham TENS group, no electrical stimulation was applied. TENS, transcutaneous electrical nerve stimulation.
Assessment
All the patients routinely received oral Cataflam (75 mg per day) as one type of NSAID. In addition, if the patients could not tolerate the pain, another IV administration of keto or another Cataflam was given. The visual analog scale (VAS) scores, heart rate (HR), and BP were assessed before TENS (before the TENS period) and 5 min after completion of the TENS treatment (post-TENS period) every day for 5 days continuously during admission. Total dose of PCA (morphine 40 mg, keto 60 mg, and butyrophenonel 2.5 mg were added to normal saline to produce 80 mL), number of times of vomiting, and total use of Cataflam were recorded for 5 days after the surgical treatment. The assessment was performed by a well-trained experienced nurse who was blind to the groups.
Primary outcome measures were VAS scores and the total dose of PCA. Secondary outcome measures were the total dose of Cataflam and the total number of times of vomiting.
Statistical analysis
All the baseline data of patients, VAS scores, BP and HR, total dose, number of times of PCA administration and the first time PCA administration was required, total dose of NSAID, number of times of nausea and vomiting, and number of patients were analyzed using independent t tests. The VAS scores from preoperation and postoperation between the real TENS group and sham TENS group for 5 days continuously during TENS admission were analyzed using a repeated measure analysis of variance (ANOVA) with two within factors, day and pre-/post-time, and one between subjects factor, treatment group. The authors defined p < 0.05 to represent significant differences in this study.
Results
Basic characteristic data
In total, 101 patients had closed displaced Colles' fracture and underwent surgical treatment. Sixty-five patients were excluded because of the following reasons: (1) 15 patients were older than 80 years, and 8 patients were younger than 20 years; (2) 12 patients refused to participate in the trial; (3) 8 patients had severe medical disorders; (4) 9 patients refused PAC use; and (5) 13 patients experienced TENS. Therefore, in total, 36 patients were included in the trial and they were randomly assigned to the sham (18 patients) or real TENS group (18 patients). All the patients completed the trial (Fig. 2).
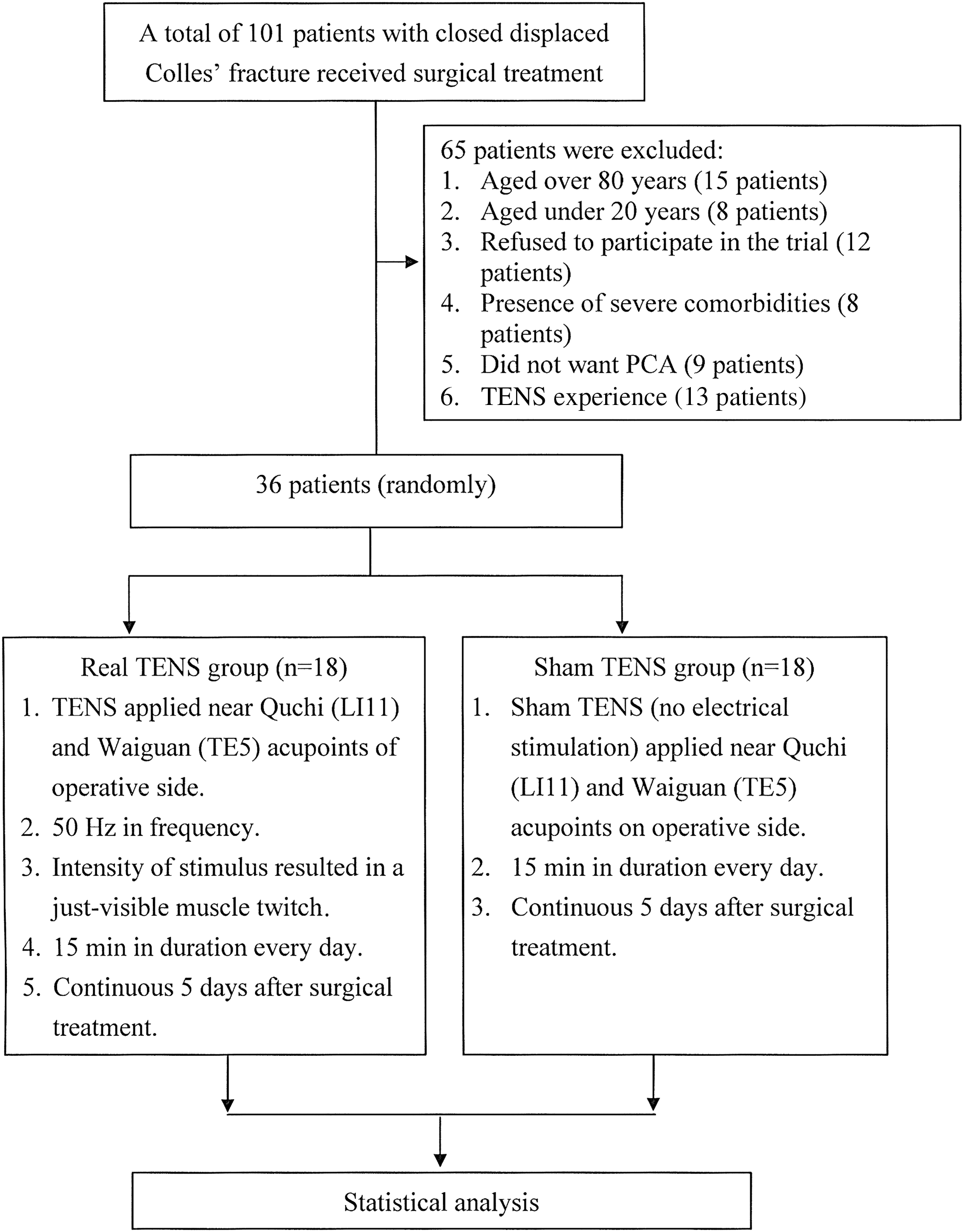
Flowchart. PCA, patient-controlled analgesia.
Basic characteristic data included age, body weight, body height, body–mass index, HR, BP, and VAS scores before and after surgical treatment, which did not differ significantly between the groups (all p > 0.05; Table 1).
The data are represented as mean ± standard deviation.
p < 0.05 compared to VAS(b) for the same patient group.
BP, blood pressure; Real TENS, patients received real TENS; Sham TENS, patients did not receive electrical stimulation from the TENS device; TENS, transcutaneous electrical nerve stimulation; VAS, visual analog scale; VAS(b), score on the VAS presurgery; VAS(p), score on the VAS postsurgery.
Effect of TENS on primary and secondary outcomes
A repeated measure ANOVA was conducted to compare the VAS scores from preoperation and postoperation identity between the real TENS group and sham TENS group across five time periods (from the first to fifth days). There was a significant interaction between the pre-/post-time and treatment group (p < 0.001). The VAS scores did not differ significantly between the real and sham TENS groups before the TENS period, from the first to fifth day after the surgical treatment (the estimated mean VAS standard error [SE] were 3.79 (0.20) and 3.67 (0.20) for the sham TENS group and real TENS group, respectively, p = 0.66). After TENS, there was no significant interaction between the treatment group and time (Wilks' Lambda = 0.809, F = 1.831, p = 0.148). There was a significant main effect for time (Wilks' Lambda = 0.238, F = 24.755, p < 0.001, partial Eta squared = 0.762), with both groups of treatment showing a decrease in VAS scores across the five time points (the first to fifth days). The main effect of comparing the two groups of treatment was significant (F = 11.243, p = 0.002, partial Eta squared = 0.248), suggesting there was a significant difference in VAS score between the real TENS group and sham TENS group (Fig. 3).
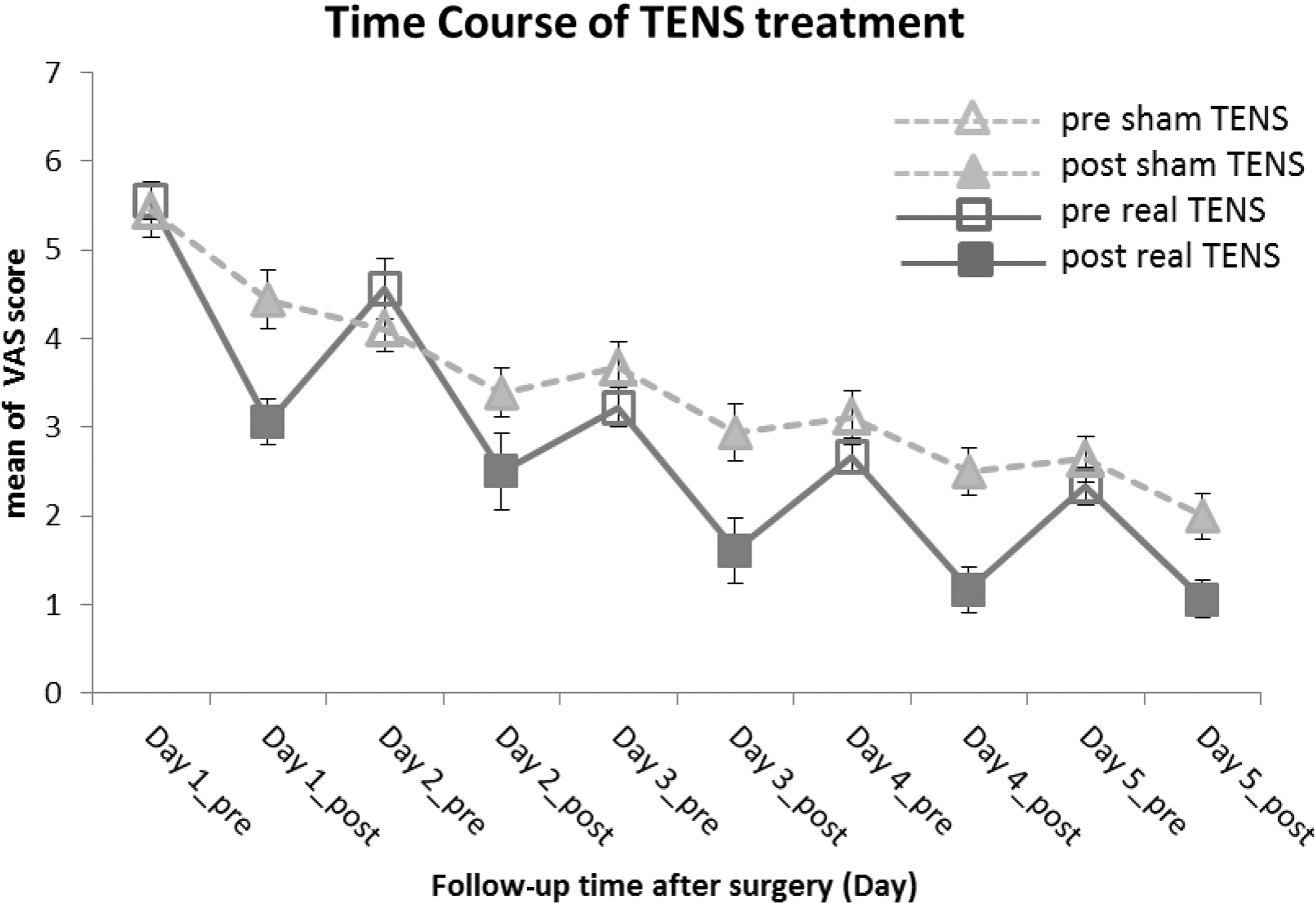
The effect of TENS on visual analog scale (VAS) scores. The VAS scores of the two groups did not differ significantly before TENS treatment; however, the VAS scores of two groups differed significantly (p = 0.002) after TENS treatment. Also, a significant time effect was observed (p < 0.001).
The total dose of PCA did not differ significantly between the groups for 5 days after surgical operation (p > 0.05; Table 2).
Data are represented as mean ± standard deviation or number (%).
Cataflam, total tablets of Cataflam; Keto, total number of intravenous injections of Keto; PCA, total dose of patient-controlled analgesia; Vomiting (number), number of patients in the group who vomited; Vomiting (times), total incidences of vomiting in the patient group.
Secondary outcomes, including the total number of keto injections, total dose of Cataflam, and total number of times of vomiting did not differ significantly between the two groups for 5 days after the surgical treatment (all p > 0.05; Table 2).
Discussion
The results of this study indicate that the VAS scores were lower in the real TENS group than in the sham TENS group during the post-TENS period, whereas the scores were similar for the two groups during the pre-TENS period after the surgical treatment in patients with Colles' fracture. In addition, the total dose of PCA, total number of keto injections, total dose of Cataflam, and number of times of vomiting did not differ significantly between the real and sham TENS groups. Therefore, the authors suggest that TENS can reduce postoperative pain immediately; however, this effect of TENS is transient and cannot be maintained for 24 h. In addition, TENS treatment could not reduce the total dose of PCA, keto injection, and Cataflam and the number of times of vomiting. However, the results could not exclude the placebo effect of TENS treatment due to the present study that was a single-blinded design, which easily produced a bias.
Numerous studies have considered TENS a noninvasive method of analgesia, such as for pain relief in the first stage of labor, 16 for reducing operative pain in patients with laparoscopic sterilization, 17 the demand of postoperative opioid in patients with spinal surgery, 18 and analgesics of postoperative pain. 19 In sum, the aforementioned reports conclude that TENS reduces pain, mainly acute pain, especially postoperative pain. This conclusion is consistent with the results of this study. By contrast, several reports have indicated that TENS cannot significantly provide relief from chronic pain. 17,20,21 Several researchers have suggested that the reducing pain mechanism of TENS is possibly mediated through the increase in endorphins or reduction in the release of substance P. 22 –24 Electroacupuncture increases the concentration of β-endophin in the blood and brain in the mouse cancer pain model. 24 Moreover, electroacupuncture increases the β-endophin levels and reduces cortisol levels in plasma in patients with osteoarthritis. 22 The rapid catabolism of endorphins may explain the transient effect of TENS on pain relief. 25,26 According to the theory of gate control, pain relief may be achieved by inhibiting the nociceptive C-fiber through the stimulation of the afferent A-fiber in the dorsal column of the spinal cord. 27 The authors assume that the inhibition of the nociceptive C-fiber requires continuous TENS stimulation to evoke the activity of the afferent A-fiber. Therefore, the effect of pain relief decreases or even disappears when TENS stimulation is stopped. This suggestion may partly explain the results of this study.
This study has several limitations: (1) the sample size was extremely small; (2) the duration of TENS stimulation was short; and (3) TENS can be set at a frequency of only 50 Hz, and the other parameters, such as intensity and the duration of stimulus, possibly affect the analgesic effect of TENS. 19,28,29 Therefore, ways of stimulating the pain-relieving effect of TENS must be studied further.
In conclusion, TENS might be valuable as a treatment of postoperative pain, but clinicians and researchers should know that it is no different than a treatment with placebo. Especially, since this form of treatment and sham treatment has a great chance of working under the mechanism of the placebo effect due to its single-blindedness.
Footnotes
Acknowledgments
This study was supported by the China Medical University under the Aim for Top University Plan of the Ministry of Education, Taiwan, and the Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW104-TDU-B-212-113002).
Contributors
C.-H.L. performed the experiment and wrote the paper; T.-Y.L. participated in the experiment and discussion; J.-S.H. participated in the discussion; W.L.L. performed the statistical analysis; and C.-L.H. participated in the discussion and design and revised the document.
Author Disclosure Statement
No competing financial interests exist.